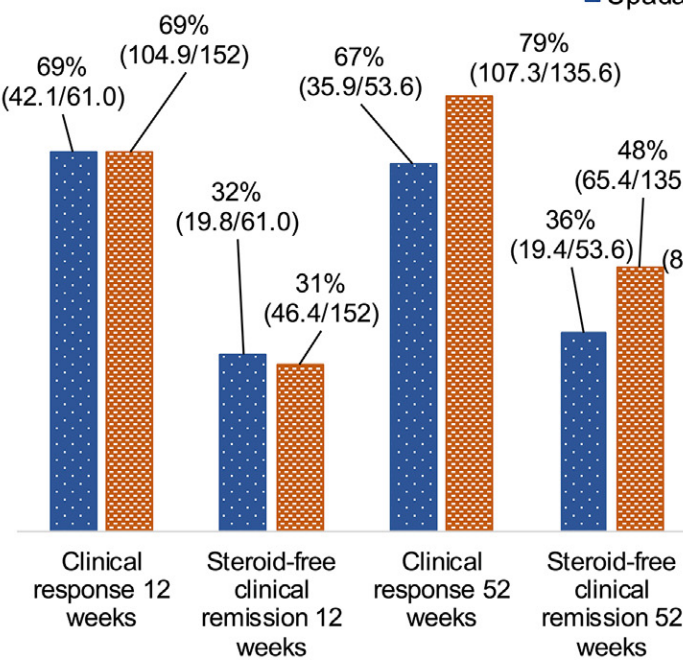
This was a retrospective single-center study (n=219) assessing upadacitinib (n=67) or risankizumab (n=152) for active Crohn’s disease (CD). Treatment initiation as post-operative prevention or for non-CD indication were excluded.
**The patients receiving upadacitinib were generally younger, had more anti-TNF/ustekinumab failures, higher CRPs, and higher HBSs compared to risankizumab-treated patients.
Key findings:
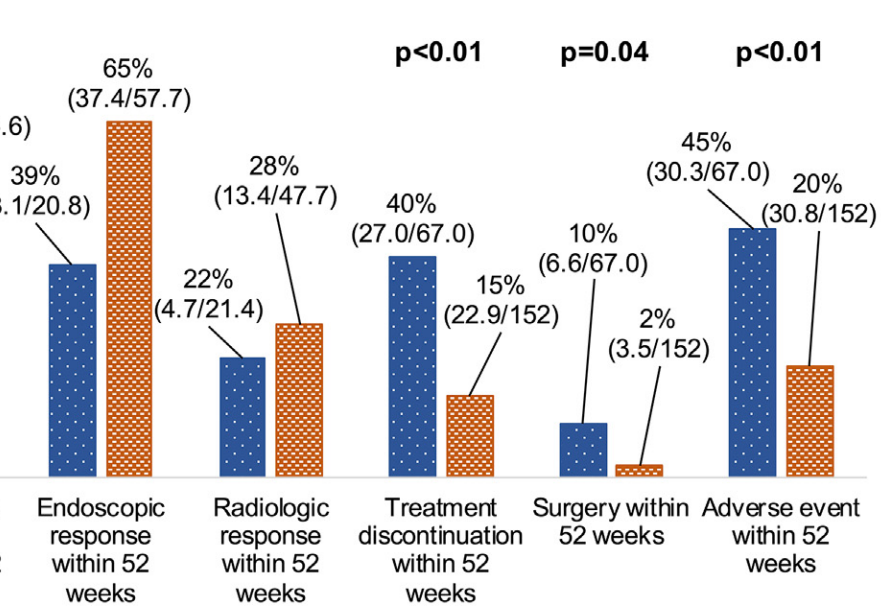
After inverse probability of treatment-weighted (IPTW) analysis, most outcomes were similar between groups. However, upadacitinib-treated patients had more surgeries, adverse events, and treatment discontinuation.
Fractions include nonintegers due to weighting, and denominators vary due to missing data.
My take: While this study favors risankizumab over upadacitinib, most of the outcomes were fairly similar. Risankizumab may have better long-term durability. However, the observational design limits the conclusions, particularly as the upadactinib-treated patients appeared to be more refractory at baseline. A prospective head-to-head study would be more definitive.
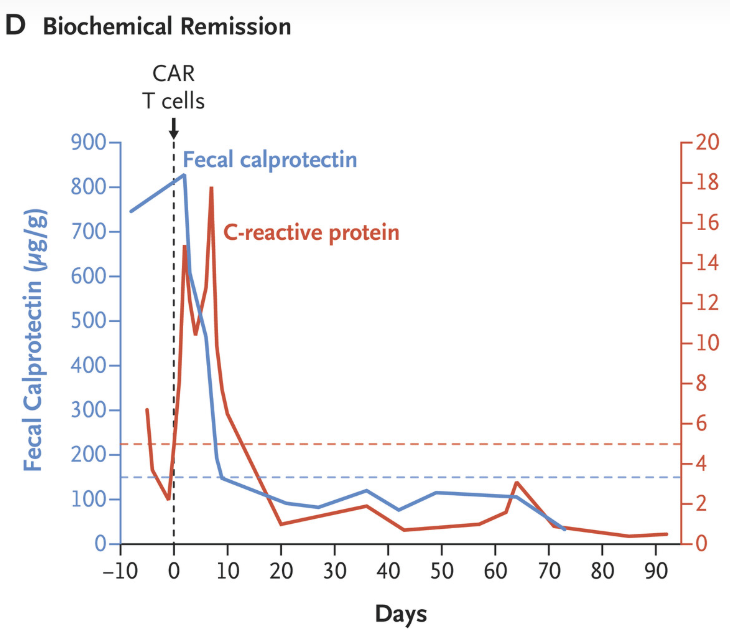
F Muller et al. NEJM 2025;393:1239-1241. CD19 CAR T-Cell Therapy in Multidrug-Resistant Ulcerative Colitis
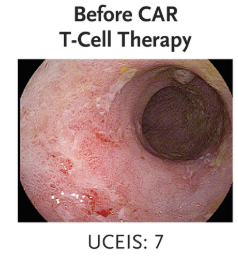
This case study involved the use of “autologous chimeric antigen receptor (CAR) T cells targeting CD19 in a 21-year-old woman with severe multidrug-resistant ulcerative colitis, who had declined colectomy. Previous treatments with prednisolone, mesalamine, infliximab, ustekinumab, ozanimod, filgotinib, vedolizumab, upadacitinib, and cyclosporine combined with mirikizumab had not induced clinical remission.”
“Clinical and biochemical remission occurred and were maintained over the 14-week follow-up period… without the use of concomitant therapy. Endoscopic, histologic, and ultrasonographic assessments showed signs of mucosal healing over time….These data suggest the possibility that CD19 CAR T-cell therapy can induce rapid drug-free remission in refractory ulcerative colitis, a disease that was previously thought to be largely B-cell–independent, given that rituximab treatment showed no efficacy..”
My take: This is only a single case report. However, it shows that modulation of the immune system could potentially cure ulcerative colitis. At the same time, long term adverse effects of CAR-T therapy will need to be monitored.
MA Colak et al. J Pediatr Gastroenterol Nutr. 2026;82:358–365. Improvement in bile drainage after Kasai portoenterostomy with a tailored steroid protocol
In this retrospective study, 28 infants underwent Kasai portoenterostomy (KPE) between 2015 and 2025. Group A had 16 infants managed without steroids between 2015 and 2021, while Group B included 12 infants managed under the new tailored steroid protocol between 2021 and 2025.
Determination of bile drainage: Postoperative stool color is monitored closely and collaboratively by hepatologists and surgeons according to the Japanese Tochigi Prefecture 3rd Edition stool card to assess bile drainage over the first five postoperative days.23 Patients with ≥50% of stools at color ≤3 are considered to have poor bile drainage, while those with >50% of stools at color ≥4 are considered to have good bile drainage.
Tailored steroid protocol: “If patients have poor bile drainage, further management depends on age at time of operation. Patients ≤45 days old at operation are started on a combined steroid and antibiotic treatment immediately after bile leak is ruled out using abdominal ultrasound. Patients >45 days old at operation are started on the steroid and antibiotic treatment only if the liver biopsy obtained during operation demonstrated acute inflammation on histology.”
Key findings:
The 3-month post-KPE TB levels were significantly lower in Group B compared to Group A (0.9 [0.3, 1.9] mg/dL vs. 6.5 [0.6, 10.4] mg/dL, p = 0.036)
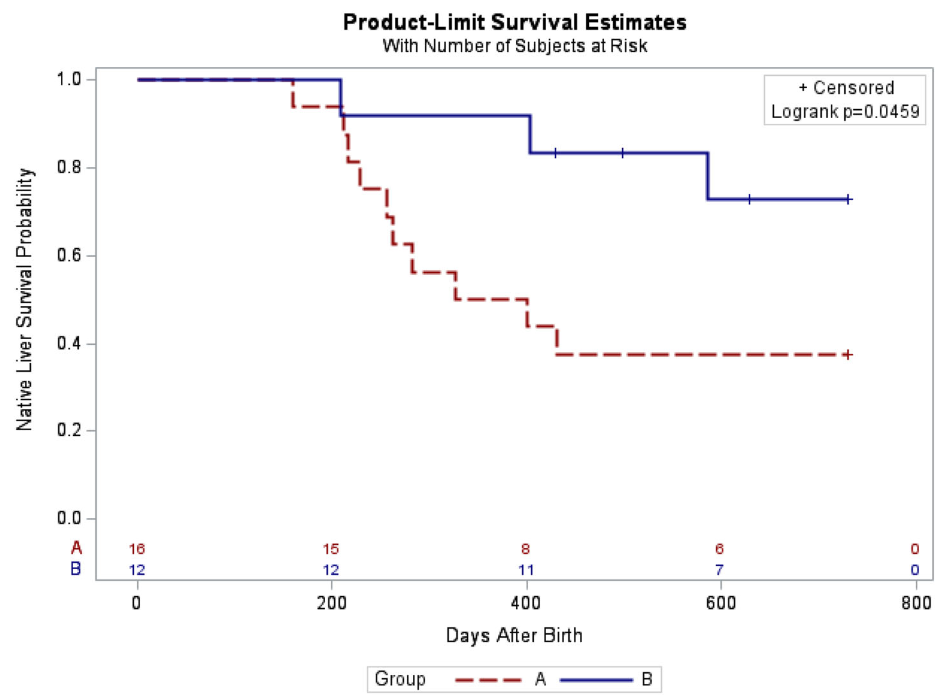
The 2-year native liver survival (NLS) was also significantly higher in Group B (72.9% vs. 37.5%, p = 0.046)
LOS, readmissions, reoperations, and complications in the 90-day postoperative period were not different between both groups
Kaplan–Meier curve of native liver survival at 2 years of age following Kasai portoenterostomy
In their discussion, the authors note that the “multicenter, placebo-controlled, double-blinded steroids in biliary atresia randomized trial (START) included 140 patients from the United States and assessed the effect of high-dose steroids (4 mg/kg/day).16 There was no significant difference in jaundice clearance at 6 months after operation (58.6% vs. 48.6%), nor significant difference in NLS at 2 years of age (58.7% vs. 59.4%) between the steroid and placebo groups.”
Subsequently, “similar to our study, Pandurangi et al. also reported a significant increase in the ratio of patients who had a TB level of <2 mg/dL at 3 months after operation in the customized steroid protocol cohort. However, although the steroid protocol cohort had greater 2-year NLS (68.8% vs. 50%), the difference did not reach statistical significance in their study.”
My take: The START study (n=140), which was powered to detect a 25% absolute treatment difference in TB levels, cannot exclude modest benefits from steroids. This current study, despite its limitations, showed that a tailored protocol for use of steroids may improve outcomes.
START Study: Steroids Not Effective For Biliary Atresia (After Kasai) In this study, the steroid intervention did not affect transplant-free survival which was 58.7% in the steroid group and 59.4% in the placebo group at 24 months of age. In addition, steroids were associated with an earlier onset of first serious adverse events.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
D Simon et al. J Pediatr Gastroenterol Nutr. 2026;82:407–414. Dolichocolon is common in pediatric gastroenterology patients with constipation and associated complaints
L Dorfman, A Kaul. J Pediatr Gastroenterol Nutr. 2026;82:320–322 Commentary. Dolichocolon in pediatric patients with constipation—The chicken or the egg?
Methods: In this retrospective study, a total of 155 contrast enemas were administered and then assessed for features of colonic redundancy consistent with dolichocolon (DC), based on a priori imaging (adult) criteria.
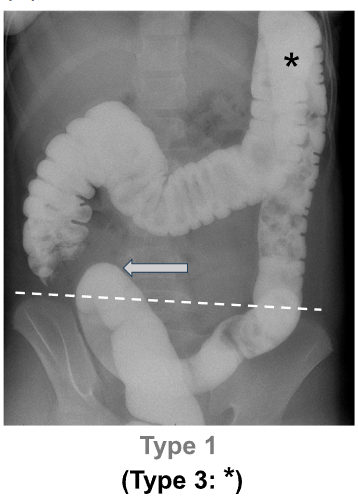
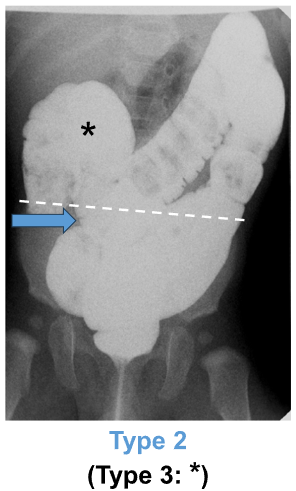
“DC was defined as: any portion of the sigmoid colon reaching above the iliac crest line (Type 1), and/or any portion of the transverse colon reaching below the iliac crestline with or without redundant flexures (Type 2)…We decided not to study Type 3 DC (i.e., redundant loops at the hepatic or splenic flexure, example shown in Figure 1A*) separately because that category was deemed to be arbitrary/imprecise.”
Key findings:
Consensus‐based identification (i.e., independent agreement among all three reviewers) of dolichocolon (DC) was observed in 74.1% of children under 2 years old and 88.6% of those aged 2–4 years presenting with constipation
The prevalence subsequently significantly decreased with age, with 68.8% in children aged 5–10 years and 47.6% in adolescents aged 11–17 years. “The pattern of decreasing prevalence of DC with age after 5 years is in contrast to findings in adult patients over 40 years with constipation, where DC frequency was found to increase significantly with age”
The vast majority (95.6%) of DC was Type 1; 3.5% was Type 2. 0.9% was both Type 1 and Type 2
The dashed line marks the iliac crest line [IC]; the gray arrow highlights the sigmoid colon reaching above the IC The blue arrow highlights the transverse colon falling below the IC
The editorial by Dorfman et al. notes that “dolichocolon has a long history in medical literature, but its exact role remains uncertain, presenting a classic “chicken or the egg” dilemma…Until more stringent pediatric-specific definitions and longitudinal evidence are acquired, clinicians should exercise caution in solely attributing symptoms to dolichocolon…While dolichocolon may play a role, it is unlikely to be the sole cause.”
My take: I had to read the article because I was not familiar with the term “dolichocolon.” The authors, though, summarize the key point: “the clinical relevance of this radiologic finding is not completely understood.” As a separate matter, a pediatric study on how a dolichocolon affects colonoscopy would be interesting; presumably, it would make it more difficult with longer duration and lower rates of TI intubation.
Danish residents with elevated lipids and CVD risk factors who were taking statins for CVD prevention saw a 16% lower risk per unit time of incident IBD, the researchers found (AS Faye et al. J Intern Med 2025;298[6]:686-696. Statin use for primary prevention of cardiovascular disease reduces the risk of incident IBD: A population-based cohort study)…
The study was a population-based, prospective cohort design drawing on the Danish National Registries. Participants were over 40 years of age and had undergone low-density lipoprotein (LDL) measurement between 2008 and 2022…Each of 110,961 people who picked up statin prescriptions within six months of LDL measurement was matched to five others (n=554,805) not prescribed statins by age, sex, calendar year, and CVD risk factors…
The aHR of developing IBD for statin users versus nonusers was 0.84 (95% CI 0.72-0.97)…The five-year number needed to treat (NNT) with statins was 2,881 to prevent one additional IBD case…
In addition to lipid-lowering properties, statins have anti-inflammatory and immunomodulating actions.
My take: This study suggests that statins have an “off target” beneficial effect in reducing the risk of inflammatory bowel disease. However, it is possible that statin use is not directly beneficial but an epiphenomenon. For example, individuals taking statins may have modified their diet to lower their risk as well.
Methods: “The LADI trial enrolled adults with luminal CD in corticosteroid-free clinical (CFCR) and biochemical remission, on adalimumab, 40 mg every 2 weeks. After randomization in a 2:1 ratio, the intervention group started on a 3-week interval and increased to 4 weeks, if in clinical and biochemical remission at week 24. The control group remained on adalimumab biweekly…The primary end point in this long-term follow-up (LTFU) study was the proportion of patients in CFCR (Harvey Bradshaw Index [HBI] <5 or remission per Physician Global Assessment [PGA] without systemic corticosteroids) without complications at year 3, on the assigned adalimumab interval.”
Key findings:
The proportion of patients achieving the primary end point was 34 of 95 (35.8%, intervention) vs 41 of 48 (85.4%, control; P < 0.001).
At year 3, 39 of 95 (41.1%) in the intervention group remained on the randomized or further de-escalated adalimumab regimen
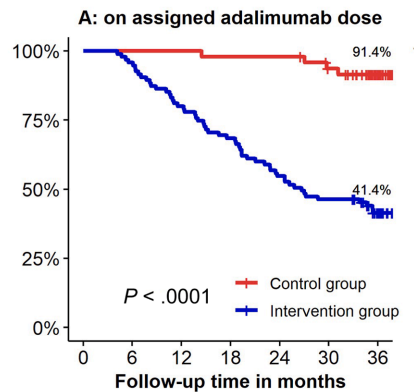
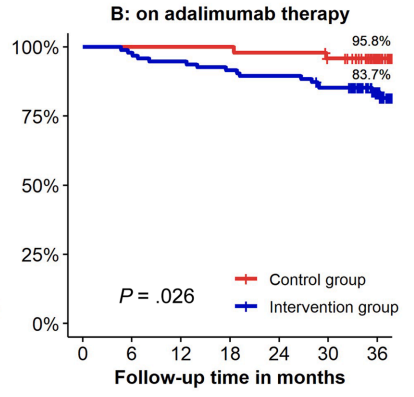
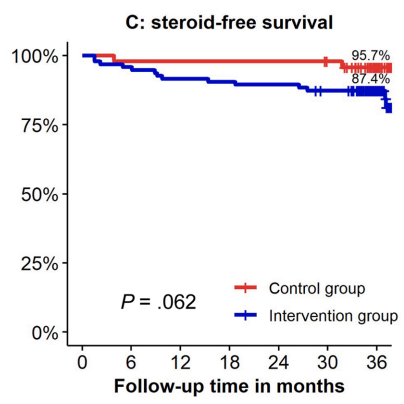
Kaplan-Meier analyses of secondary end points showed the following probabilities at year 3 (intervention vs control) (Figure 1): remaining on the assigned adalimumab dose, 41.4% vs 91.4% (P < .0001); remaining on adalimumab, 83.7% vs 95.8% (P = .026); corticosteroid-free survival, 87.4% vs 95.7% (P = .062); and complication-free survival, 83.2% vs 97.9% (P = .015)
Kaplan-Meier curves visualizing maintenance of assigned dosing at baseline, continued adalimumab therapy, and corticosteroid-free survival in both groups. (A) Probability of maintaining assigned adalimumab dosing interval of 3–4 weeks (intervention) vs 2 weeks (control).(B) Probability of remaining on adalimumab therapy over time. (C) Probability of remaining in corticosteroid-free remission.
My take: About 60% of patients were unable to de-escalate their adalimumab dosing interval. Suboptimal dosing increased the risk of complications and having adalimumab therapy become ineffective.
Methods: This was a prospective study with 300 endoscopies involving 112 patients with eosinophilic esophagitis (EoE).
Key findings:
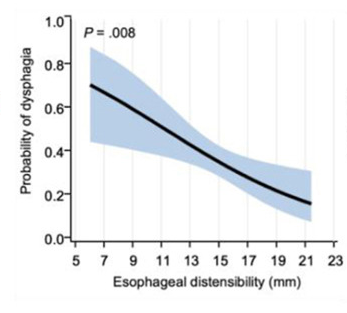
“Participants exhibiting a histologic response to treatment showed the most significant improvement in distensibility over time (1.41 vs 0.16–0.53 mm/y; P = .003).”
“After adjusting for Eosinophilic Esophagitis Endoscopic Reference Score and age at symptom onset, lower esophageal distensibility was independently associated with increased odds of patient-reported dysphagia” (odds ratio, 0.85; P = .008).
“Baseline distensibility predicted the need for future stricture dilation (area under the curve, 0.757; P = .0003).”
At baseline, fibrostenotic features were noted in 26 (23%) and strictures in 16 (14%).
Discussion Points:
“Our results support the potential plasticity of esophageal remodeling based on the observed improvement in distensibility among patients with adequately controlled inflammation.”
“A recent cohort study of 105 adult patients with EoE with more than 10 years of pediatric followup…found that patients with longer periods of histologic control were less likely to develop esophageal strictures.”
My take: The esophagus works better when eosinophilic inflammation is treated.
This is a terrific, succinct review of functional dyspepsia.
Key points:
“The syndrome probably comprises several different and as yet incompletely characterized disorders; local microinflammation driven by an aberrant response by type 2 helper T cells may represent an important subset of cases.”
“Functional dyspepsia can overlap with other gastrointestinal syndromes, particularly irritable bowel syndrome and gastroesophageal reflux disorder, and persons with such overlap have more severe symptoms.”
“There is no approved drug therapy; treatment is empirical and directed at symptoms, consisting of acid suppressants and low-dose tricyclic antidepressants (and other neuromodulators), along with appropriate nutritional and psychological support.”
Discussion points:
Epidemiology: “Worldwide, functional dyspepsia is present in 7.2% of adults (10.1% in the United States), affects women 1.6 times as often as men, and is more common in persons younger than 40 years of age.”
Diagnostic workup: Workup depends on clinical judgement. Careful evaluation is needed in the presence of alarm symptoms like GI bleeding, anemia, weight loss, dysphagia, personal/family history of gastrointestinal cancers.
Treatments:
“Acid-inhibition pharmacotherapy is considered to be first-line treatment in functional dyspepsia. However, the benefits of this approach are modest at best”
Neuromodulators: “Tricyclic antidepressants are considered first-line therapy in this category…Results of the Functional Dyspepsia Treatment Trial showed significant superiority of low-dose amitriptyline over placebo in achieving prespecified “adequate relief” for the last 5 weeks of the 10-week trial (53% with amitriptyline vs. 40% with placebo, P=0.05). The effect appeared to be greatest in participants with epigastric pain (relative risk, 1.34; 95% CI, 1.02 to 1.59). In contrast, the response obtained with escitalopram (a selective serotonin-reuptake inhibitor) did not differ from that obtained with placebo.39 The benefit of amitriptyline was independent of changes in depression or anxiety scores…Mirtazapine (an atypical tetracyclic antidepressant that also antagonizes histamine H1 receptors and serotonin 5-hydroxytryptamine [5-HT] type 3 receptors) also has shown efficacy in functional dyspepsia and may be best suited for patients with prominent nausea and clinically significant weight loss.41“
Psychology: “Recognition and treatment of uncontrolled anxiety and depression are important in all cases. In refractory functional dyspepsia, it is also important to consider psychological therapies as an adjunct for helping patients cope with their symptoms and perhaps attenuate the severity of symptoms. Studies support the use of cognitive behavioral therapy, mindfulness-based stress reduction, and hypnotherapy in functional dyspepsia, and benefits may last up to 12 months.42…the evidence from these trials is considered to be very low.”
Diet: “Dietary advice has not been shown to be effective in studies.”The effectiveness of simple dietary advice (i.e., small low-fat meals and avoidance of carbonated drinks to limit gastric distention), although seemingly rational, has not been borne out in a randomized trial.33 Low-FODMAP (fructans, fermentable oligosaccharides, disaccharides, monosaccharides, and polyols) diets have not been shown to reduce symptoms any more than traditional dietary advice.34…” IgE-mediated (classical) food allergy is generally not mistaken for functional dyspepsia, and screening for IgG-mediated reactivity to food antigens is not recommended.25“
Immune-Modulating Treatment: “A randomized, controlled trial of montelukast, a cysteinyl leukotriene antagonist, in children with duodenal eosinophilia and dyspeptic symptoms showed a significant effect in reducing pain as compared with placebo (62% vs. 32%, P<0.02), and the effect appeared to be even greater (84%) in patients with more than 20 eosinophils per high-powered field.43“
My take (borrowed from the authors) “Given the limited efficacy of drugs that are recommended under national and international guidelines…, the consideration of therapies for which evidence is insufficient may be reasonable in refractory cases.”
The authors make several good arguments for mass screening for celiac disease.
Key Points:
“The worldwide prevalence is high, affecting an estimated 1% to 3% of the general population…One study showed that two-thirds of children remain undiagnosed.” (Dig Liver Dis. 2023; 55:608-613). Thus, screening would identify many cases that would otherwise go undiagnosed and untreated
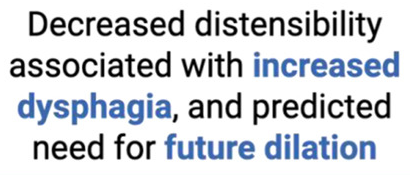
” As one of the most HLA-restricted diseases, nearly all patients carry HLA-DQ2.5, DQ2.2, or DQ8 (and very rarely DQ7.5), and their absence makes CeD extremely unlikely. Although 30% to 40% of the general population carry these alleles, only approximately 3% will go on to develop CeD”
“The Environmental Determinants of Diabetes in the Young (TEDDY) study showed that although there was some early anxiety reported, there was no long-term psychological harm in disclosing genetic risk to parents of children that were tested and most parents adapted over time”
“Children identified as highest risk at birth through HLA-DQ typing also represent an ideal cohort to test interventions such as dietary modifications or microbiome targeted therapies during the predisease phase, during the key “window of opportunity,” ideally before seroconversion (primary prevention).” There are no currently proven primary prevention interventions.
Some of the drawbacks to screening: 1. “Evidence on health benefits of treating asymptomatic CeD is limited.” 2. “The potential psychosocial effects of both newborn genetic testing and a strict gluten-free diet in individuals diagnosed through screening need to be considered.” 3. “HLA-DQ typing may be cost prohibitive in some regions of the world.” 4. “Most children identified to be at risk for CeD based on HLA-DQ will not develop CeD.”
My take: I am skeptical about the benefits of screening at birth and how it would work in our current health care system. We have plenty of examples in our field in which early screening is not followed up well (eg. Hepatitis C, Biliary Atresia). If more evidence emerges on the benefits of primary prevention, then more widespread screening at birth may be worthwhile. For example, there is “a clinical trial underway in Sweden, the GRAin study (NCT04593888) that aims to investigate whether eating a gluten reduced diet (<2 g of gluten per day) may reduce the risk of CeD in children with genetic risk.”
Methods: Multicentre, prospective cohort study conducted across 47 UK centres. Patients with Crohn’s disease (CD), ulcerative colitis (UC) or IBD unclassified (IBDU) in self-reported remission were prospectively followed up. 2629 participants (1370 CD; 1259 UC/IBDU) – followed up for a median of 4.1 years.
Key findings:
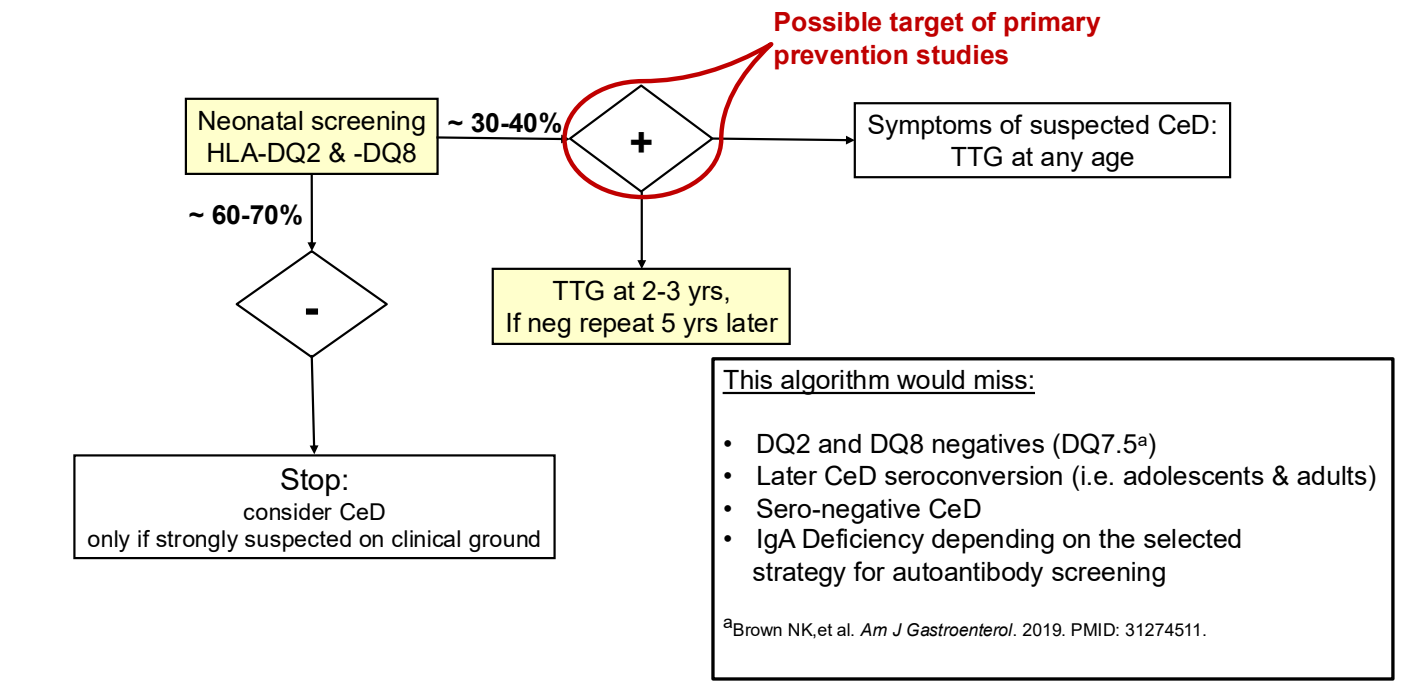
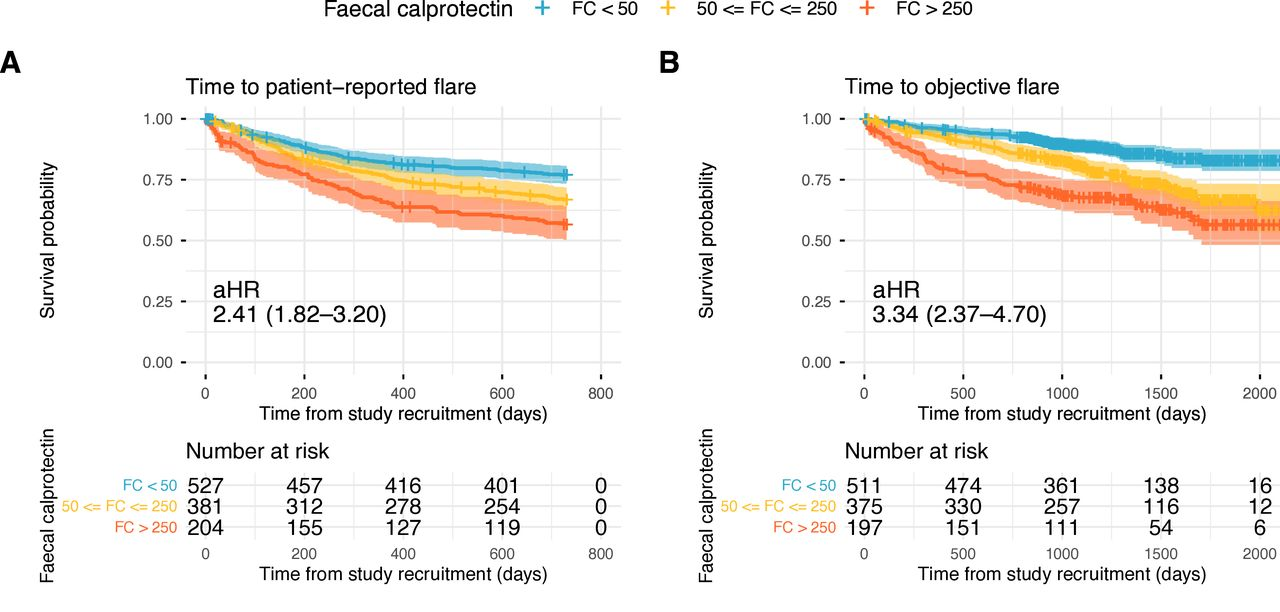
Baseline FC was strongly associated with patient-reported flares (FC ≥250 µg/g: adjusted HR (aHR) 2.22; FC 50–250 µg/g: aHR 1.52 (reference <50 µg/g)).
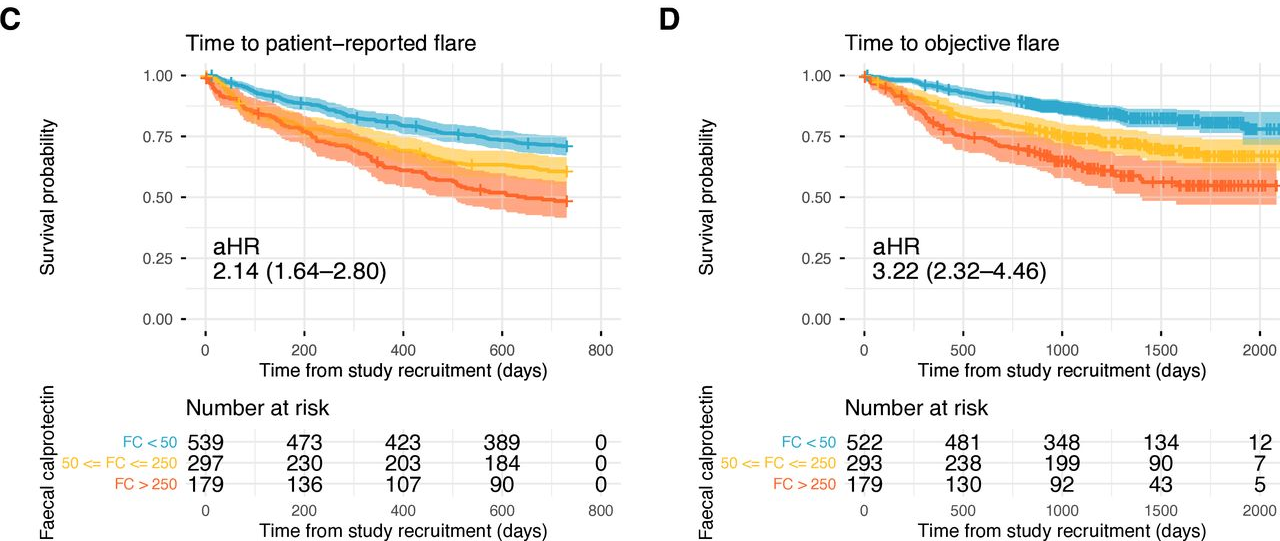
Baseline FC was also strongly associated with objective flares (FC ≥250 µg/g: aHR 3.25; FC 50–250 µg/g: aHR 1.98). Objective flares were “clinical flare plus C-reactive protein >5 mg/L and/or faecal calprotectin (FC) >250 µg/g with treatment escalation.” In ulcerative colitis, the probability of an objective flare within two years rose from 11% in those with baseline calprotectin below 50 µg/g to 34% in those above 250.
At 24 months, cumulative patient-reported and objective flare rates were 28% and 12% in CD, and 33% and 15% in UC/IBDU, respectively. Overall, patient-reported flares were more common (31%), while objective flares were less frequent (14%).
In UC, higher total meat intake was associated with increased risk of objective flares (highest versus lowest quartile: aHR 1.95, 95% CI 1.07 to 3.56). The absolute two-year risk rose from 12% in the lowest quartile of meat intake to 26% in the highest.
No consistent associations were observed for ultraprocessed foods, fiber or polyunsaturated fatty acids and flare.
Flares by faecal calprotectin (FC) stratified into FC < 50, 50 ≤ FC ≤ 250, and FC >250 μg/g. (A) Patient-reported flare in Crohn’s disease; (B) objective flare in Crohn’s disease; (C) patient-reported flare in ulcerative colitis/inflammatory bowel disease unclassified; (D) objective flare in ulcerative colitis/inflammatory bowel disease unclassified. aHR, adjusted hazard ratio.
My take: Lower calprotectin values, even in remission, are associated with better outcomes. Risk was meaningfully increased even in the 50–250 µg/g range, compared with levels below 50. Higher meat intake may increase the risk of flares for UC.