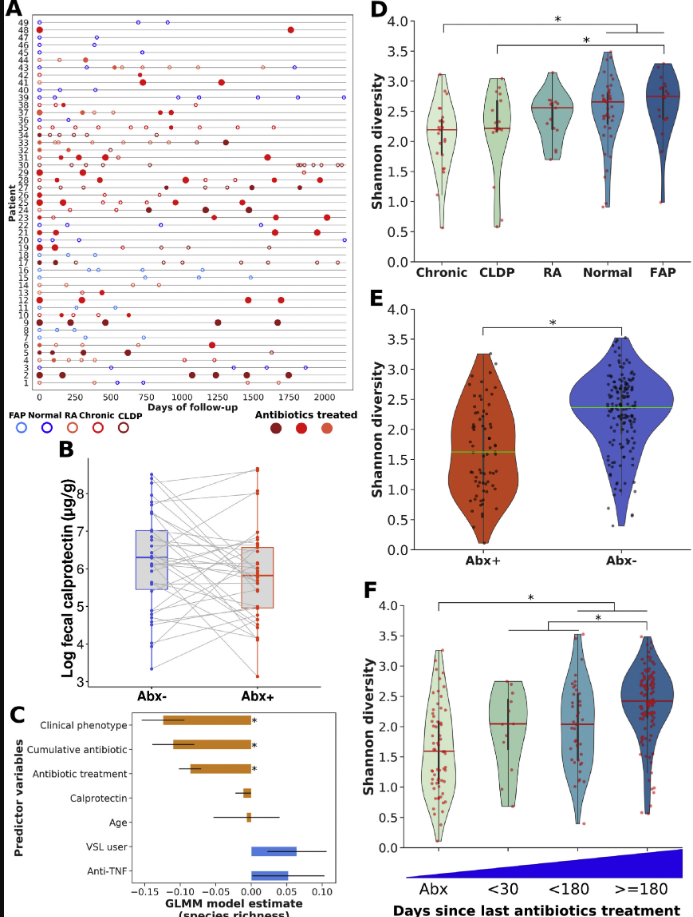
R Pittayanon et al. Gastroenterol 2020; 158: 930-46. In this systematic review of the relationship between gut microbiota and inflammatory bowel disease, 48 studies and 45 articles were included from a total of 2631 citations. Overall, the authors found inconsistent results with differences in the abundances of some bacteria in IBD. My take: These microbiota studies use ‘big data’ to look for abnormal patterns in patients with IBD. Overall, most of these studies support a reduced diversity among patients with IBD. Specific variation in microbes varies widely and remains unclear if they are a cause or a consequence of IBD.
J Piercy et al. JPGN 2020; 70: 318-23. Among 90 adolescents with IBD, “perfectionistic concerns (self-critical and socially prescribed perfectionism) were associated with higher rates of adolescent-reported externalizing symptoms” Thus, perfectionism may help with self-management but lead to more stress and psychosocial symptoms.
S Jardine et al. Gastroenterol 2020; 158: 1000-15. This study used both TTC7A-knockout cells and a zebrafish model to screen compounds that have been FDA approved for treatment of inflammatory bowel disease caused by TTC7A deficiency. The authors identified leflunomide that reduces apotosis and levels of active caspase 3 in TTC-7A-knockout cells and restored gut motility along with improvement of intestinal cell survival in zebrafish. This study has some amazing figures detailing the changes induced by leflunomide. My take: Although some centers have offered hematopoetic stem cell transplant (with dismal results), there is NOT a currently accepted treatment for TTC7A deficiency-induced IBD. This study suggests an agent which may help.
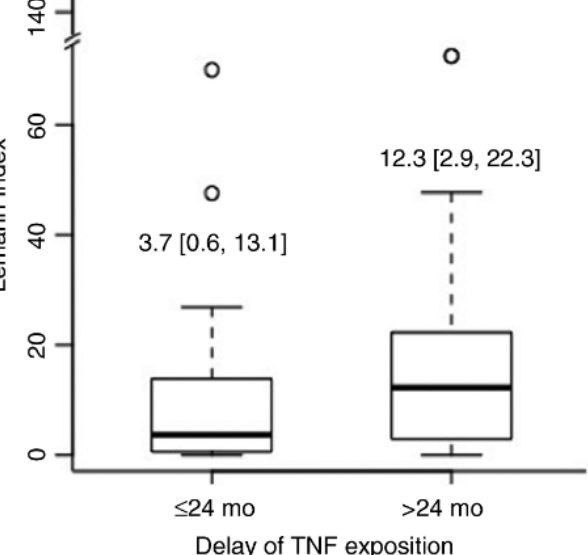
CLD Prevost et al. AP&T 2020. https://doi.org/10.1111/apt.15681 Key finding: Among patients exposed to anti‐TNF, the Lémann Index was lower in those who were exposed in the first 2 years of their disease (P = 0.015). My take: Early treatment with anti-TNF agents can reduce risk of permanent bowel damage. This was seen as well in the RISK study which showed that anti-TNF therapy reduced the development of penetrating disease. (Related post: CCFA Update 2017, Part 3)