In this retrospective study of 41 adults with history of ileal pouch-anal anastomosis (IPAA) for ulcerative colitis (UC), the authors evaluated the clinical response (subjective judgement of provider) to chronic vancomycin therapy (125 mg twice a day).
Key findings:
At 4 weeks, 21 (51%) of patients had a clinical response. 16 of these patients maintained a clinical response at 3 and 6 months (remained on treatment).
6 additional patients demonstrated a later response. In total 22 (54%) were considered clinical responders at 3 and 6 months.
The mean number of antibiotics utilized prior to vancomycin was 4, including ciprofloxacin, metronidazole, levofloxacin, rifaximin, sulamethoxazole-trimetoprim, amoxicillin, and amoxicillin-clavulanic acid
My take: Since vancomycin has poor enteral absorption, it’s side effect profile is very favorable. More prospective and objective data is needed; however, vancomycin’s high cost will likely limit frequent use.
Methods: This was a double-blind, randomized, sham-controlled trial in patients (n=100) with nocturnal symptoms of gastroesophageal reflux. Patients were advised to sleep in the left lateral decubitus position and were assigned randomly (1:1) to an electronic sleep positional therapy wearable device (applied with an adhesive sticker), programmed to either produce a vibration when in the right lateral position (intervention) or only during the first 20 minutes (sham).
Key findings:
In the intention-to-treat analysis, the rate of treatment success (defined as a 50% or more reduction in the nocturnal reflux score) was 44% in the intervention group (22 of 50) vs 24% in the sham group (12 of 50)
There was increased time sleeping in the left lateral decubitus position (intervention 60.9% vs sham 38.5%)
My take: In those with nocturnal heartburn, this appears to be a helpful nonpharmacological tool.
Website for the company (side sleep technologies) that makes the device: The Left ” Your body will be conditioned to sleep at least 80% on your left within a week.” (I do not have any financial relationship with this company).
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
This was a cross-sectional study of caregivers of children (n=34) with intestinal failure receiving long-term parenteral nutrition. 97% of caregivers were the child’s mother and median duration of providing care among respondents was 3.4 years.
Key findings:
Caregivers reported a median of 29.2 hours per week (IQR, 20.8-45.7 hours per week) of direct medical care. 6.1 hours was spent on providing PN and care of the central venous catheter. 6.3 hours was spent on enteral nutrition and enteral tube care.
In the associated editorial (pgs 10-12 by S Mauskar, JG Berry. Open Access! “Failing to Support Families’ Burden of Care for Children with Intestinal Failure“), the authors note that in the U.S. there has been a growing population of children at home with greater medical complexity and reliance on medical technology and that the need for home nursing support “greatly exceeds the supply, leaving many families on their own to care for their children.”
They also note that the medical literature (over the last 25 years) on caregiver burden for children notes it is associated with “marital discord, loss of employment, and financial struggle…In the U.S. a substantial portion of children with medical complexity assisted with technology live in single-parent households, in poverty, and are exposed to adverse childhood events…very vulnerable to the effects of high caregiving burden.”
My take: This study shows that while we have an effective treatment for intestinal failure, the burden of this treatment is very high even with care coordination and social worker help. Understanding this burden could help medical providers be more empathetic for the family who is struggling with home medical care (eg. child with recurrent admissions for central line infections).
Methods: In patients (n=99) with Rome IV–defined non-constipated IBS, outcomes after randomization to one of three diets were compared. The “traditional dietary advice” group: “Its principles include adopting healthy, sensible eating patterns such as having regular meals, never eating too little/too much, maintaining adequate hydration, and reducing the intake of (1) alcohol/caffeine/fizzy drinks, (2) fatty/spicy/processed foods, (3) fresh fruit to a maximum of 3 per day, (4) fiber and other commonly consumed gas-producing foods (eg, beans, bread, sweeteners, etc), and (5) addressing any perceived food intolerances (eg, dairy).” (Link: National Institute for Health and Care Excellenceadvice on IBS mgt). The Gluten-Free diet allowed for cross-contamination. All patients had specialist dietary counseling.
Key findings:
All three diets resulted in improvement. The primary end point of ≥50-point reduction in IBS-SSS was met by 42% (n = 14/33) undertaking TDA, 55% (n = 18/33) for LFD, and 58% (n = 19/33) for GFD (P = .43)
Alterations in stool dysbiosis index were similar across the diets, with 22%–29% showing reduced dysbiosis
“The pragmatic study design, whereby the responsibility was left on patients to undertake the diets following appropriate education, means our findings can be generalized”
My take: All three diet approaches would be appropriate to reduce IBS symptoms, thought the TDA is the easiest for patients.
Why does Mississippi have the best childhood immunization rates (99%)? This is due to state policies. This article reviews the small but significant drops in childhood immunizations which is opening the door for highly contagious diseases like measles.
Some excerpts:
U.S. routine childhood vaccination rates have historically been among the world’s best. But within the first year of the pandemic, the nation’s children missed nine million vaccine doses for diseases like polio and measles. Rates for the three major childhood immunizations — for measles, mumps and rubella; chickenpox; and diphtheria, tetanus and pertussis — fell by an average of 1.3 percentage points, with the rates in seven states and many cities falling under 90 percent…
Measles should not be taken lightly. The virus is highly contagious; according to the C.D.C., if one person has it, up to 90 percent of the people close to that person who are not immune will also become infected. It can live up to two hours in the air. One to three of every 1,000 children who contract measles die of respiratory and neurological complications…
Covid vaccine acceptance and anti-vax attitudes do not fully explain differences among states. Neither do red-blue partisan affiliations or the strength of a state’s public health system. Instead, the decline is rooted in longstanding policies among some states that allow, for instance, for nonmedical exemptions, failures to rigorously enforce vaccination requirements and inadequate public health campaigns…
Vaccines are one of the few true cost savers in medicine. The routine immunizations of children born from 1994 to 2018 are projected to prevent nearly one million early deaths and save nearly $1.9 trillion in economic costs — more than $5,700 for each American, according to the C.D.C. For measles, a state might spend more than $2 million responding to a single outbreak, with each case costing nearly $50,000 on average, according to an analysis of a recent outbreak in Washington State.
To avoid dangerous and costly outbreaks, states should introduce enforceable solutions that give their children and communities the best protections against vaccine-preventable infectious diseases.
Recommendation 5: Despite the presence of gastric polyps in children, and the later risk of duodenal polyposis and ampullary cancer in adult practice, there is no justification to commence routine UGI surveillance until the age of 25 years. (weak recommendation, low-quality evidence, consensus agreement 90%)
Methods: A prospective record of all upper GI endoscopies in children (aged 9 to 17) with FAP was kept across a 12-year period
Key finding:
Thirty-eight esophagogastroduodenoscopies (79%) identified at least 1 gastric or duodenal polyp in 22 (79%) patients; 10 (36%) patients had gastric adenomas
Eight (29%) patients showed very high numbers of polyps
All 21 patients who had duodenal polyps had adenomas
No patients had malignancy
My take: This is a provocative study. Is there a benefit for the patient in identifying gastric/duodenal polyps at a younger age?
This article recommends medical schools stop participating in U.S. News & World Report’s (USNWR) ‘best medical school’ survey. I would advocate for eliminating USNWR’s reports more broadly including their ranking of hospitals and medical specialties.
The medical school rankings rely on the following:
Federal research dollars
Reputation – “assessed by a survey (with an abysmal response rate) of medical school deans, department chairs, and residency program directors”
Ratio of full-time faculty to students
Students’ median scores on the Medical College Admission Test and their undergraduate grade-point averages
Acceptance rate
Some excerpts:
“Yale and Harvard Law Schools recently announced they would no longer participate in U.S. News & World Report’s (USNWR) flawed ranking system, followed closely by additional schools. The nation’s medical schools need to follow their lead. Why? The USNWR ranking system is in direct opposition to medical schools’ goal of educating a well-trained, diverse, and culturally competent medical workforce..”
“It is hardly a secret among medical school deans that the USNWR rankings are based on data not directly related to educational process, quality, and outcomes. Nor can they trust the veracity of the data that are provided, given the recent scandals reported in other professional schools and colleges that manipulate the formula to their own advantage.”
“Comprehensive analyses of USNWR rankings have long demonstrated that the methodology is ill-conceived, that the response rate of those completing the questionnaires that feed into the ranking formula would not meet the standards of a peer-reviewed publication, and that the most important aspects of educational quality are largely ignored.”
“There is peer pressure to stay within the system and to compete for the top prize because it feels good to see your school on top, no matter how flawed the measuring stick.”
My take: It is difficult to measure quality. I do not trust USNWR’s rankings with regard to “best” medical school, “best” hospital or “best” subspecialty. I think medical care would be better off without these reports. Another option would be to focus on reporting hard data, rather than the current aggregate format. This data could include federal research dollars and reputational surveys; the latter would need to be transparent with regard to methodology.
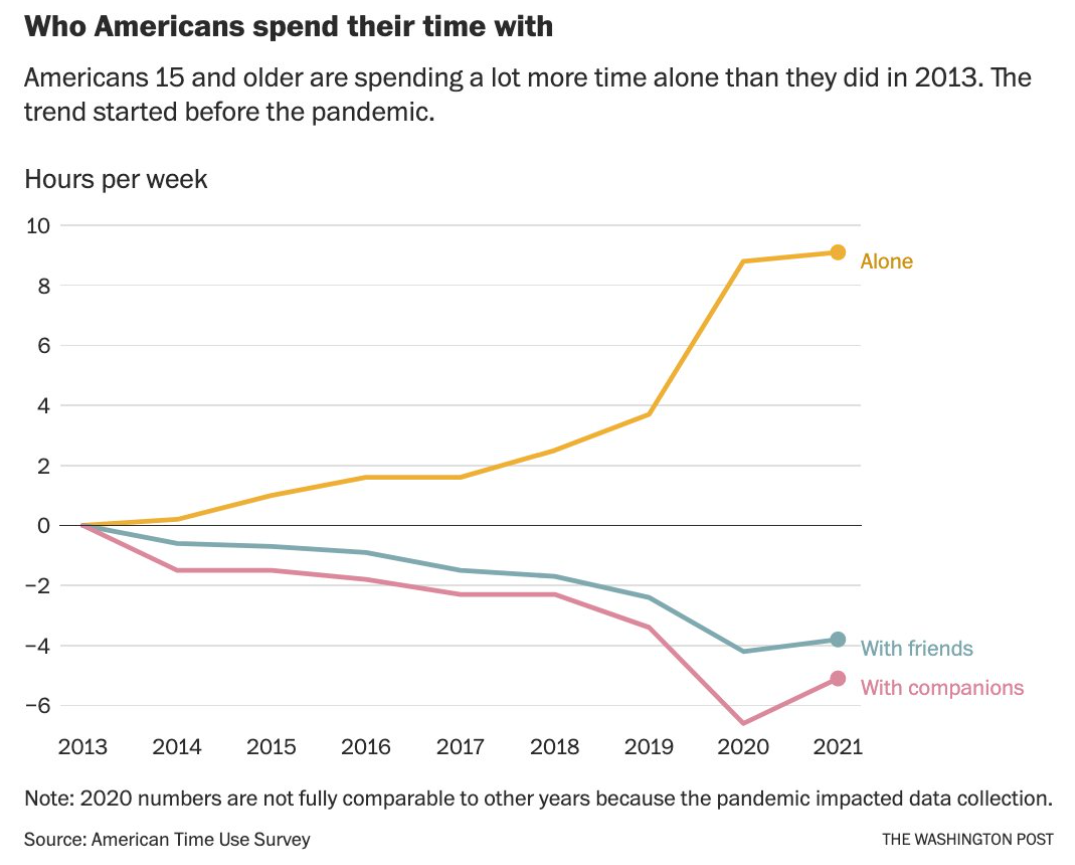
From TheWashington Post, 11/23/22. Opinion Americans are choosing to be alone. Here’s why we should reverse that. “Spending less time with friends is not a best practice by most standards, and it might contribute to other troubling social trends — isolation, worsening mental health (particularly among adolescents), rising aggressive behavior and violent crime. “
As noted previously, in my view, “bad” inflammatory bowel disease (IBD) occurs when treatments are not working; though, many would argue that any IBD is bad IBD. Today’s post concludes several reviewed articles that focus on the problem of IBD that is not responding well to treatment.
Methods: Seventeen steroid-resistant adult UC patients were treated with cyclosporine in combination with vedolizumab, with a follow up of 52 weeks. Only 2 patients in this chort had failed infliximab therapy. The authors administered IV cyclosporine at a dose of “2 to 4 mg/kg/d IV for 7 days, titrated to a goal trough level of 300 to 400 ng/mL.” In those with a response, patients were started on oral therapy along with IV vedolizumab. During oral therapy (for 8 weeks), goal trough levels were 150 to 250 ng/mL (measured weekly).
Key findings:
Fifteen (88%) of 17 patients initially responded to cyclosporine and were started on vedolizumab
At week 10, 11 (73%) of 15 patients had achieved endoscopic remission with a Mayo score of ≤1.
At week 26, 14 (93%) of 15 of the patients were in clinical remission and 11 (73%) were in endoscopic remission.
At week 52 of follow-up, 10 (71%) of 14 of these patients continued to be in endoscopic remission and 11 (79%) of 14 were in clinical remission.
Colectomy-free survival rate was 82% (n = 14 of 17) at 1 year and mean C-reactive protein, erythrocyte sedimentation rate, and fecal calprotectin levels were 3.2 mg/L, 16.1 mm/h, and 168.3 µg/g, respectively
My take: Cyclosporine is a fast-acting medication and thus appropriate as a salvage therapy in those with severe disease. Concerns for adverse effects have led most pediatric GIs to favor infliximab for refractory severe UC. However, in selected patients, it could be a useful “bridge” to slower-acting long-term treatments. It is possible (likely) that insurance issues would be less with cyclosporine than tofacitinib as a bridge therapy.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
Island Ford National Recreational Area, Sandy Springs GA
As noted yesterday, in my view, “bad” inflammatory bowel disease (IBD) occurs when treatments are not working; though, many would argue that any IBD is bad IBD. Over the next few days, reviewed articles will focus on the problem of IBD that is not responding well to treatment. This article reports on the use of tofacitinib to avoid colectomy in children with severe ulcerative colitis.
This small (n=11) retrospective single-center cohort study of consecutive hospitalized pediatric patients initiating tofacitinib for refractory ulcerative colitis from 2018 to 2021. All patients demonstrated nonresponse to both intravenous corticosteroids and anti-TNF therapy prior to tofacitinib initiation.
Key findings:
Eight of 11 patients remained colectomy-free at 90 days following hospital admission and 6 remained colectomy-free over median 182-day follow-up, including 4 of whom remained on tofacitinib
The authors note that three patients started with TID dosing and eight received BID dosing (10 mg per dose). The higher dosing was influenced by a case control study by Bernstein et al which showed a 15% 90-day colectomy rate among adults with acute severe ulcerative colitis (ASUC), particularly those dosed at TID (Open Access: Clin Gastroenterol Hepatol 2021; 19: 2112-2120. Tofacitinib for Biologic-Experienced Hospitalized Patients With Acute Severe Ulcerative Colitis: A Retrospective Case-Control Study)
“Remission rates peaked at 12-16 weeks and decreased at 6 months…tofacitinib may …bridge to slower-acting and possibly safer long-term therapies such as ustekinumab or vedolizumab”
The median time to corticosteroid discontinuation was 89 days
No serious tofacitinib-related adverse events were observed
My take: Given the small numbers, this is clearly an area where cooperation (& ImproveCareNow) could be helpful in determining the safety and effectiveness of tofacitinib for pediatric ASUC. Also, if tofacitinib is used as a ‘bridge’ this is likely to present insurance coverage issues.
Related article:
Hoisnard L, Pina Vegas L, Dray-Spira R, et al. Annals of the Rheumatic Diseases Published Online First: 05 October 2022. doi: 10.1136/ard-2022-222824. Risk of major adverse cardiovascular and venous thromboembolism events in patients with rheumatoid arthritis exposed to JAK inhibitors versus adalimumab: a nationwide cohort study Methods: This was a nationwide population-based cohort study (n=15,835) of the French national health data system, the exposed group initiating a JAKi and non-exposed group initiating adalimumab Key findings: Risk of major adverse cardiovascular events (MACEs) for the exposed versus non-exposed group was not significant: HRw 1.0 (95% CI 0.7 to 1.5) (p=0.99), nor was risk of VTEs significant: HRw 1.1 (0.7 to 1.6) (p=0.63). This study provides reassuring data regarding the risks of MACEs and VTEs in patients initiating a JAKi versus adalimumab, including patients at high risk of cardiovascular diseases.
Generally, in my view, “bad” inflammatory bowel disease (IBD) occurs when treatments are not working; though, many would argue that any IBD is bad IBD. Over the next few days, reviewed articles will focus on the problem of IBD that is not responding well to treatment.
In this retrospective study with 69 children with Crohn’s disease (CD) from 25 centers, the authors looked at the effectiveness of ustekinumab (UST) dose escalation which entailed reducing frequency to less than every 8 weeks. Most children were biologic (98.6%)- and immunomodulator (86.8%)- experienced.
Key findings:
Clinical response and remission were observed at 3 months after UST escalation in 46 (67%) and 29 (42%) children, respectively.
Fecal calprotectin level from 1100 (500–2300) to 515 (250–1469) µg/g (P = 0.012) 3 months post-escalation
Endoscopic and transmural healing were achieved in 3 of 19 (16%) and 2 of 15 (13%) patients, respectively
In their discussion, the authors note that UST has not received FDA approval despite the fact that it has become a common second- and third-line biologic therapy for pediatric CD.
My take: This study supports the common practice of escalation of UST for children with active CD despite treatment at every 8 weeks.
Related Ustekinumab Studies:
J Meserve et al.Clin Gastroenterol Hepatol 2022; 20: 2728-2740. Open Access! Effectiveness of Reinduction and/or Dose Escalation of Ustekinumab in Crohn’s Disease: A Systematic Review and Meta-analysis In this article with 15 cohort studies in 925 adults with CD with inadequate response or loss of response to standard dose ustekinumab, on meta-analysis, 55% of patients achieved clinical response [with dose escalation]…61% of patients were able to achieve endoscopic response, including 29% who achieved endoscopic remission. Dose interval shortening alone recaptured response in 57% patients.
RS Dalal et al. Clin Gastroenterol Hepatol 2022; 20: 2399-2401. Predictors and Outcomes of Ustekinumab Dose Intensification in Ulcerative Colitis: A Multicenter Cohort Study This retrospective study looked at 108 adult patients with UC who had ustekinumab escalation; more than 40% required dose intensification. “Similar to our findings in Crohn’s disease, >50% of dose-intensified patients achieved corticosteroid-free remission….Patients with minimal/no response to induction had lower odds of remission after intensification.”
S Dansese et al.Clin Gastroenterol Hepatol 2022; 20: 2858-2867. Open Access! Early Symptomatic Improvement After Ustekinumab Therapy in Patients With Ulcerative Colitis: 16-Week Data From the UNIFI Trial This study, a post hoc analysis of UNIFI trial, found that an early (2 week) symptomatic remission with ustekinumab in 20.2% (P = .012) vs placebo (12.9%). The more extensive results reviewed in the article (Figure 2) showed increasing symptomatic remission rates at week 4 (32.9%), week 8 (44.7%), and week 16 (53,1%) with IV dose of 6 mg/kg. The biologic-naive group had higher symptomatic remission rates (69% at week 16).
Deepdene Park, Atlanta. Part of Olmstead Linear Park
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.