- Thanks to Ben Gold & Rebecca Winderman (@kidsgastrodoc) (twitter feeds) for reference: Roca, M., Rodriguez Varela, A., Carvajal, E. et al. Open Access (full text): Fecal calprotectin in healthy children aged 4–16 years. Sci Rep 10, 20565 (2020). https://doi.org/10.1038/s41598-020-77625-7.
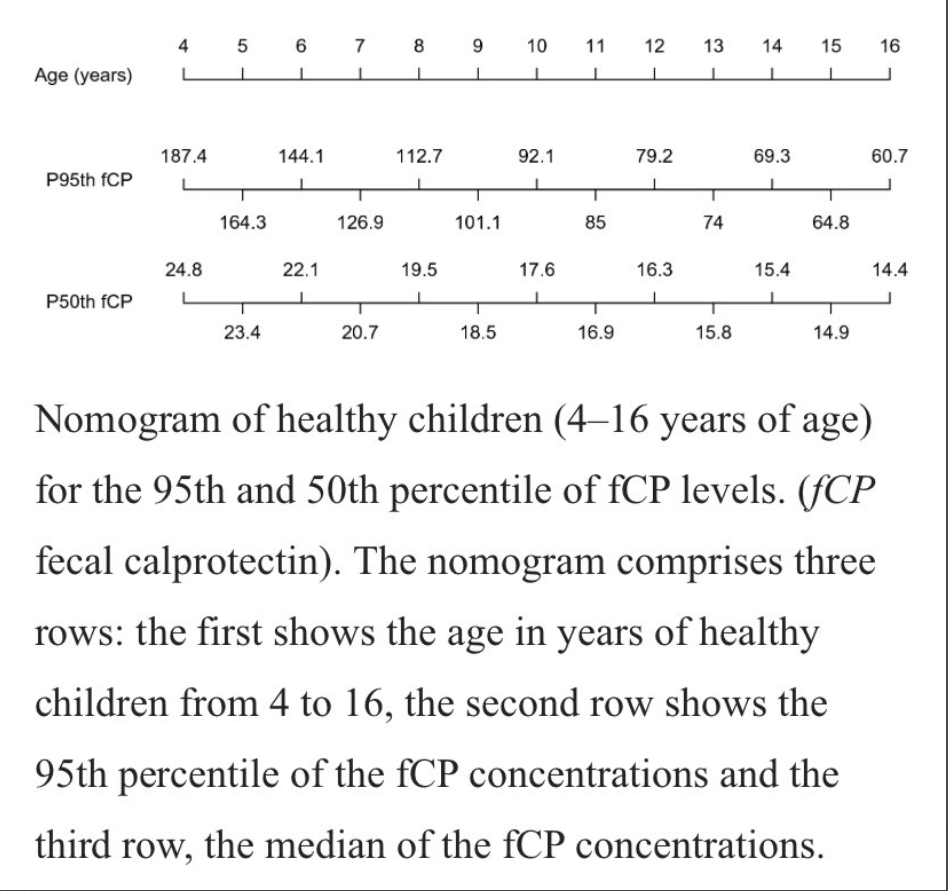
This study collected prospective data from 212 children. Key finding: The median and 95th percentile for fCP were 18.8 mg/kg and 104.5 mg/kg, respectively. “We found a statistically significant association between the 95th percentile of fCP concentrations and age (p < 0.001).”
My take: This is another study showing that calprotectin cut off values need to be higher in younger children.
Related blog posts:
- Fecal Calprotectin Levels Are Higher in the First Years of Life
- Keep the Stool Cool for More Reliable Calprotectin Testing
- Diagnostic Strategy for Children with Abdominal Pain and Diarrhea
- An Insurance Company Doing the Right Thing (with Calprotectin)
- Narrowing the Workup for Chronic Abdominal Pain –Carlo DiLorenzo Was Right! | gutsandgrowth
- Value of Calprotectin | gutsandgrowth