Recently, I attended the 17th Annual Donald Schaffner lecture. This lecture honors the legacy of an outstanding surgeon who I had the opportunity to work with many years ago. One of my partners, Dr. Jeff Lewis, has been instrumental in arranging these annual lectures.
This terrific lecture by Emory physician, Dr. Stan Sonu, focused on Adverse Childhood Experiences (ACEs). While this has been a pervasive long-standing problem, there has been heightened interest in this topic following the shameful policy of promoting childhood separations at the U.S.-Mexico border.
This lecture explained how widespread the problem of ACEs is among children born in the U.S., even among the affluent. Much of the lecture focused on the ACEs study which included a cohort of 17,000 –all of whom were insured and 75% were white and 75% were college educated.
Here are pictures of some of the slides -which explain the scope the problem and the consequences of ACEs:
The above slide provides the three take home points.




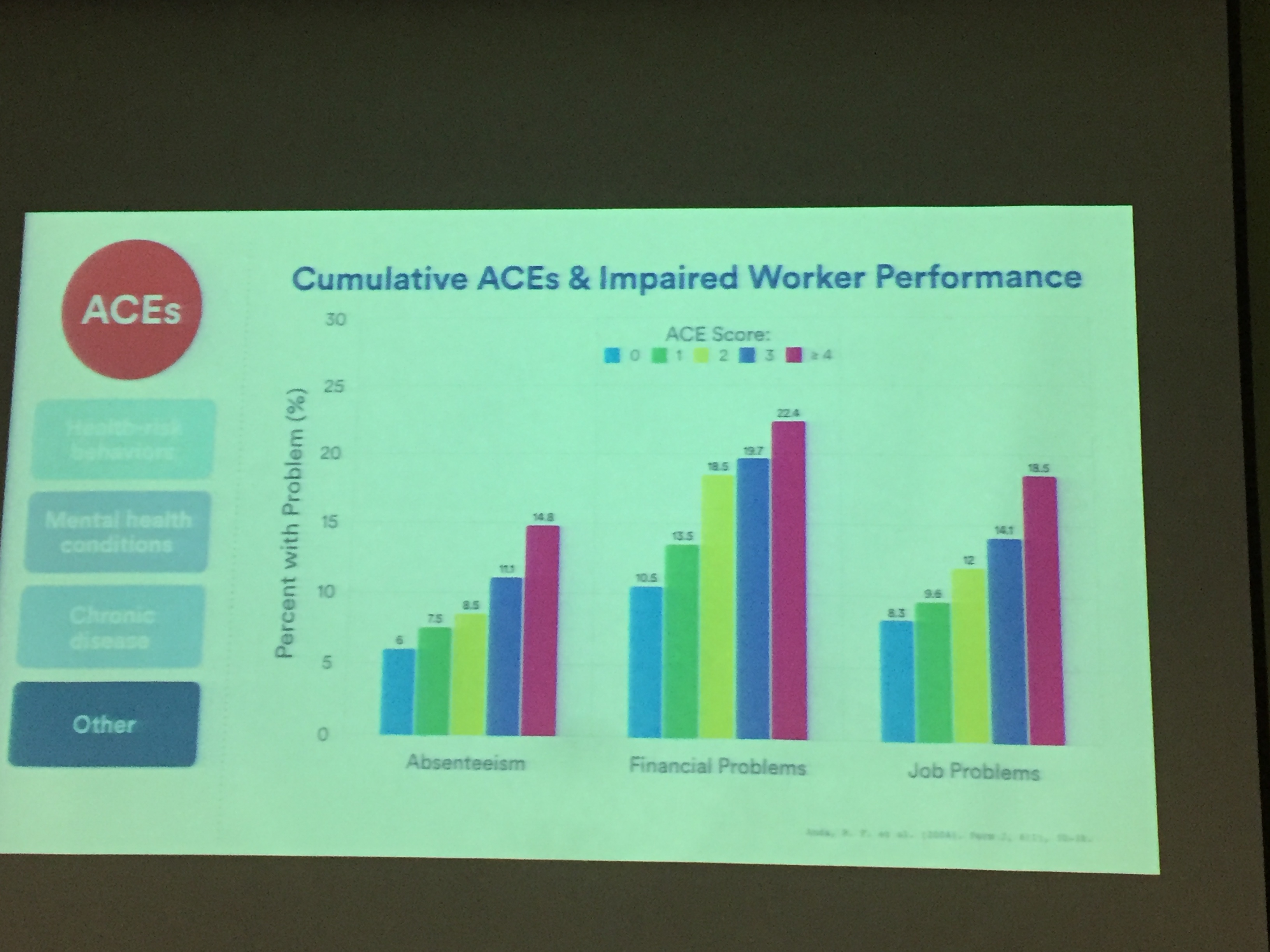
The slide above shows associations between ACEs and smoking drinking, and IV drug use. The slides below shows associations between ACEs and negative mental health outcomes, chronic diseases, and poor work performance.




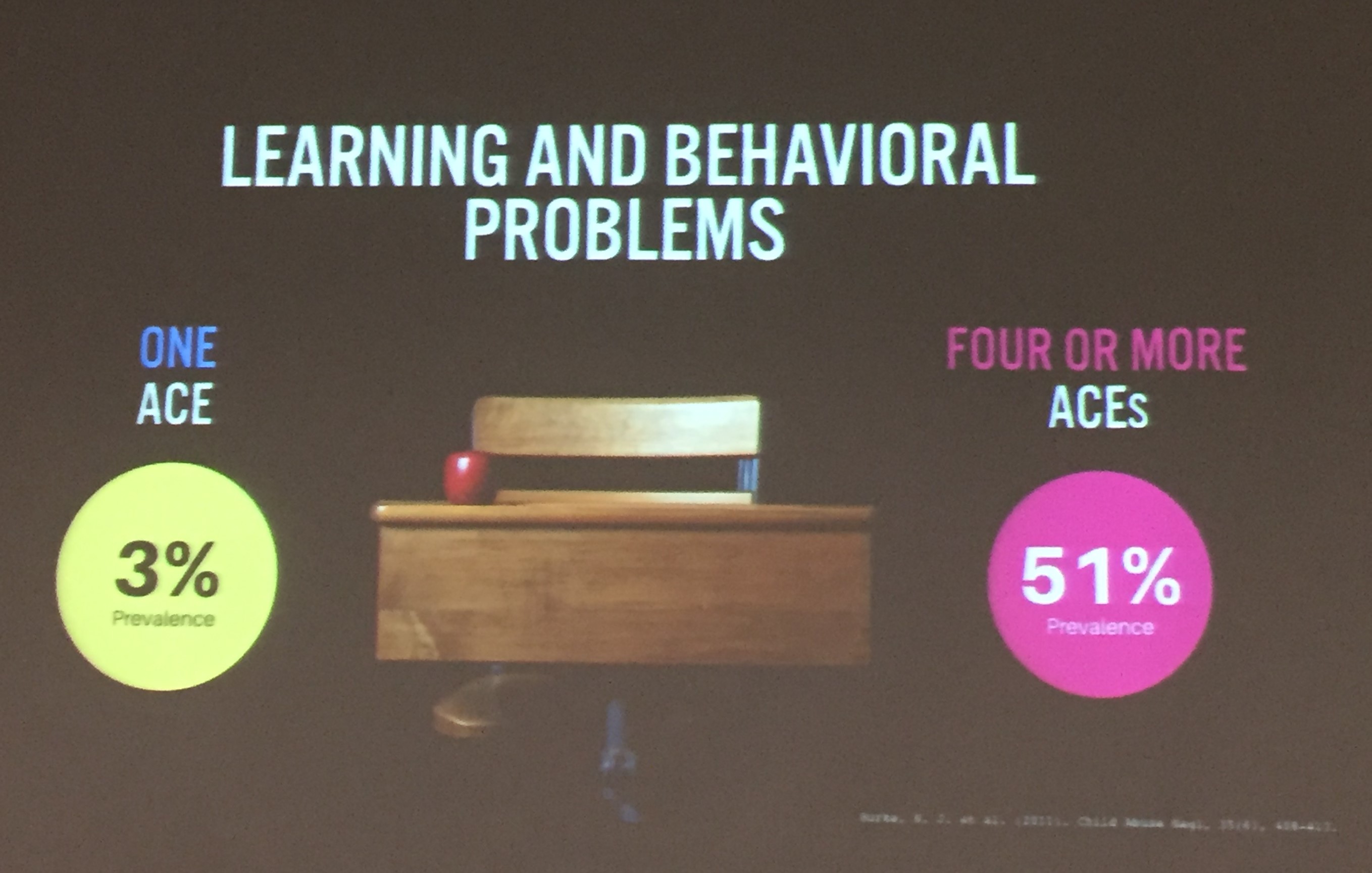
The slide above demonstrates that adverse health effects are increased even among 18-34 year olds. The slide below showed that learning problems are associated with ACEs as well; thus, the effects of ACEs start in childhood.




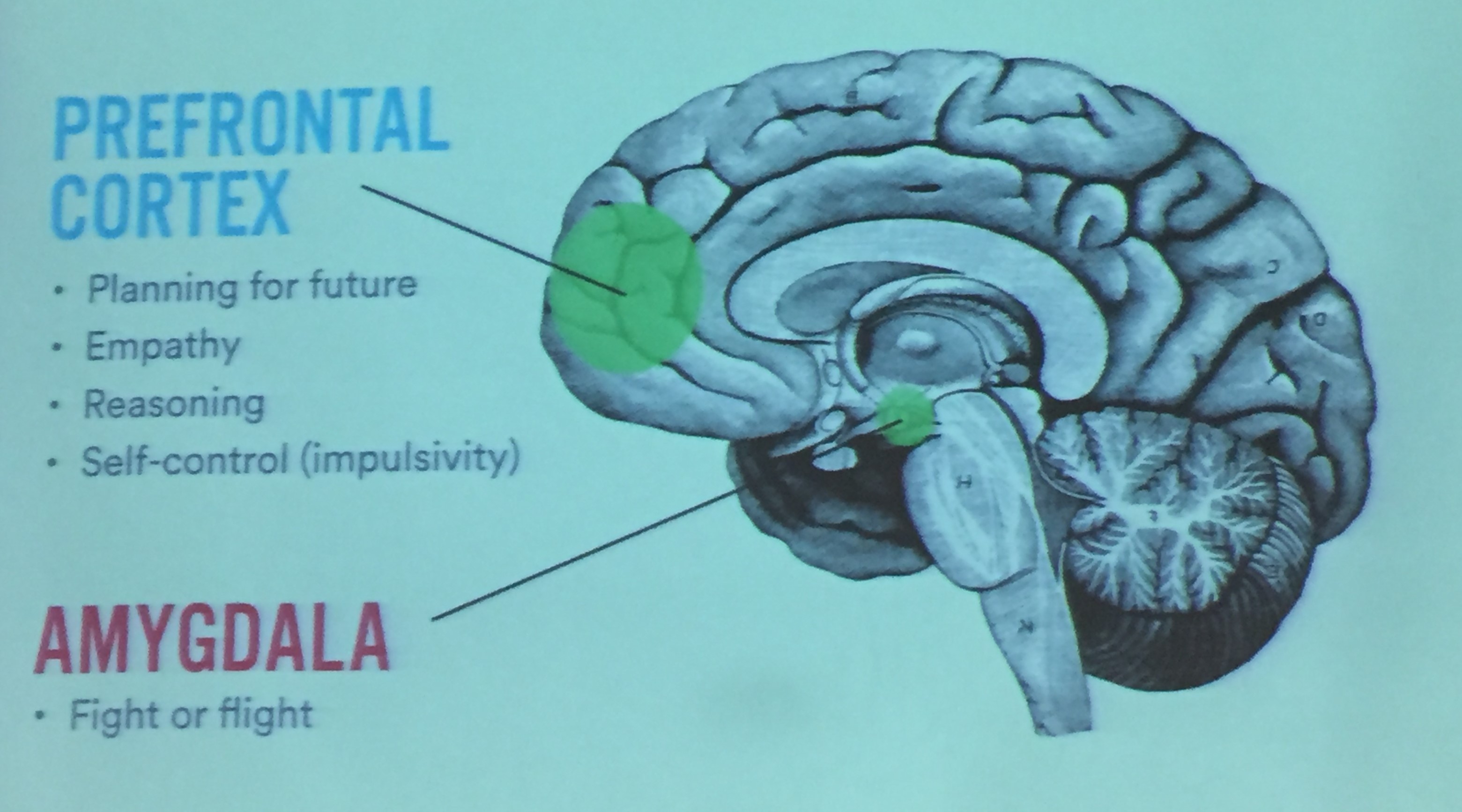
The slide above coincided with discussions (&other slides) of how toxic stress can result in physical changes to the brain.
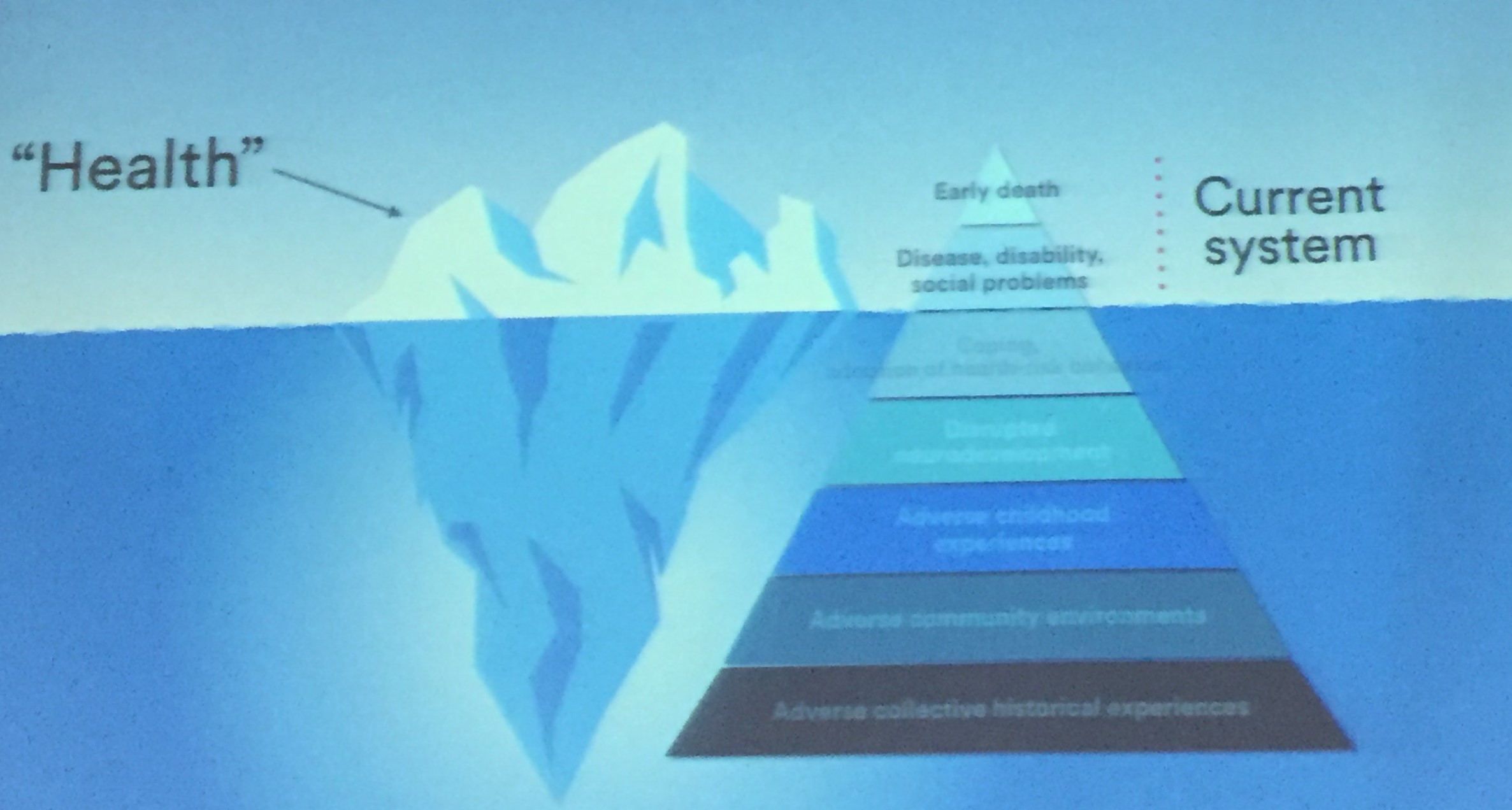
The slide above (which is difficult to see) indicates that while we see the health effects, we often are not seeing ACEs directly.

Dr. Sonu stated the single most protective factor was having a stable relationship with caregiver.