More from our recent AAP Board Meeting –more highlights:
Dr Sally Goza, AAP National President reviewed some of the AAP’s initiatives:
- Healthcare coverage & Change in ‘public charge’
- Gun violence
- Climate Change
- Early Childhood Programs
- Suicide Prevention
- E-cigarettes
- Social Media. She noted that Pinterest and Google have made efforts to curb harmful inaccurate posts, especially with regard to immunization information, whereas Facebook has not been cooperative.
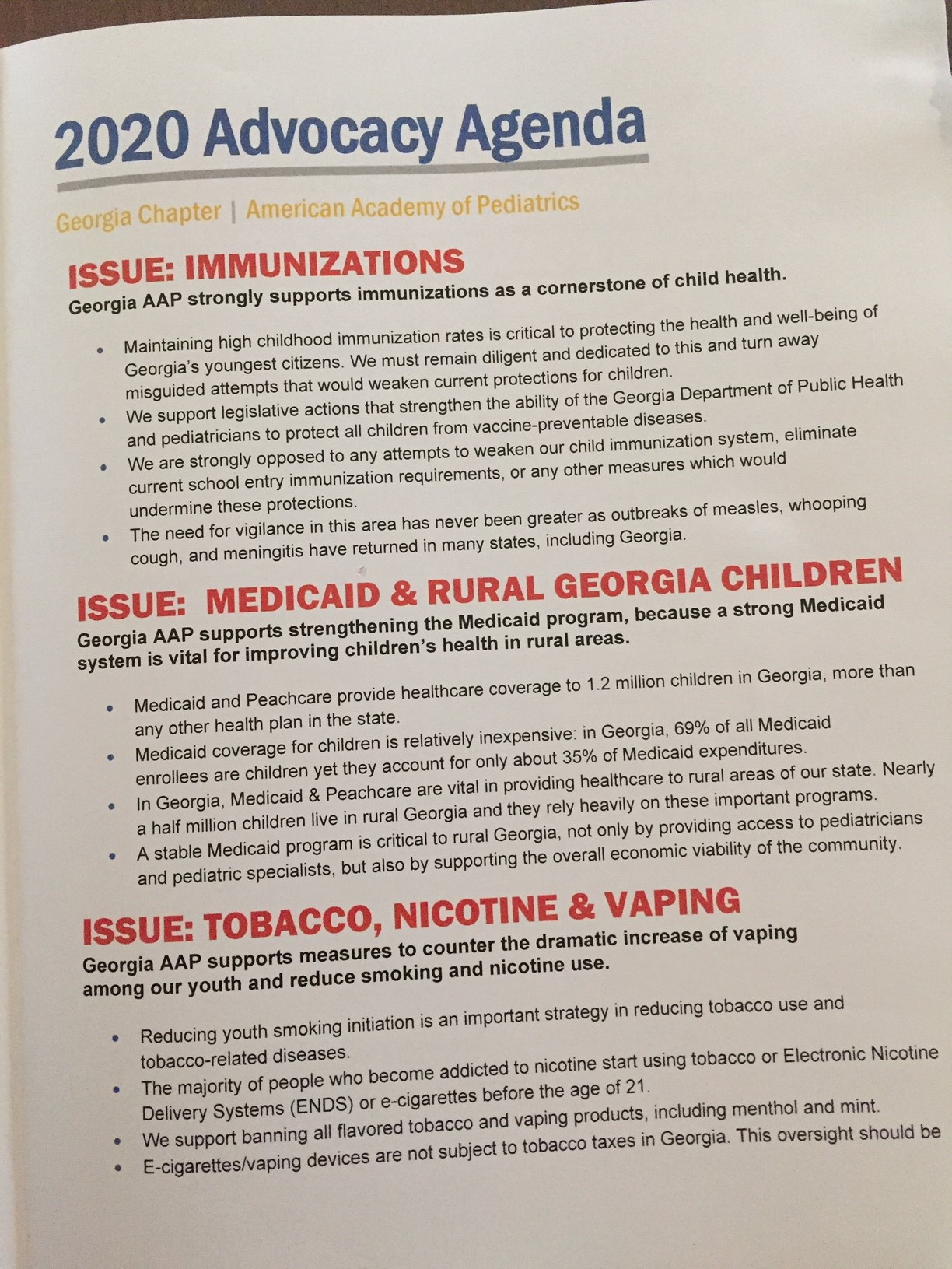
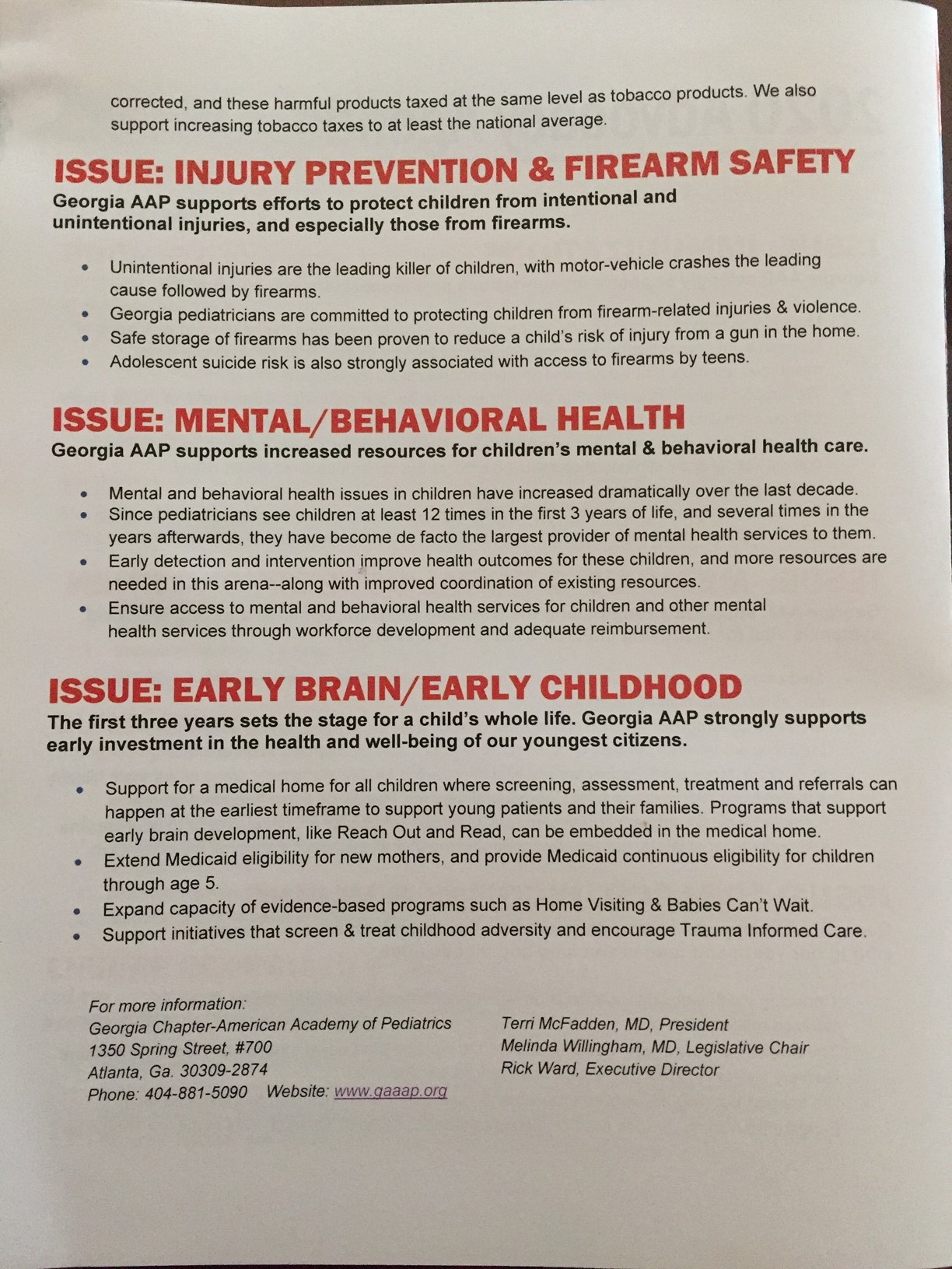
2020 Georgia Blueprint for Children:

Dr. Sarah Lazarus, a terrific ED physician and an advocate for safe sleep, described updates and obstacles related to reducing sudden unexpected death infant death.
Key points:
- NASPGHAN 2018 GERD recommendations (33 page PDF) with regard to positioning: “The working group recommends not to use positional therapy (ie, head elevation, lateral and prone positioning) to treat symptoms of GERD in sleeping infants”
- CPSC has removed many inclined sleepers. Commentary from Dr. Lazarus from WebMD (November 2019): Sleeping on an Incline Not Safe for Baby
The Consumer Product Safety Commission is warning parents not let a baby sleep in rockers, pillows, car seats, or any other product that holds an infant at an incline — with their head higher than their feet.
“I do think it should have happened a while ago when we saw there were deaths from them, but I’m glad they did it now,” says Sarah Lazarus, DO, a pediatric emergency medicine physician at Children’s Healthcare of Atlanta. Dr. Lazarus is also an injury prevention researcher at Emory University and reviews infant deaths for the state of Georgia. And what about putting the crib mattress at an incline to help with reflux?
- The High Toll of Sudden Infant Death From 2013-2015, there was an average of 3523 US infants each year who died from SUID (sudden unexpected infant death), peaking at 1-2 months of life. More black infants died of SUID in the first year than black children who died from firearm homicides in all of childhood through age 19 years. SUID deaths from 2013-2015 (10,568) was similar to the total number of motor vehicle-traffic deaths in all of childhood (10,714) and greater than the total number of any of the other causes.
- Are We Making Progress on Infant Sleep-Related Deaths? (not anymore)
- Safe Sleep (AAP 2017) Useful website: Charlieskids.org This website has a book called “Sleep Baby Safe and Snug” which incorporates updated recommendations on safe sleep practices.
- Preventing Sudden Infant Death -Latest Guidelines Children should sleep in the same room but on a separate surface from their parents for at least the first six months of their lives, and ideally the first year. They say that this can halve the risk of SIDS…You can read the AAP’s full guidance here.
Dr. Heval Kelli introduced a program called young physician initiative. “Getting into medical school can be a long process and difficult to navigate particularly for students from underserved communities due to the lack of access to medical mentorship and network. The Young Physicians Initiative provides early and interactive guidance to underserved middle school, high school and college students. We inspire students to pursue careers in medicine and pursue pipeline’s opportunities by Being Present in their communities.”
Here are links to his website and to one of the articles covering this project:
- Young Physicians Initiative
- How a Syrian refugee is recreating his ‘American Dream’ for the next generation
My take: This is a terrific program, though there are many other challenges that need to be addressed to encourage applicants from a wide range of socioeconomic groups.
Related blog post: Hidden Costs of Medical Schools


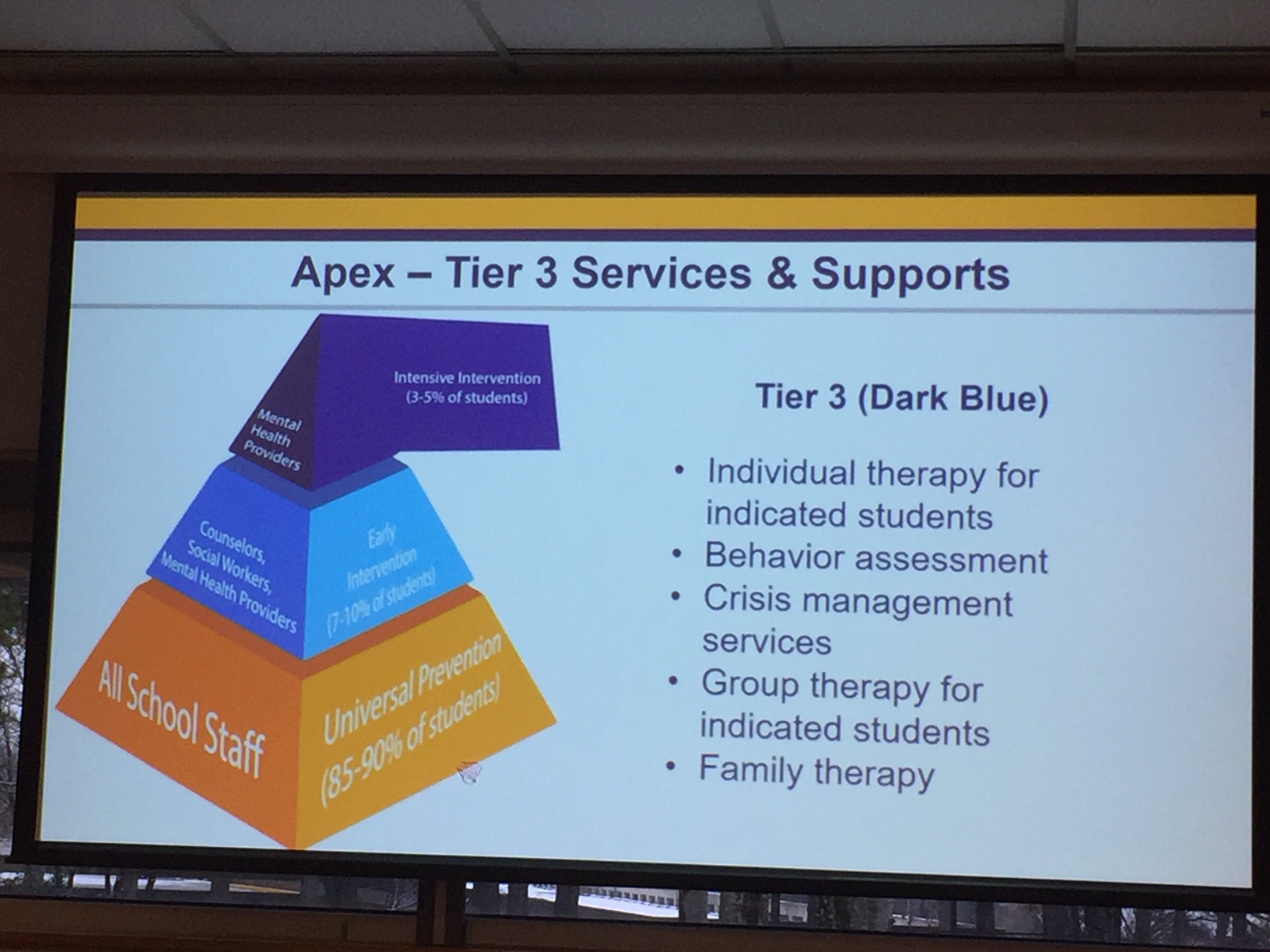
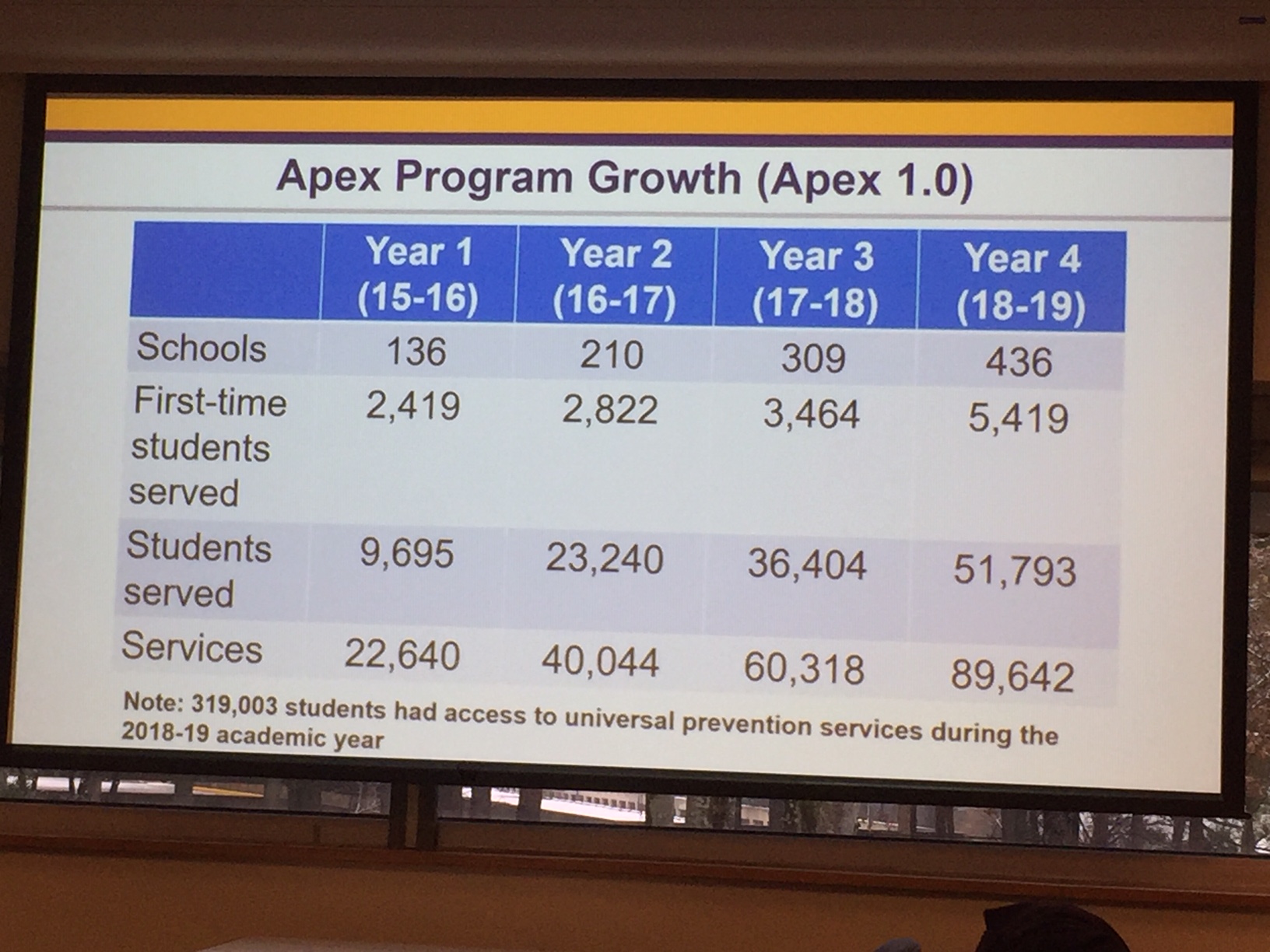
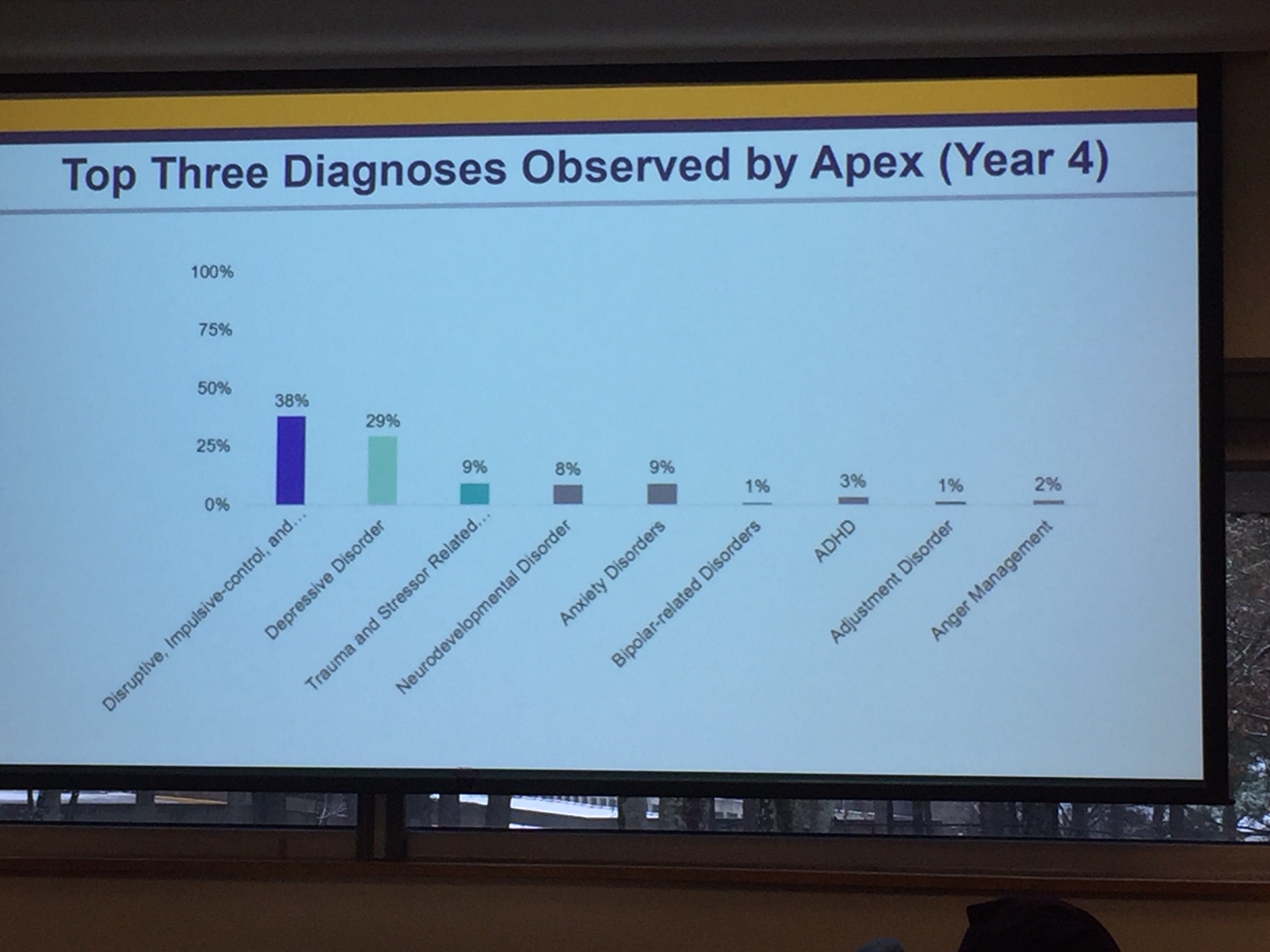
The final speaker, Dante McKay, discussed the APEX program which is a school-based program to address mental health issues in children.