PJ Trivedi et al. Gastroenterol 2020; 159: 915-928. Effects of Primary Sclerosing Cholangitis on Risks of Cancer and Death in People With Inflammatory Bowel Disease, Based on Sex, Race, and Age
Methods: The authors linked prospectively collected data from national health care registries maintained for all adults in England on hospital attendances, imaging and endoscopic evaluations, surgical procedures, cancer, and deaths.
Key findings:
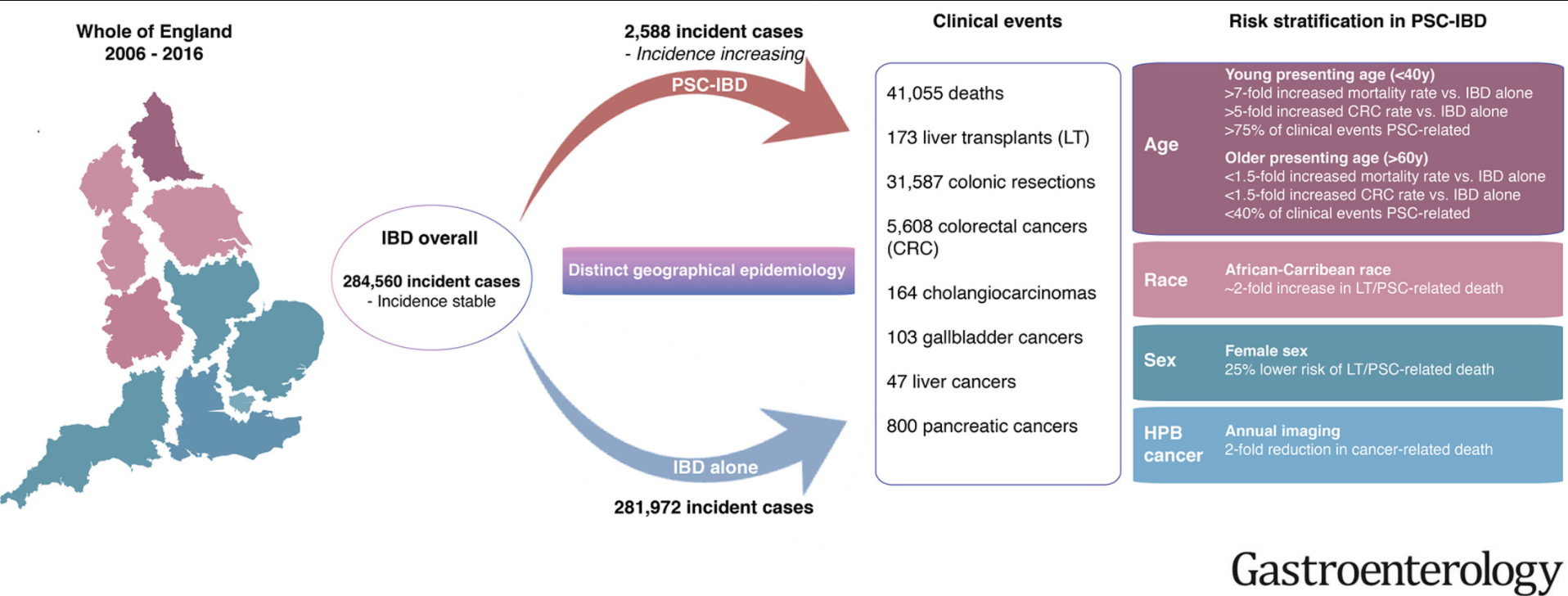
- Over 10 years, we identified 284,560 incident cases of IBD nationwide; of these, 2588 patients developed PSC. This study excluded patients <18 years of age.
- Development of PSC was associated with increased risk of death and CRC (hazard ratios [HRs], 3.20 and 2.43, respectively; P < .001) and a lower median age at CRC diagnosis (59 y vs 69 y without PSC; P < .001)
- Compared to patients with IBD alone, patients with PSC-IBD had a 4-fold higher risk of CRC if they received a diagnosis of IBD at an age younger than 40 years
- Development of PSC also increased risks of cholangiocarcinoma (HR, 28.46), hepatocellular carcinoma (HR, 21.00), pancreatic cancer (HR, 5.26), and gallbladder cancer (HR, 9.19) ( P < .001 for all)
- The greatest difference in mortality between the PSC-IBD alone group vs the IBD alone group was for patients younger than 40 years
- Patients with PSC-UC had >40% risk of colonic resection compared to patients with IBD alone (aHR 1.65)
My take: This study shows the impact the added diagnosis of PSC has for patients with IBD. One of the limitations in assessing outcomes is determining whether someone with IBD has PSC as there are a lot of patients with IBD who have asymptomatic changes in their biliary tree.
Related blog posts:
- Online Aspen Webinar (Part 3) -PSC in Pediatrics
- Easy Advice for Pediatric Hepatologists: PSC Guidelines from AGA Best practice advice 6: “Surveillance for cholangiocarcinoma should not be performed in PSC patients with small-duct PSCs or those younger than age 20.”
- Ursodeoxycholic Acid for Pediatric PSC
- Active Colitis More Likely in Children with PSC-IBD
- Big Study of PSC in Children
- PSC -Natural History Study (pediatric)
- Primary Sclerosing Cholangitis (PSC) –Natural History Study
- Why does PSC increase the risk of colorectal cancer in UC?
- Should We Care About Subclinical Primary Sclerosing Cholangitis with Inflammatory Bowel Disease?
- Staying current with PSC
- Primary Sclerosing Cholangitis 2016 | gutsandgrowth
- Population-Based Outcomes for Primary Sclerosing Cholangitis
- PSC 2013 Review