Congratulations to Bonney!


Congratulations to Bonney!
DA Schwartz et al. Clin Gastroenterol Hepatol 2022; 20: 1059-1067. Open Access: Efficacy and Safety of 2 Vedolizumab Intravenous Regimens for Perianal Fistulizing Crohn’s Disease: ENTERPRISE Study
Methods: “Patients with moderately to severely active CD and 1–3 active perianal fistulae (identified on magnetic resonance imaging [MRI]) received vedolizumab 300 mg intravenously at weeks 0, 2, 6, 14, and 22 (VDZ) or the same regimen plus an additional vedolizumab dose at week 10 (VDZ + wk10)… Enrollment was stopped prematurely because of recruitment challenges”
Key findings:
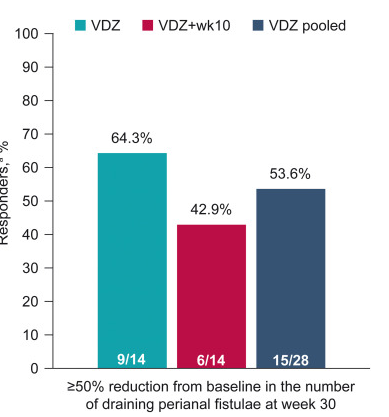
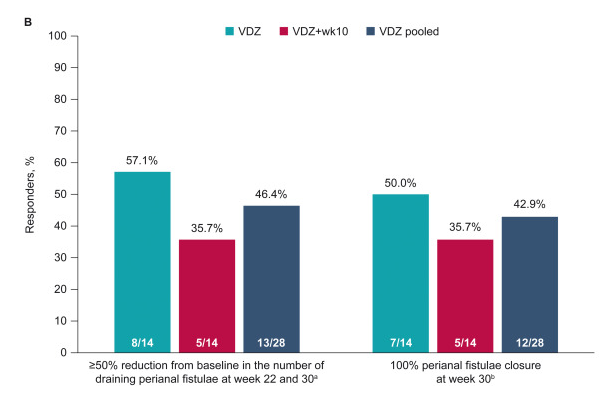
The study findings are limited by relatively small size and lack of control group (eg. placebo or seton/antibiotic group). However, the rate of response in this study is significantly higher than placebo studies which have shown “~1 in 6” who experienced fistula closure.
My take: Vedolizumab is another option for treating Crohn’s disease with perianal fistula. Both regimens in this study were associated with response, though the additional 10-week dose (in one group) did not improve outcomes.
Related blog posts:
Most patients that I see with celiac disease (CD) do very well after diagnosis/implementation of dietary therapy. A recent study indicates a subset of patients have significant work disability as adults.
SR Bozorg et al. Clin Gastroenterol Hepatol 2022; 20: 1068-1076. Open Access: Work Loss in Patients With Celiac Disease: A Population-based Longitudinal Study
In this large-scale nationwide study (part of the ESPRESSO study) from Sweden, the authors used prospectively recorded register data to estimate work loss in patients with CD in comparison to the general population, including the temporal relationship of work loss before and after diagnosis. This study included more than 16,000 patients with CD.
Key findings:
In the discussion, the authors speculate about whether the work loss could be due to inadequate response to a gluten free diet; however, in this study, the authors found similar work loss between patients with CD with or without mucosal healing (only 25% underwent f/u biopsy).
My take: It would be interesting to see the pediatric corollary of work loss, namely school absenteeism and whether this is increased in a small subset as well. My suspicion is that the subset with increased work loss likely has a higher rate of functional disorders, in addition to CD, than the comparator group and probably accounts for a significant amount of the work disability.
Related blog posts:

A couple recent articles indicate a lot of reasons for concern.
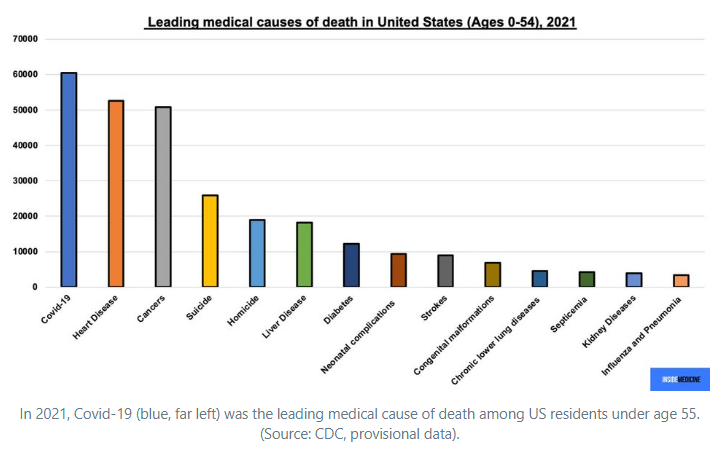
First of all, it is important to recognize that even among persons less than 55 years of age, COVID-19 was the leading cause of death in 2021. Inside Medicine: Open Access: The million US Covid dead are younger than you think.
Sadly, more than 300,000 deaths in the U.S. could have been averted (NPR: This is how many lives could have been saved with COVID vaccinations in each state)

There has been a culture shift to learn to live with the virus. This is evident almost everywhere from packed restaurants, crowded venues, etc. However, there is currently high transmission and variants that are evading vaccine protection as detailed by Eric Topol, Open Access: The Covid Capitulation
Key points:
My take: Unfortunately, these articles indicate that we have a long way to go. High quality masks are going to be needed at health care settings for a while. For those trying to avoid COVID-19, it will remain important to avoid large indoor gatherings. For public policy/economic policy, we need to continue to fund COVID-19 resources.

Related blog posts:
RC Ungaro et al. Inflamm Bowel Dis 2022; 28: 649-651. Impact of Thiopurine Exposure on Immunogenicity to Infliximab Is Negligible in the Setting of Elevated Infliximab Concentrations
Background: Whether proactive therapeutic drug monitoring (pTDM) is superior to reactive TDM (rTDM) is not entirely clear, though some studies have shown better outcomes with pTDM. Additionally, Colombel et al (Clin Gastroenterol Hepatol 2019; 17: 1525-32) showed that antidrug antibodies during combination therapy were detected only in those with the lowest quartile of infliximab trough levels; this suggests that optimized monotherapy should be similarly effective to combination therapy.
Methods: The authors retrospectively analyzed a commercial laboratory database (Prometheus) with 3970 patients and paired 6-thioguanine (6-TGN) levels with infliximab (IFX) and antibodies to infliximab (ATIs)
Key findings:
My take: In patients with IFX levels >5 mcg/mL, there does not appear to be much benefit for most patients from the addition of a thiopurine; this may not be true for those who are switching to a 2nd anti-TNF agent due to antidrug antibodies. This study supports pTDM to assure adequate IFX levels.
Related blog posts:
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition

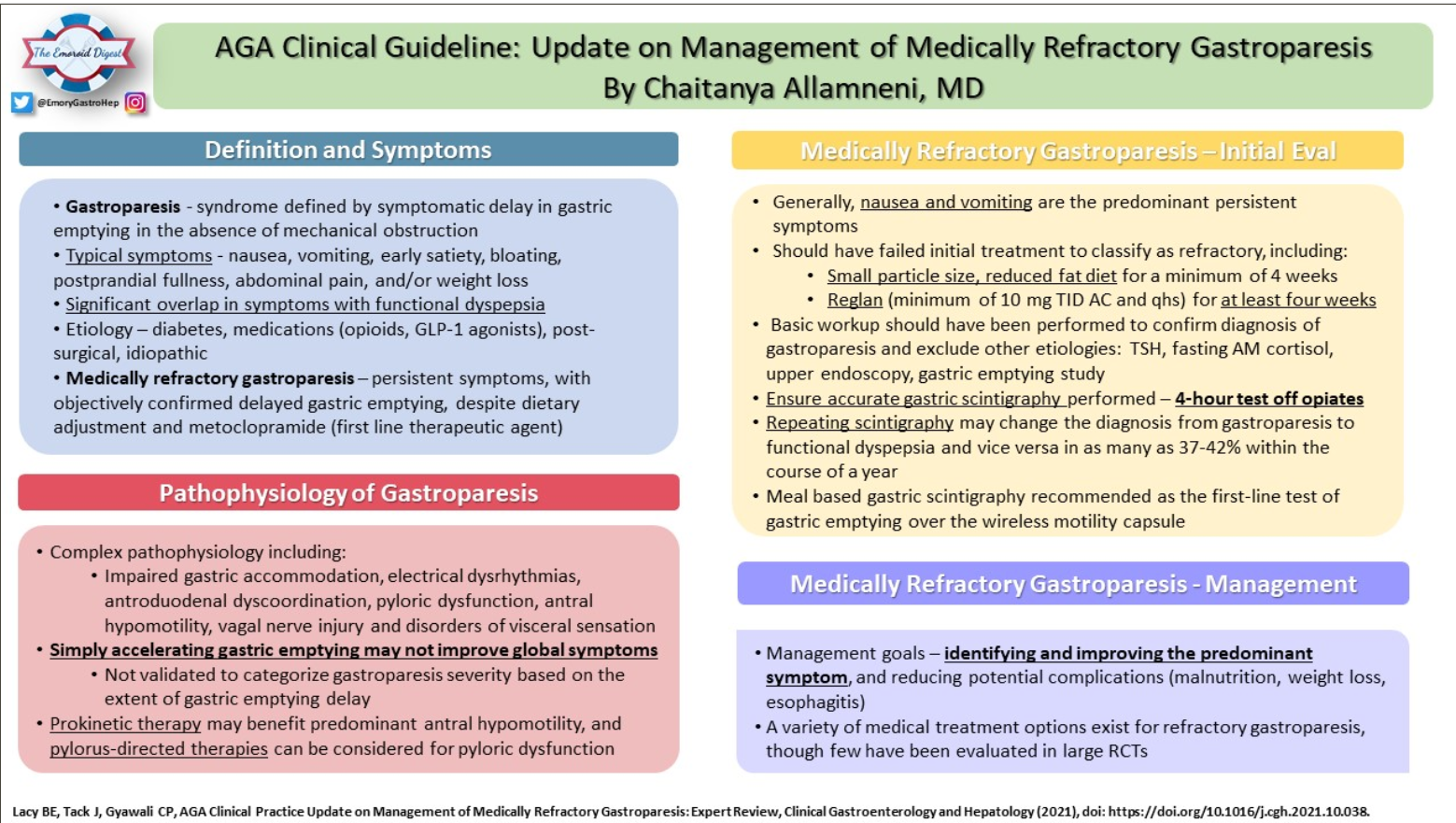
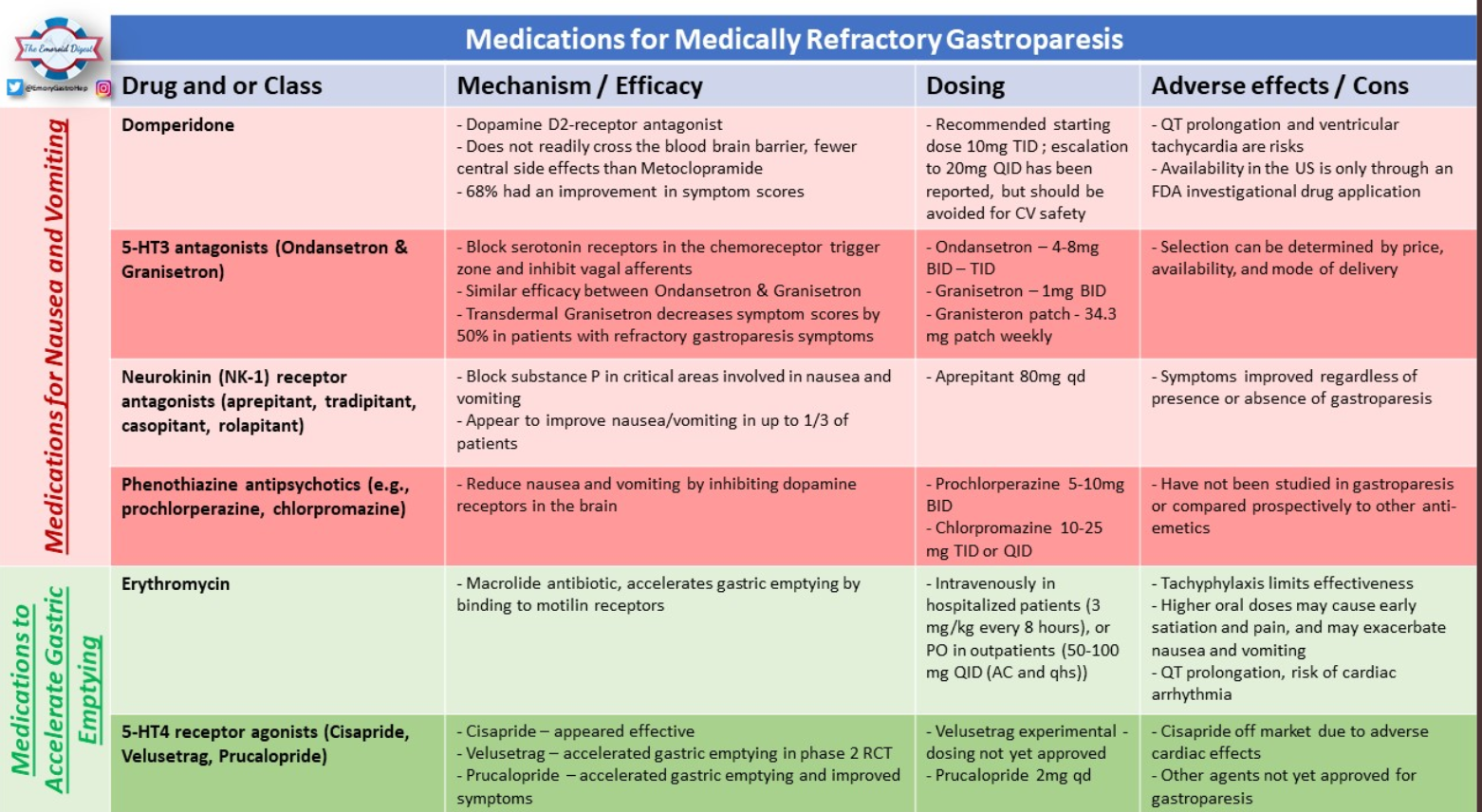
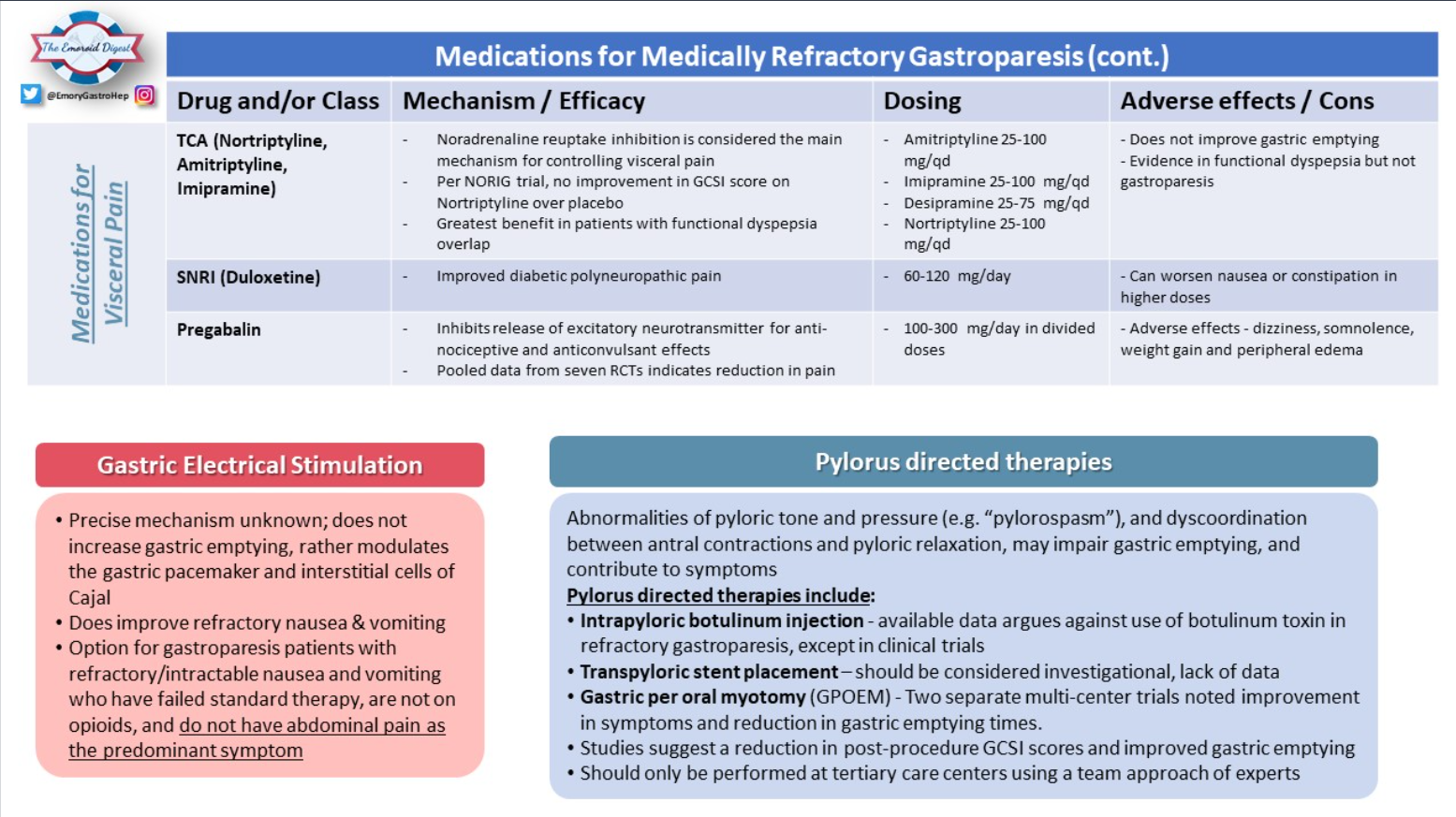
Tweetorial from “The Emoroid Digest”(posted 5/2/22):
Related blog posts:
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
CDC (January 2022): Open Access PDF: Our Risk of Infectious Diseases Is Increasing Because of Climate Change
“Between 2004 and 2018, the number of reported illnesses from mosquito, tick, and flea bites more than doubled, with more than 760,000 cases reported in the United States. Nine new germs spread by mosquitoes and ticks were discovered or introduced into the United States during this period. The geographic ranges where ticks spread Lyme disease, anaplasmosis, ehrlichiosis, and spotted fever rickettsiosis have expanded, and experts predict that tickborne diseases will continue to increase.”
EPA: Climate Change Indicators: Lyme Disease This EPA website has links to many other climate change indicators.

Related blog posts:
R Yadiatpati et al. Clin Gastroenterol Hepatol 2022; 20: 984-994. AGA Clinical Practice Update on the Personalized Approach to the Evaluation and Management of GERD: Expert Review
The general approach, outlined in Figure 1, is to empirically treat patients with typical GERD symptoms for 4-8 weeks with single-dose PPI. In those with response, the goal is to use the lowest effective dose and consider reflux testing (“offer endoscopy with prolonged wireless reflux monitoring”) if needing prolonged treatment (>1 yr). In those without a response, adjusting treatment (possibly change medication or change to twice a day) should be considered and reflux testing (off treatment) is recommended as well in those lacking response to treatment.
Some of the recommendations/best practice advice:
Related blog posts:

A recent article (The Dispatch, Scott Lincicome: America’s Infant Formula Crisis and the ‘Resiliency’ Mirage) explains that the reasons we are facing formula shortages go beyond the Abbott recall.
Excerpts:
The infant formula crisis isn’t simply another case of a one-off event causing pandemic-related supply chain pressures to boil over. Instead, U.S. policy has exacerbated the nation’s infant formula problem by depressing potential supply….all part of our government’s longstanding subsidization and protection of the politically powerful U.S. dairy industry…
[Additionally, there] are strict FDA labeling and nutritional standards that any formula producer wishing to sell here must meet….These regulatory barriers are probably well-intentioned, but that doesn’t make them any less misguided—especially for places like Europe, Canada, or New Zealand that have large dairy industries and strict food regulations
The combination of trade and regulatory barriers to imported infant formula all but ensures that our almost $2 billion U.S. market is effectively captured by a few domestic producers—despite strong demand for foreign brands. What German company, for example, is willing to spend the time and money meeting all the FDA requirements—registration, clinical trials, labeling and nutritional standards, inspections, etc.—only to then face high import taxes that make its product uncompetitive except during emergencies? The answer: almost none…
Meanwhile, Abbott is in full-on crisis mode and has turned to flying in formula produced at an FDA-registered Irish affiliate…
WIC program’s use of sole supplier contracts has created a problem specific to the current crisis because … the big FDA recall just happened to hit the very producer—Abbott—holding most of the WIC contracts.
My take: This article explains why there is not a simple switch to flip to fix the current formula bottlenecks.
Related blog posts:

Yesterday, this blog discussed what is needed to achieve high cure rates for H pylori. One of my microbiology colleagues informed me that until recently there have only been susceptibility standards for clarithromycin from the Clinical Laboratory Standards. Now, the European Committee on Antimicrobial Susceptibility Testing has criteria for clarithromycin, tetracycline, amoxicillin, levofloxacin, metronidazole, and rifampin. Given the difficulty culturing H pylori, his view is that stool testing is the most promising avenue for susceptibility testing because we now have the genes that determine resistance delineated for all of these drugs.
A related issue is antimicrobial stewardship: DY Graham. J-M Liou. Clin Gastroenterol Hepatol 2022; 20: 973-983. Open Access: Primer for Development of Guidelines for Helicobacter pylori Therapy Using Antimicrobial Stewardship
Key points:
H pylori is difficult to eradicate:
My take: The lack of action on H pylori susceptibility despite the current tools is a bad look for the GI community. Would this still be the case if the treatment were relegated to our infectious disease colleagues? Antibiotic stewardship is coming for H pylori -children and adults with this infection should have higher cure rates and easier treatment regimens.
Related blog posts: