The images below show how much more prevalent problems with regurgitation, colic, functional diarrhea, dyschezia, and functional constipation in the first 3 months of life compared to later in the first year of life.



The images below show how much more prevalent problems with regurgitation, colic, functional diarrhea, dyschezia, and functional constipation in the first 3 months of life compared to later in the first year of life.
A recent study (S Salvatore et al. J Pediatr 2019; 212: 44-51) examines the role of neonatal antibiotics and prematurity on the development of functional gastrointestinal disorders in the first year of life.
What is most striking, though, in this study is how many of these infants have a GI disorder.
Background: Prospective cohort multicenter study with 934 infants who completed study; n=302 premature, n=320 antibiotic recipients
Key findings:
Limitation: This study relied on parental reports which could overestimate infant’s symptoms.
My take: More than 75% of infants had at least one FGID.
Related blog posts:

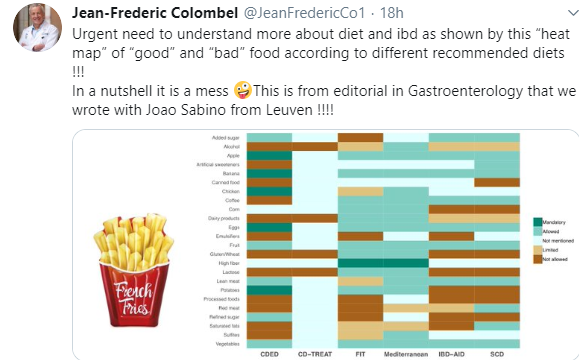
As noted in a previous blog (IBD Briefs August 2019), there have been numerous diets proposed to help with Crohn’s disease. The chart below illustrates the lack of any consensus.
Related blog posts:

A Carroccio et al. Clin Gastroenterol Hepatol 2019; 17: 682-90. This prospective study examined 78 patients with a diagnosis of non-celiac gluten sensitivity (NCGS) based on double-blind wheat challenge. The authors identified markers of inflammation including eosinophils in the duodenum and rectum of patients with NCGS: –the mean eosinophil infiltration was more than 2.5-fold the upper limit of normal in rectum and almost 2-fold in duodenum.
Rectal eosinophilia (>9 eos in the rectal lamina propria) had a sensitivity of 94%, specificity of 70%, positive predictive value of 81% and negative predictive value of 89% for NCGS.
My take: (from the editorial,pg 613-4) “In many cases, NCGS is likely a mislabeled functional GI disorder (IBS or FD) induced by wheat proteins or FODMAPs…tissue eosinophilia [is a] potential biomarker..although this observation needs further confirmation.”

Yummy! Though, probably the wrong place for those trying to be gluten-free
A recent cross-sectional study (LM Little et al. J Pediatr 2019; 210: 141-5) which examined sensory processing and constipaiton included 66 children and 66 control children.
Key finding:
The authors utilized the Child Sensory Profile-2 and the Toileting Habit Profile Questionnaire.
The finding that sensory problems contribute to chronic constipation. In those with over-responsiveness, which was more frequent in this study, this can lead to avoidance behaviors. In under-responsiveness, children may not realized that they need to defecate which can lead to problems as well.
My take: This study suggests that recognition of how sensory problems contribute to chronic constipation could improve counseling/treatment approaches.
Related blog posts:

Salt Creek Falls, OR
A recent study (JL Yasuda et al. JPGN 2019; 69: 163-70) shows that esophagitis is common with and without proton pump inhibitor (PPI) therapy in children with esophageal atresia (EA).
Background: This study encompassed 310 patients (34% long gap EA) and 576 endoscopies (median age 3.7 years)
Key findings:
While this is a large study, the findings have several limitations. This is a single center retrospective study and this center attracts highly complex cases of EA.
My take: In addition to fairly high rates of erosive esophagitis and eosinophilic esophagitis, this study shows a high incidence of microscopic esophagitis, the significance of this is unclear. This study supports the current recommendations of 3 endoscopies in childhood and perhaps more frequent surveillance in those with more complex EA.
Related blog posts:

Sign in Hood River, OR
WE Bennett, MD Pfefferkorn.
Full Link: Editorial: “Mental Health Screening as the Standard of Care in Pediatric Inflammatory Bowel Disease” Thanks to Ben Gold for this reference.
An excerpt:
Butwicka and colleagues1 have published a fascinating, landmark cohort study in this issue of JAMA Pediatricsassessing the prevalence of psychiatric diagnoses and symptoms among children with inflammatory bowel disease (IBD) in Sweden. The authors used a rigorous design that compared a cohort of more than 6000 pediatric patients with IBD with hundreds of thousands of healthy controls, as well as a separate cohort comprising the patients’ own siblings who did not have IBD. Butwicka et al1 computed hazard ratios for any psychiatric disorder, as well as for multiple specific disorders, and found a hazard ratio of 1.6 for any psychiatric diagnosis when comparing children with IBD with healthy controls. The statistical analysis is stellar and represents the best data we currently have on the intersection of pediatric IBD and mental health. Their study highlights a substantial risk in a vulnerable population and should trigger revision of guidelines and allocation of resources to support widespread screening and treatment for these dangerous conditions.
Related Article:
A Butwicka et al.
Full Text Link: Association of Childhood-Onset Inflammatory Bowel Disease With Risk of Psychiatric Disorders and Suicide Attempt
Related blog posts:

Crater Lake, OR
O Courbette et al. JPGN 2019; 69: 189-93. Infliximab Paradoxical Psoriasis in a Cohort of Children With Inflammatory Bowel Disease
From Abstract:
Results: One hundred and twenty-three CD patients and 24 UC patients were treated with IFX. Twenty patients (13.6%) experienced a paradoxical psoriasis. All of them were affected by CD. Perianal CD was more frequent in the psoriasis group (P = 0.033). Fourteen patients (70%) were in remission when skin lesions occurred. Paradoxical psoriasis was diagnosed 355 days (median, interquartile range [IQR] 239; 532) after the initiation of IFX corresponding to the eighth injection (median, IQR: 6; 15). Psoriasis lesions were controlled by local steroids in all cases and no patients discontinued IFX therapy.
Conclusions: 13.6% of our IBD patients treated with IFX developed psoriasis during a median follow-up of 23.9 months (IQR: 11.6; 36.5). Crohn disease patients with perianal disease were at a higher risk to develop this common side effect.

Another large retrospective ‘real-world’ study (C Chen et al. Inflamm Bowel Dis 2019; 1417-27) examined persistence profiles of biologic therapies in newly diagnosed IBD patients. This study, based on Truven Health MarketScan data (2008-2015) included 5612 patients with Crohn’s disease (CD) and 3533 with ulcerative colitis (UC). There were 1156 persons (20.6%) in the pediatric age range (0-18)
Key findings:
Why did combination therapy result in higher medication persistence rates?
Limitation: This study may overestimate drug discontinuation as some patients may simply have had a dosing delay.
My take: This study shows a higher-than-expected rate of drug discontinuation indicating dissatisfaction related to efficacy, cost or complications. Those receiving immunomodulators (combination therapy) were much less likely to discontinue treatment.
Related blog posts:

Wizard Island, Crater Lake, OR
Disclaimer: These blog posts are for educational purposes only. Specific dosing of medications/diets (along with potential adverse effects) should be confirmed by prescribing physician/nutritionist. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition
There is speculation that the use of therapeutic drug monitoring (TDM) may obviate the advantages of combination therapy. However, there is plenty of data supporting combination therapy including a recent retrospective population-based study (LE Targownik et al. Clin Gastroenterol Hepatol 2019; 17: 1788-98).
This ‘real-world’ study (2001-2016) utilized the Manitoba IBD database and included 852 persons with Crohn’s disease (CD) and 303 with ulcerative colitis (UC).
Key findings:
My take: Combination therapy has been associated with higher response rates to IBD therapy. This advantage has to be weighed against potential adverse effects.
Related blog posts:
Disclaimer: These blog posts are for educational purposes only. Specific dosing of medications/diets (along with potential adverse effects) should be confirmed by prescribing physician/nutritionist. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.

Wizard Island. Crater Lake, OR
