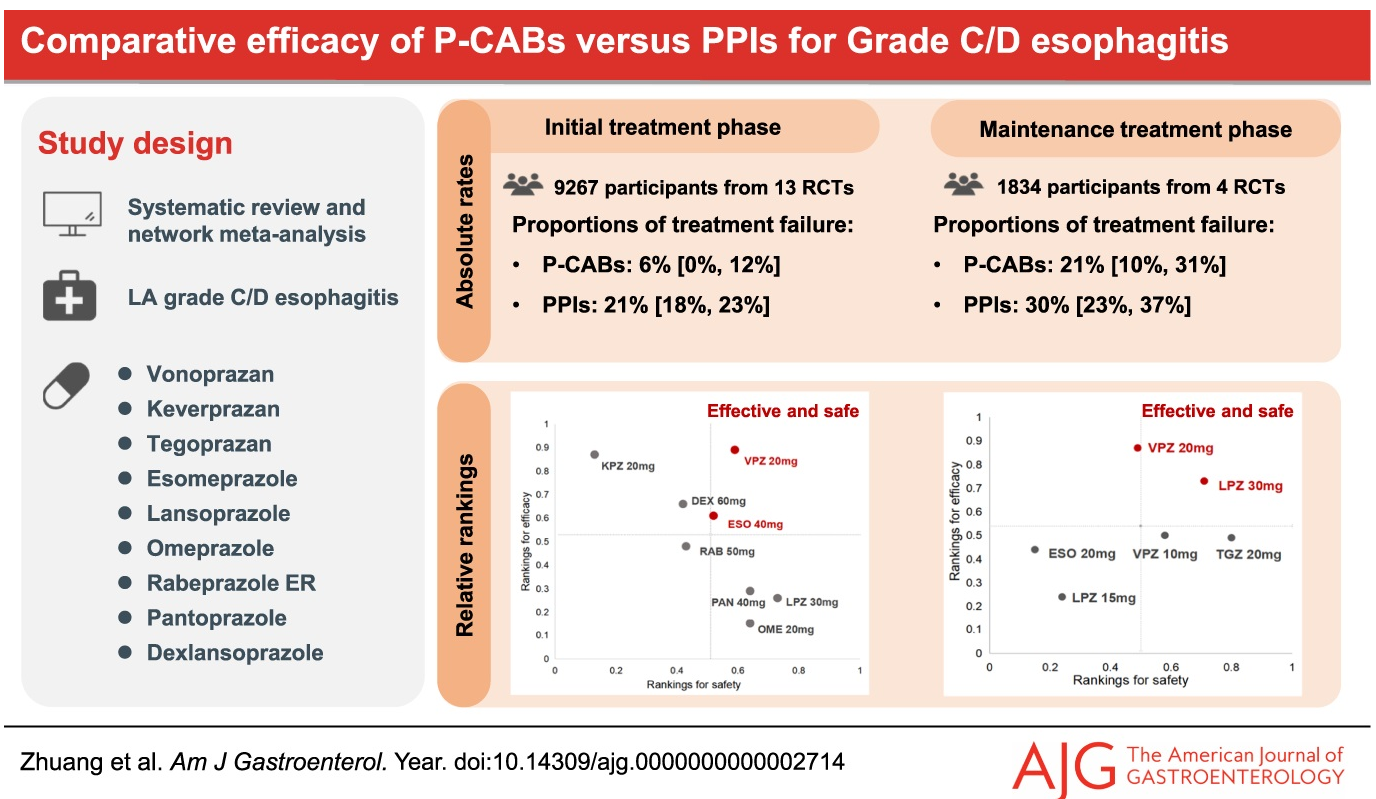
In this meta-analysis, 24 studies met criteria. Key findings:
Vonoprazan (20 mg) had the lowest rates of treatment failure: 6% in the initial treatment phase, and 21% in the maintenance phase of healing of grade C/D esophagitis
Vonoprazan had similar risk of incurring adverse events, severe adverse events, and withdrawal to drug when compared with PPI.
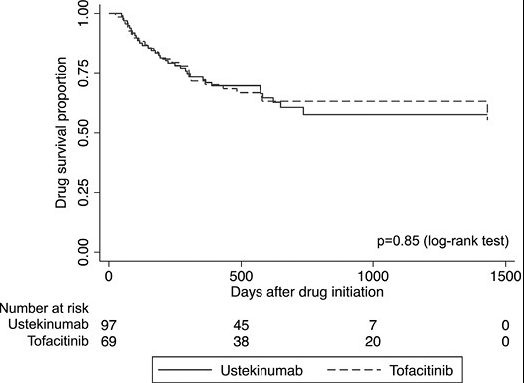
In this real-world cohort of anti-TNF-exposed patients with ulcerative colitis, tofacitinib (n=69) and ustekinumab (n=97) demonstrated similar effectiveness in achieving steroid-free clinical remission (SCFR) at 12 and 52 weeks. The median follow-up was 88.0 and 62.0 week, respectively. 35 of 66 in the tofacitinib cohort had dose reduction from the starting dose of 10 mg twice daily. This reduction occurred at a mean of 144 days. 59 of 97 in the ustekinumab cohort received either Q4W dosing (n=43) or Q6W (n=16).
Key findings:
53% of patients receiving tofacitinib and 32% of patients receiving ustekinumab achieved SFCR at 12 weeks. Tofacitinib-treated patients had higher baseline Mayo endoscopic subscores and CRPs.
At 52 weeks, approximately 50% of patients in both treatment groups achieved SFCR. There were also high proportions (>60%) of patients in both treatment groups who had endoscopic response within 52 weeks.
Both drugs were well-tolerated, as only 1 patient in each treatment group discontinued therapy due to an AE during >260 patient-years of follow-up.
My take: This shows similar response to either tofacitinib and ustekinumab in a cohort that had refractory disease as patients were anti-TNF failures and most had prior vedolizumab as well.
“Close don’t count in baseball.Close only counts in horseshoes and hand grenades.” –Frank Robinson 1973.
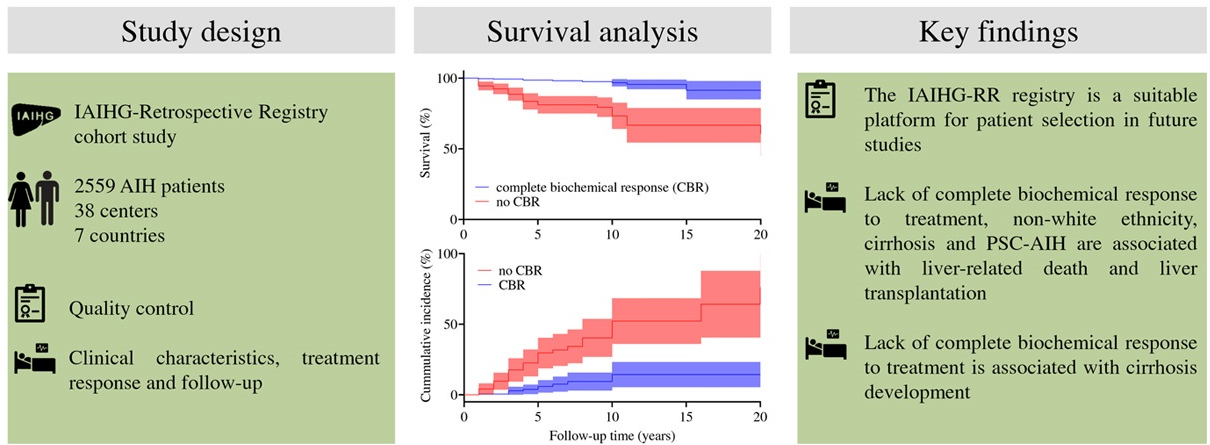
This study used the the International Autoimmune Hepatitis Group retrospective registry (IAIHG-RR), a web-based platform. This retrospective, observational, multicenter study analyzed 2559 patients; however, only 1700 had adequate follow-up. A complete biologic response (CBR) was defined as normalization of aminotransferases and serum IgG within 6 months; only 706 had serial results of these parameters to assess for a CBR.
Key findings:
Among the 706 with adequate data, 68.5% achieved a CBR.
Non-White ethnicity (HR 4), cirrhosis (HR 3.5), variant syndrome with primary sclerosing cholangitis (PSC) (HR 3.1), and lack of complete biochemical response within 6 months (HR 5.7) were independent prognostic factors.
Patients with a CBR had a greater actuarial survival over a 20-year period (91%) compared to those without a CBR (61%). Lack of a CBR at 6 months conferred a 3.6-fold higher risk of progression to cirrhosis.
Even in patients with cirrhosis, a CBR increased long-term survival: 82% versus 34%.
My take: A CBR is associated with the best long-term outcomes. My suspicion is that a biochemical response is actually similar to horseshoes. Improvement with treatment is likely beneficial but not as good as hitting the stake (the target).
Cyanobacteria are commonly found in water bodies and their production of hepatotoxins can contribute to liver damage.
Methods: Across the contiguous United States, regions with high cyanobacteria exposure (CE) counts in water bodies were identified using satellite remote sensing data. The data were geospatially mapped to county boundaries, and disease mortality and incidence rates were analyzed.
Key findings:
There was a highly significant spatial association between CE, liver disease, and liver cancer. In Figure 4, the counties in the top half of CE had higher liver cancer. The mean CE 569.6 in the top half compared with median counts of CE of 319.5 in the bottom half of CE
Counties with CE exceeding the 80Th percentile for >8 or more years had as significantly higher liver cancer age-adjusted incidence rate (mean 9.48) compared with that did so for 5 or fewer years (mean=8.79)
Hot spots of CE and mortality were identified along the Gulf of Mexico, eastern Texas, Louisiana, and Florida, and cold spots across the Appalachians.
Cyanotoxins were detected in 62% of US counties using remote sensing.
My take: This study shows an association between areas with higher CE exposure and increased risk of liver cancer. This could be mediated via contaminated water exposure.
D Khullar et al. NEJM 2024; 390: 965-967. Vertical Integration and the Transformation of American Medicine
This article examines the growing trend of hospital acquisition of physician practices.
Some excerpts:
“From July 2012 through January 2018, the share of practices owned by a hospital increased from 14% to 31%, according to data from the Physicians Advocacy Institute; from January 2019 to January 2022, hospitals acquired 4800 additional practices, and about 58,000 more physicians became hospital employees.”
“In theory, vertical integration (the combining of organizations operating at different levels of production into a single entity) in health care can lead to improved patient outcomes — for example, by promoting care coordination, information exchange, and economies of scale. To date, however, the most consistent documented effect of such transactions has been an increase in prices.”
Increased prices are due to multiple factors including strengthened negotiating position, “facility fees” that are added to services delivered by hospital-owned practices.1, increased tests and procedures in hospital settings, higher payor rates, and in many cases discounted outpatient drug prices (for those qualified in 340B program)
“The limited research in this area suggests that vertical integration doesn’t tend to result in meaningful improvements in quality of care, with some studies finding that it may lead to poorer quality, if health systems take resources away from unprofitable services and redistribute them to more lucrative ones.2“
“Hospital acquisitions of physician practices have gone largely unreviewed by agencies such as the Federal Trade Commission (FTC) and the Department of Justice (DOJ)…In December 2023, the FTC and the DOJ issued new antitrust guidelines that could strengthen the agencies’ approach to vertical integration in health care “
“Many clinicians may be satisfied after their practice is acquired; they may, for example, have an improved work–life balance, receive greater administrative support, and be relieved of managing the business-related aspects of medicine. Alternatively, they may work longer hours, have less autonomy and constrained job mobility, and experience more burnout or moral injury.”
“The rapid acquisition of physician practices by hospitals highlights an important tension in health care — between the possibility that integration can promote efficiency and improved quality and the concern that it distorts markets and can worsen health and financial outcomes.”
My take: There are clear financial incentives for hospitals to acquire physician practices. This trend leaves patients facing higher costs and clinicians dealing with less autonomy. Regulatory efforts face a difficult task to limit this widespread anti-competitive practice which at this point is akin to extracting a large trichobezoar from the stomach.
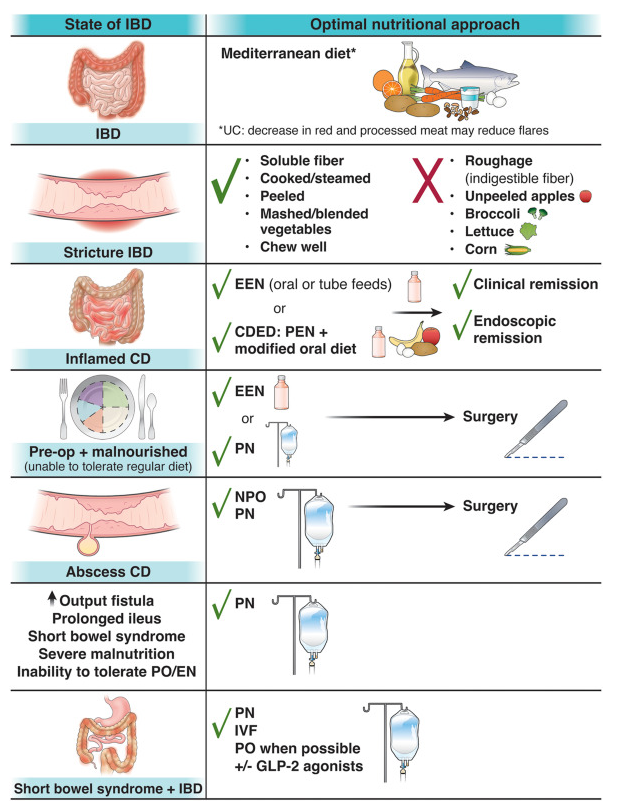
There are 12 “best practice” recommendations. Here are a few of them:
Best Practice Advice 1: Unless there is a contraindication, all patients with IBD should be advised to follow a Mediterranean diet rich in a variety of fresh fruits and vegetables, monounsaturated fats, complex carbohydrates, and lean proteins and low in ultraprocessed foods, added sugar, and salt for their overall health and general well-being. No diet has consistently been found to decrease the rate of flares in adults with IBD. A diet low in red and processed meat may reduce ulcerative colitis flares, but has not been found to reduce relapse in Crohn’s disease.
Best Practice Advice 3: Exclusive enteral nutrition using liquid nutrition formulations is an effective therapy for induction of clinical remission and endoscopic response in Crohn’s disease, with stronger evidence in children than adults. Exclusive enteral nutrition may be considered as a steroid-sparing bridge therapy for patients with Crohn’s disease.
Best Practice Advice 6: In patients with IBD who have an intra-abdominal abscess and/or phlegmonous inflammation that limits ability to achieve optimal nutrition via the digestive tract, short-term parenteral nutrition may be used to provide bowel rest in the preoperative phase to decrease infection and inflammation as a bridge to definitive surgical management and to optimize surgical outcomes.
Best Practice Advice 7: We suggest the use of parenteral nutrition for high-output gastrointestinal fistula, prolonged ileus, short bowel syndrome, and for patients with IBD with severe malnutrition when oral and enteral nutrition has been trialed and failed or when enteral access is not feasible or contraindicated.
Best Practice Advice 10: All patients with IBD should be monitored for vitamin D and iron deficiency. Patients with extensive ileal disease or prior ileal surgery (resection or ileal pouch) should be monitored for vitamin B12 deficiency.
Best Practice Advice 12:Breastfeeding is associated with a lower risk for diagnosis of IBD during childhood. A healthy, balanced, Mediterranean diet rich in a variety of fruits and vegetables and decreased intake of ultraprocessed foods have been associated with a lower risk of developing IBD.
“The FDA cautions that microorganisms contained in probiotics have been reported in the medical literature as causing bacteremia or fungemia, sometimes with a severe clinical course, in very preterm or very low birthweight (VLBW) infants.”
“Moreover, the American Academy of Pediatrics states ‘Given the lack of FDA-regulated pharmaceutical grade products in the United States, conflicting data on safety and efficacy, and potential for harm in a highly vulnerable population, current evidence does not support the routine, universal administration of probiotics to preterm infants, particularly those with a birth weight of <1000 g.’”
“The FDA is also reminding healthcare providers that FDA has not approved any probiotic product for use as a drug or biological product in infants.”
My take: Despite promising studies (over the last 20 years) indicating that probiotics reduce the risk of necrotizing enterocolitis and death, this appears to be the end of the line for the use of probiotics for preemies in the U.S. To change course, there would need to be a pharmaceutical-grade probiotic and proof that it was a reliable high-quality agent meeting FDA standards along with subsequent studies showing this probiotic was effective.
Probiotics in Preemies: Lifesaving Therapy Lots of studies have indicated that probiotics may be beneficial in premature newborns; the problem is that there are currently no FDA-approved probiotics for preterm infants. The use of probiotics as a non-regulated FDA product leads to the potential risk of contamination due to inconsistent quality control as well as variability in the strains and concentrations. The risks are not inconsequential as there has been a report of 29-week infant who died from mucormycosis due to probiotic contamination with mold.
Background: This retrospective single-center study examined the transfusion threshold in children 6 months to 36 months (mean 18.5 months, n=125) in light of current society recommendations which advise against blood transfusion in hemodynamically stable children with iron deficiency anemia.
Key findings:
“A hemoglobin of 39 g/L had sensitivity 92% and specificity 72% for transfusion.”
In this study, there were 38 children with a hemoglobin <50 g/L who were NOT transfused
Discussion points:
“There is a paucity of evidence to support a hemoglobin threshold for transfusion in the management of iron deficiency anemia (IDA)….McEvoy et al recently developed an algorithm for the management of young children with IDA in the ED with a consensus of surveyed hematologists recommending a hemoglobin of <50 g/L be used for transfusion.”
In one study, “the median time to increased hemoglobin by at least 20 g/L…was 7 days for children receiving iron sucrose and 44 days for children receiving oral iron alone.”
My take: In children without active bleeding who are hemodynamically stable, more restrictive use of transfusion is now standard practice. In clinical practice, the exact threshold for transfusion is not clear. This study suggests that it is somewhere between 3.9 g/dL and 5 g/dL.
Related blog posts (regarding anemia and active bleeding):
All Bleeding Stops (part 2) “A randomized trial showed lower rates of death (the primary outcome), rebleeding, and adverse events with a transfusion threshold of 7 g per deciliter than with a transfusion threshold of 9 g per deciliter.”
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
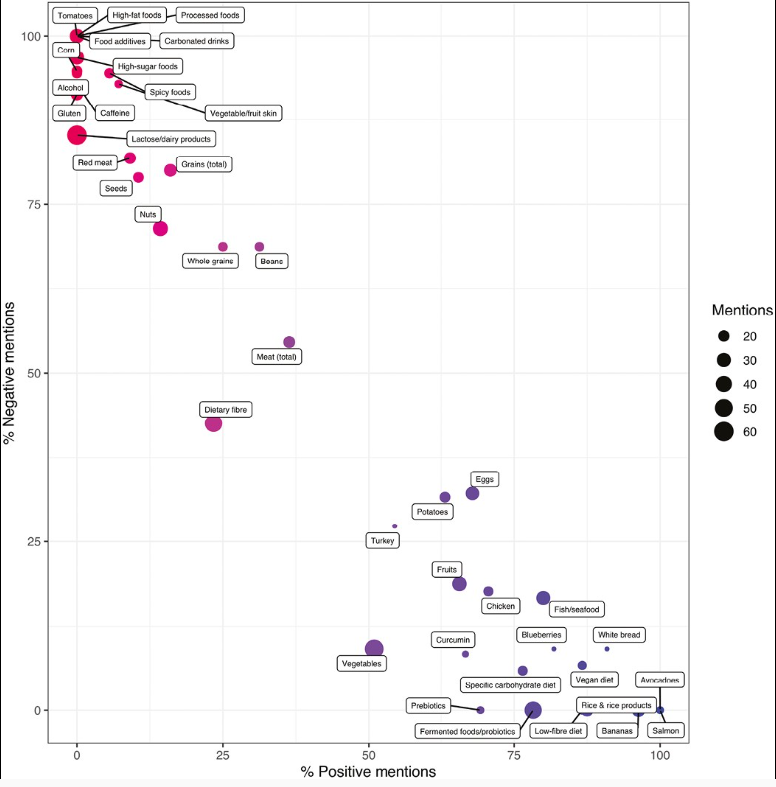
The authors assessed videos discussing dietary aspects (food, diet-related items, and advisory comments [FODRIACs]) on YouTube. Of 1800 videos screened, a total of 160 were included in the final analysis.
Background: “Currently, the only well-established dietary treatment in IBD is exclusive enteral nutrition (EEN), which is used for induction of remission mostly in pediatric CD.5,6 Over the past 2 decades, several food-based exclusion diets have been suggested as potential treatments for CD and UC, some of which demonstrated promising efficacy signals such as the CD-TREAT (Crohn’s disease treatment with eating) diet and the CDED (Crohn’s disease exclusion diet).7-9 Nonetheless, current societal guidelines do not recommend the use of any solid food–based exclusion diet as a treatment option for the induction or maintenance of clinical remission in IBD.6“
Key findings:
Foods pertinent to a prudent dietary pattern (ie, fish, chicken, avocado, blueberries), foods high in pre- and probiotics, and certain food exclusion diets (eg, SCD) were primarily portrayed as beneficial.
Foods often associated with a Western dietary pattern, including processed foods, high-sugar foods and high-fat foods, red meat, and alcohol, were considered detrimental for disease outcomes in patients with IBD.
Neutral opinions were expressed about fiber and vegetables.
There was a higher video interaction rate and number of likes in patient-generated videos compared with videos from healthcare professionals.
Only 3% of all patient videos and 35% of videos from healthcare professionals cited any form of scientific evidence.
Problems with diet advice is that extensive dietary restrictions and adherence to extreme diets may lead to the development of disordered eating as well as nutrient deficiencies (nutritionist involvement is important to avoid this). In addition, reliance on unproven diets may lead some patients to forgo proven therapies.
My take: Though there are some overlapping advice in these videos, much of the dietary advice on YouTube (and elsewhere) is conflicting. In part, this reflects the lack of evidence-based dietary guidelines for IBD. Physicians should review information on dietary therapies at diagnosis and request that families contact them (or well-qualified nutritionists) when considering dietary modifications.
Since baseball season is now getting started, I wanted to share this news story (which is a real story and not The Onion):
An excerpt:
“For more than a quarter-century, Phillies fans considered dollar hot dog night among the best ballpark promotions — but the team has now decided it was the wurst…Armed with projectile frankfurters, some unruly Phillies fans began chucking their favorite Hatfield meat during a game last year, and the dogs soared like cans of corn throughout the stands and onto the field…”
“It wasn’t just the throwing,” said John Weber, senior vice president, Phillies ticket operations and projects. “It’s the concourse, the crowds of everybody being at the same X amount of stands. But obviously, you know, the throwing was a little bit of a tipping point…”
“Hey, there is still a chance in Philly to always snag a free hot dog — just catch one out of the Phanatic’s famed hot dog launcher.”