Another terrific lecture from David Rubin: Positioning of Advanced IBD Therapy. Here are my notes and some slides which could include errors in transcription and omission. Can get access to all 46 slides here: IBD Pro CCFA 2023 Atlanta
Many challenges in sequencing treatment -heterogeneity of diseases, loss of response, challenges in interpreting data, understudied issues (perianal disease, extra-intestinal manifestations, psychological health).
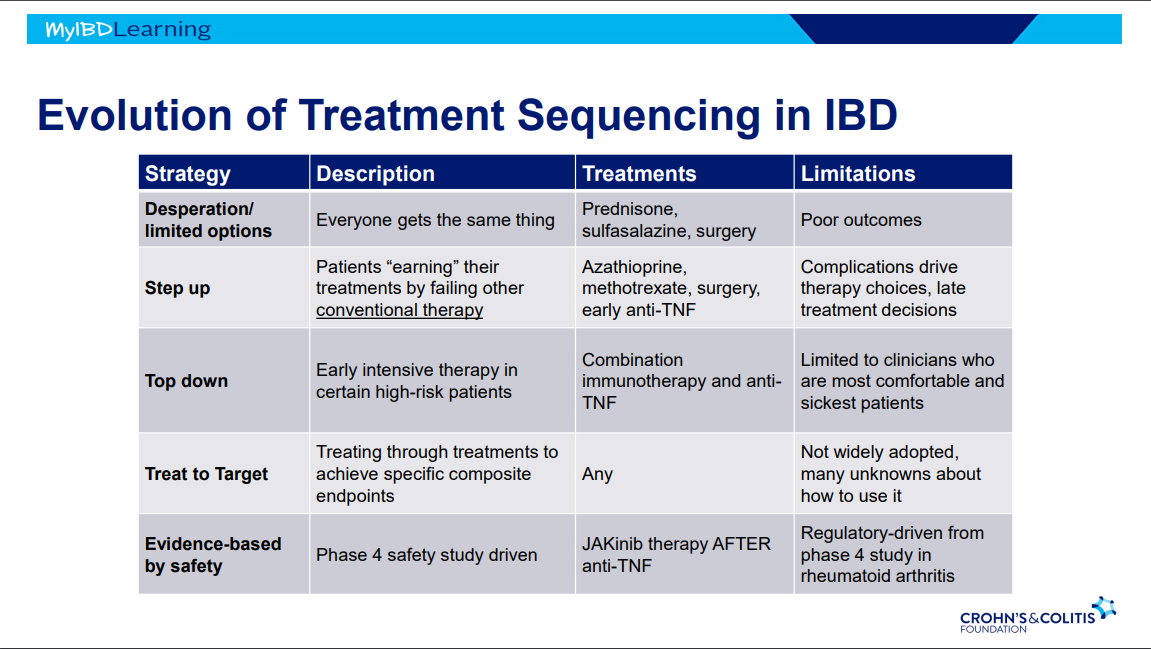
Evolution of therapies: desperation era -limited options, step up era, top down era with anti-TNFs, treat to target era and currently evidence-based by safety era.
It is possible to avoid steroids in many patients with upcoming plans to use an advanced therapy -this is probably beneficial. This may result in patients remaining symptomatic until these therapies can be started.
JAK inhibitors cannot be given as first-line agent in U.S. (but is done in other countries).
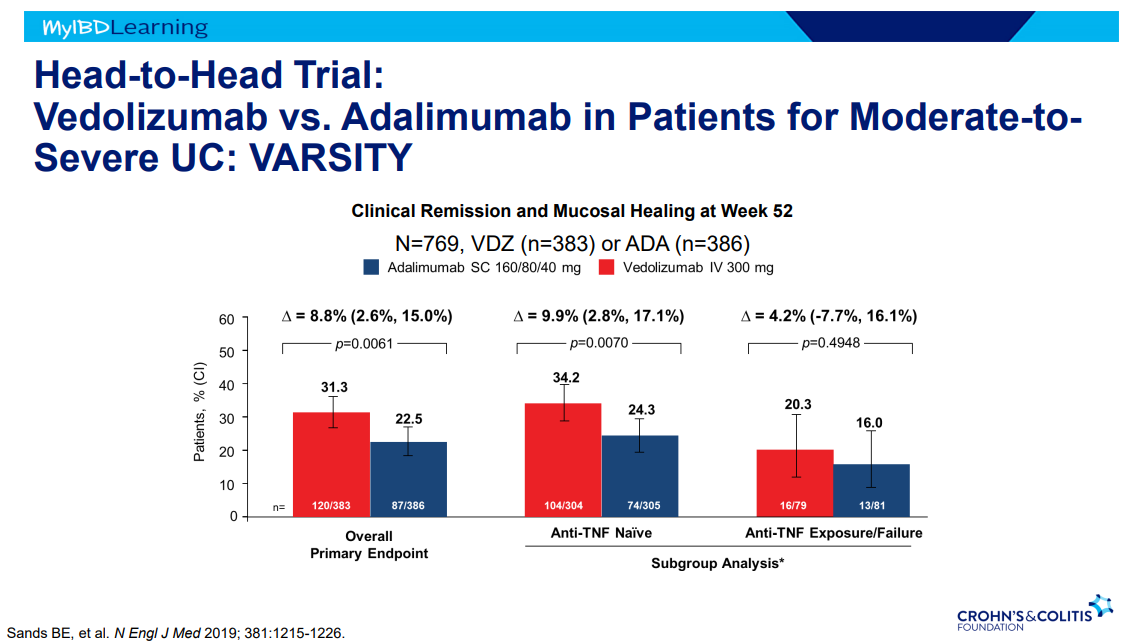
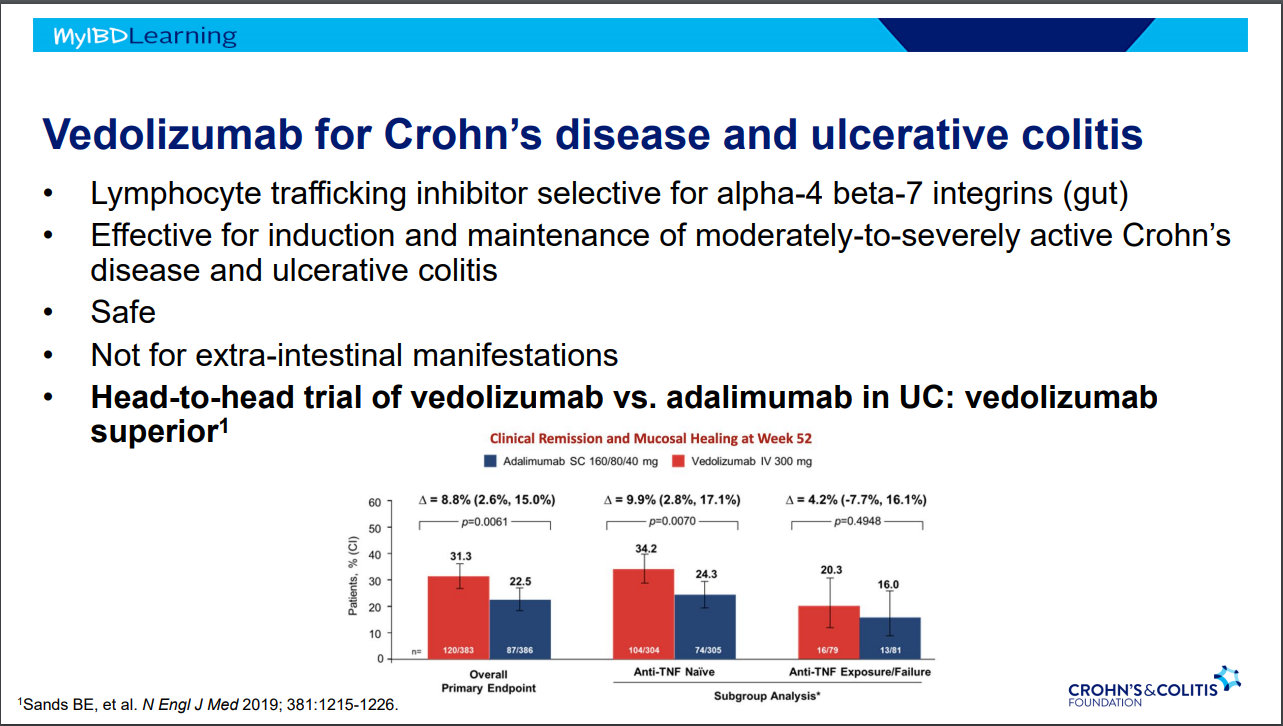
VARSITY trial enrolled patients with prior anti-TNF exposure (but not adalimumab) which biased the study against adalimumab vs vedolizumab
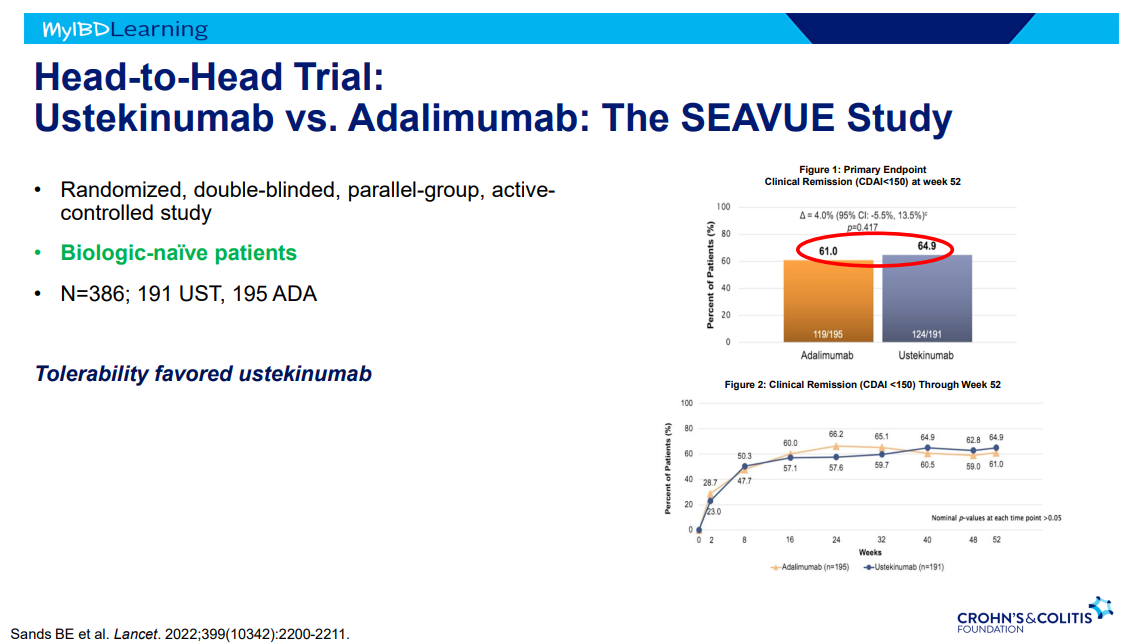
SEAVUE study ~65% in clinical remission at 1 yr with both adalimumab and ustekinumab; though, ustekinumab had better tolerability
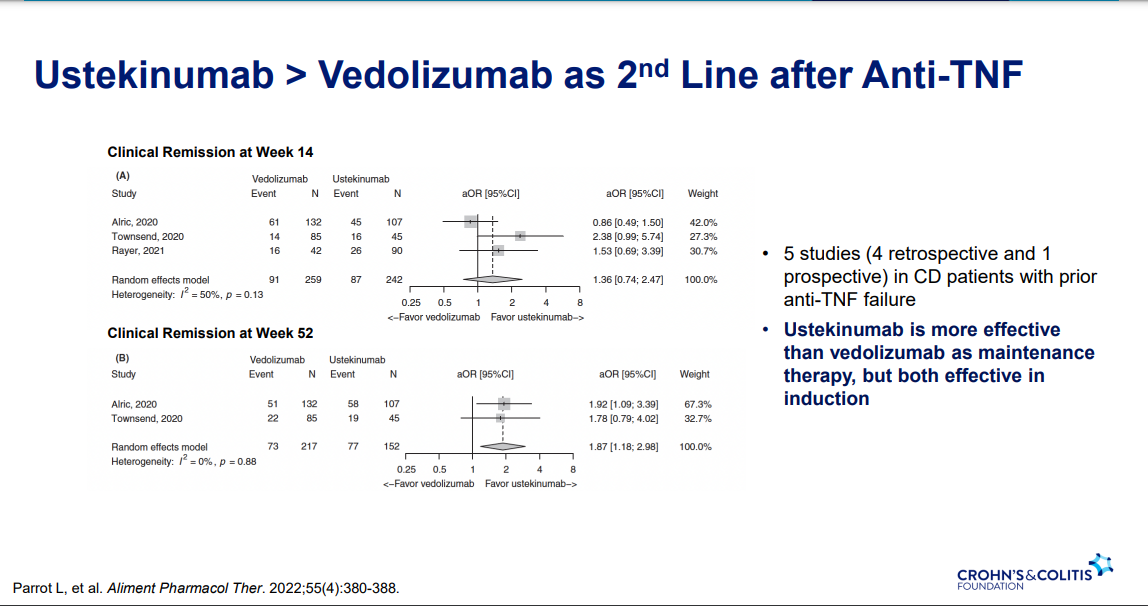
Ustekinumab better 2nd line treatment for CD after anti-TNF (Parrot et al. AP&T 2022; 55: 380-388
Vedolizumab is a good therapy for CD, especially in biologically-naïve
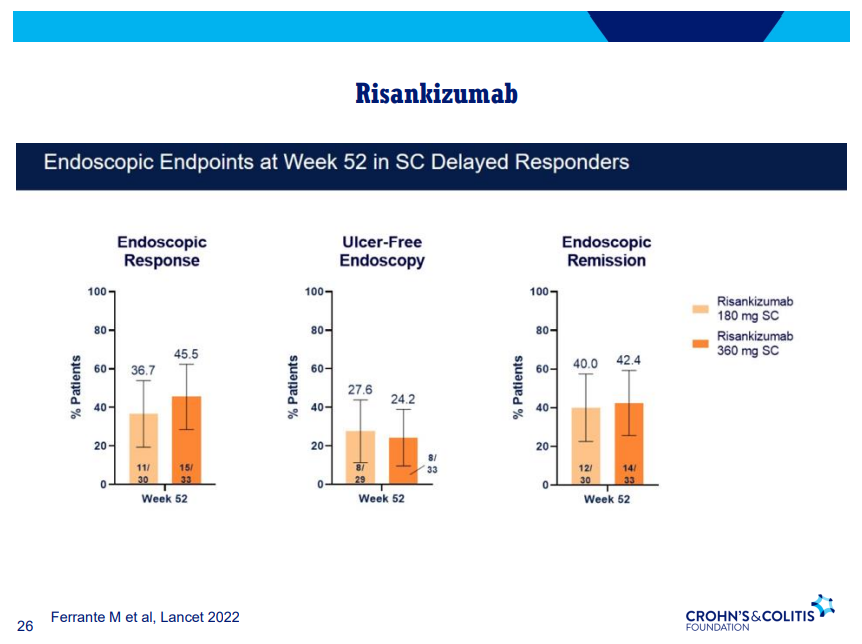
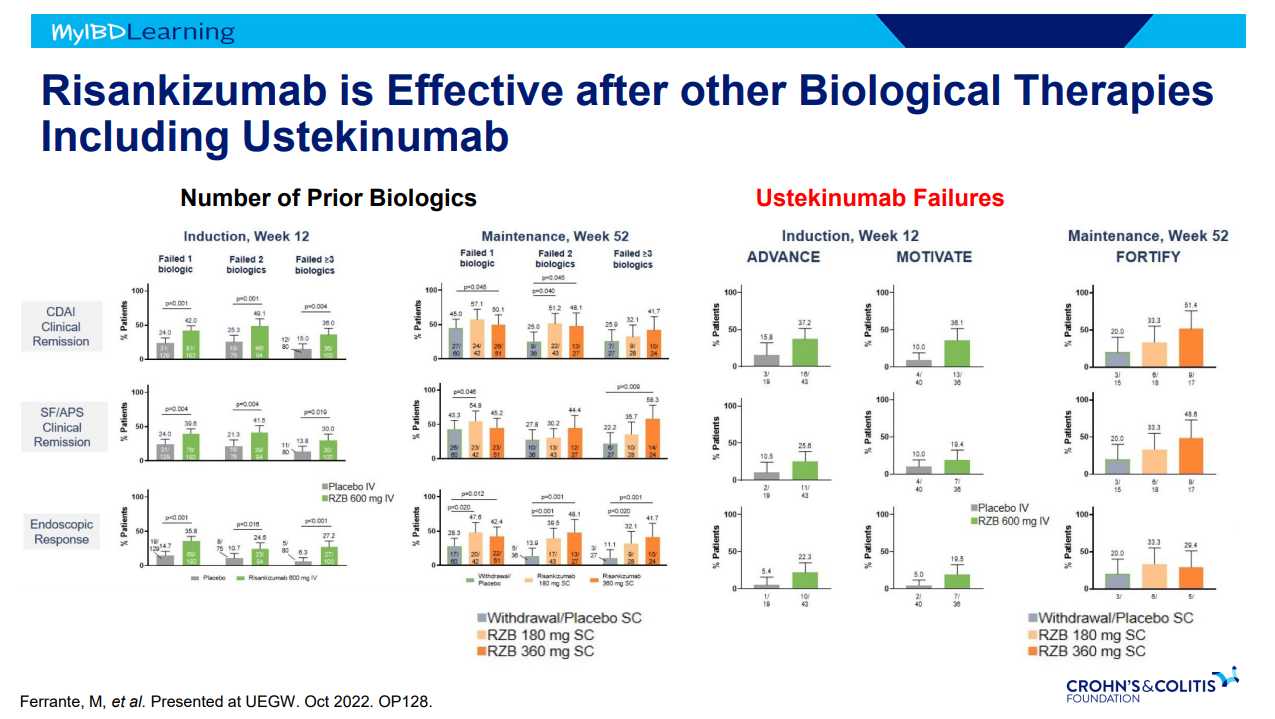
Risankizumab good for moderate-severe CD both in biologically-naïve and biologically-experienced
Dose reduction in maintenance of Jak inhibitors can result in LOR and 50-75% can achieve response after resumption of higher dosing
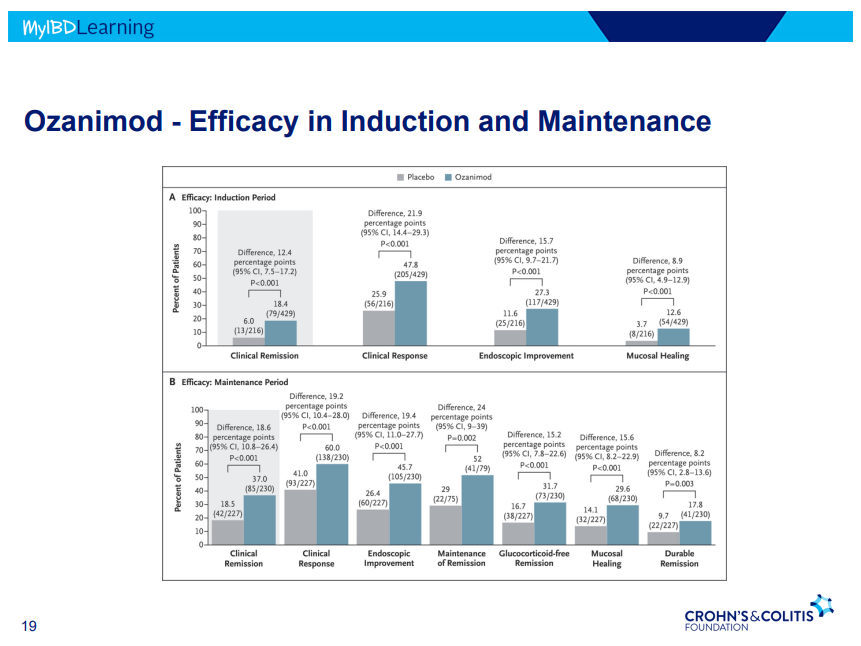
This is third day summarizing some of the talks at the regional CCFA conference. Erin Forster presented on Treatment with Oral Advanced Therapy. Below are my notes and some of the slides; my notes may have errors of omission or transcription. Can get access to full slide set: (n=22) here: Treatment with Oral Advanced Therapy
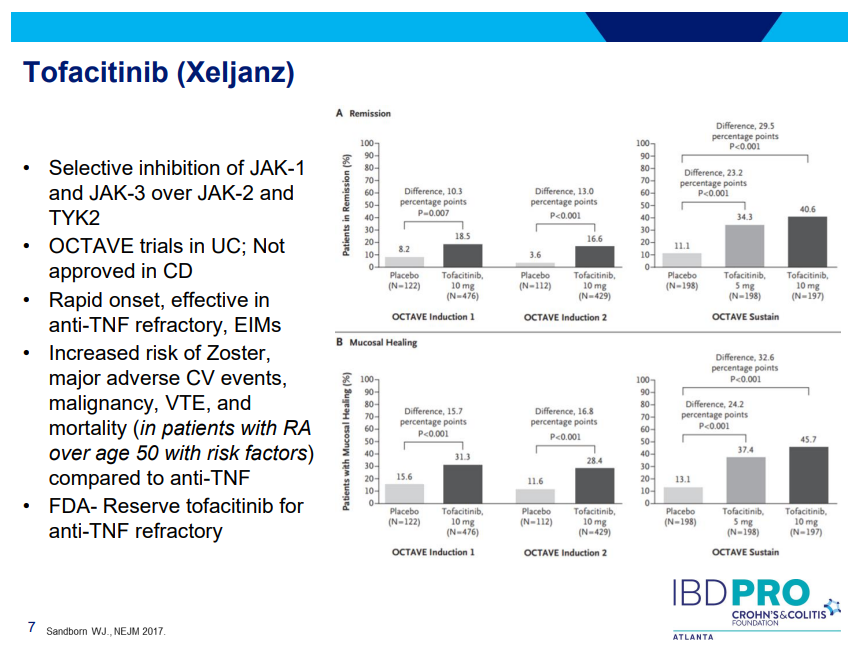
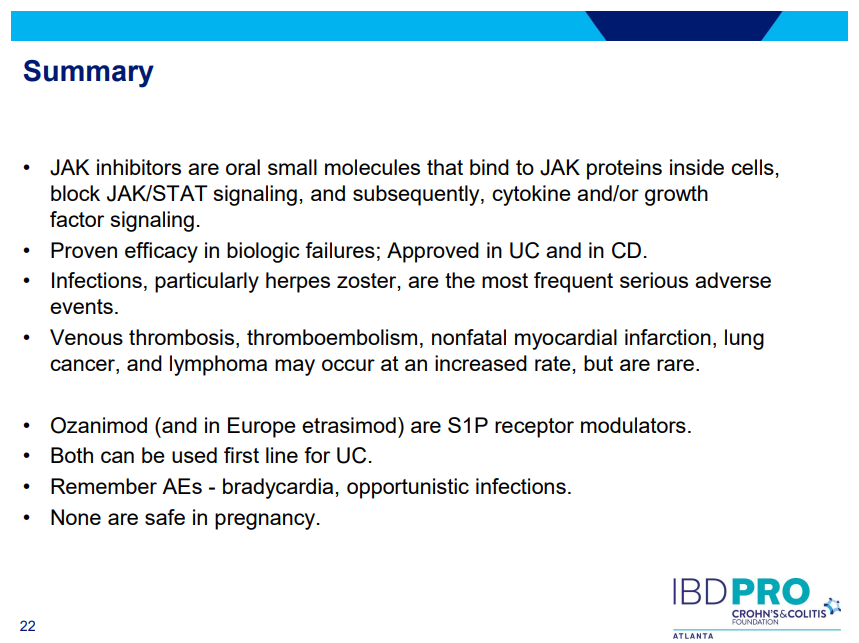
JAK inhibitors (Tofacitinib, Upadacitinib) have rapid onset of action and are taken orally
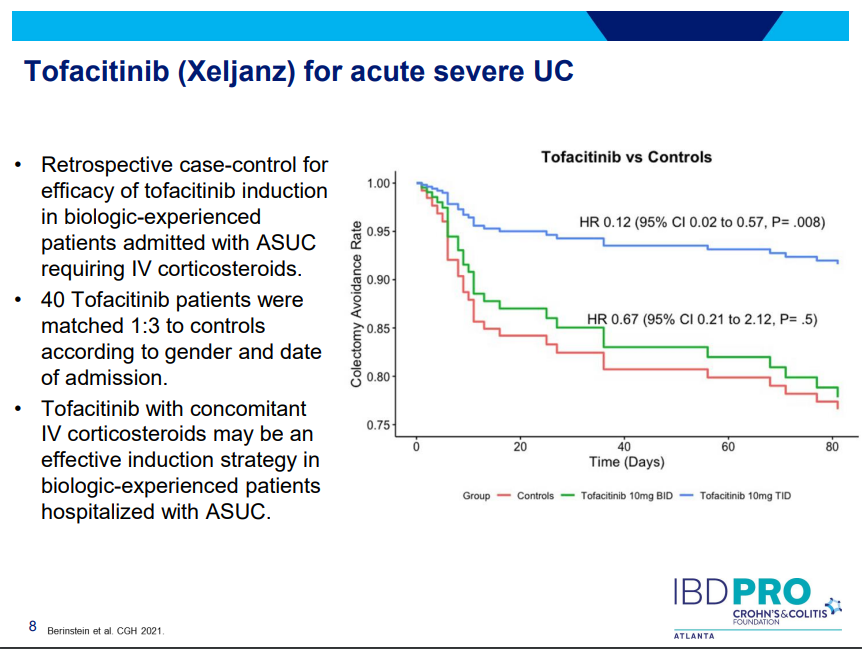
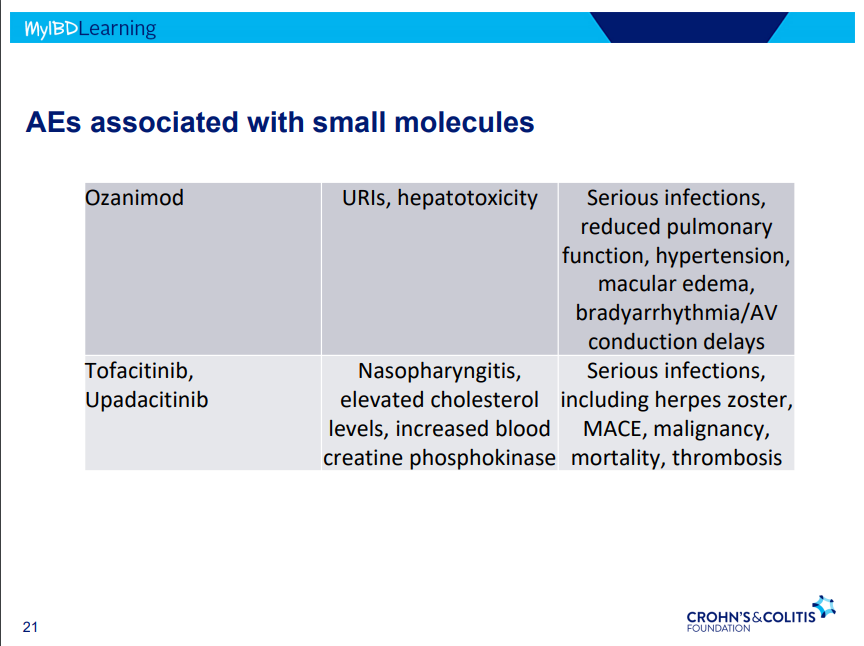
Tofacitinib (Xeljanz) -concern about cardiovascular events was derived from elderly rheumatologic patients. Cardiovascular events are rare. Higher dose (TID) (in the hospital) associated with lower colectomy rates in acute severe ulcerative colitis.
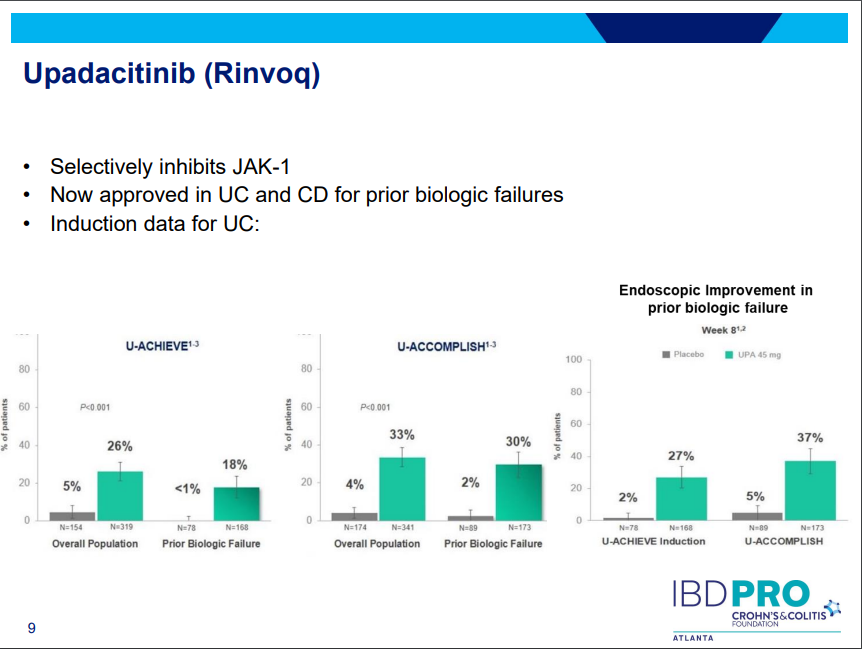
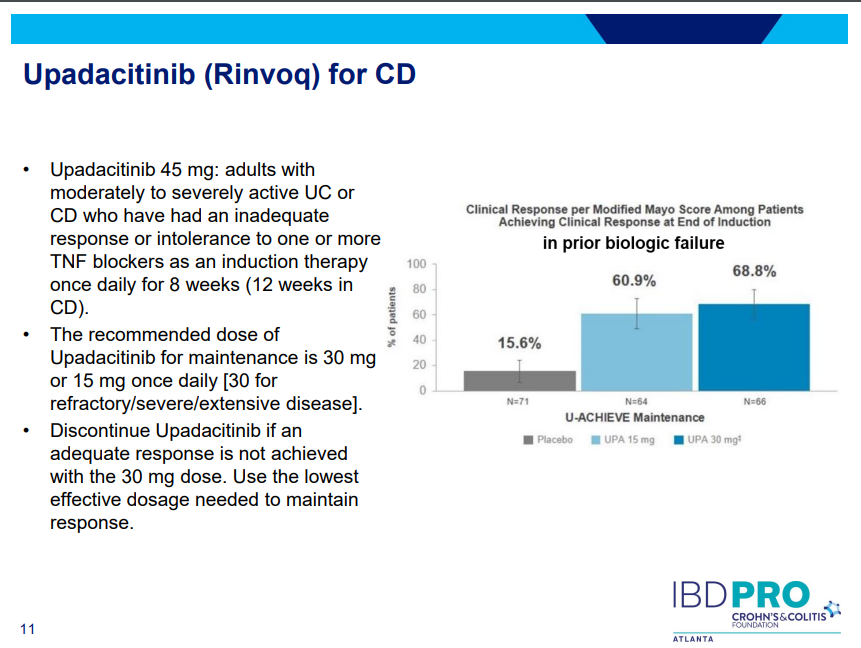
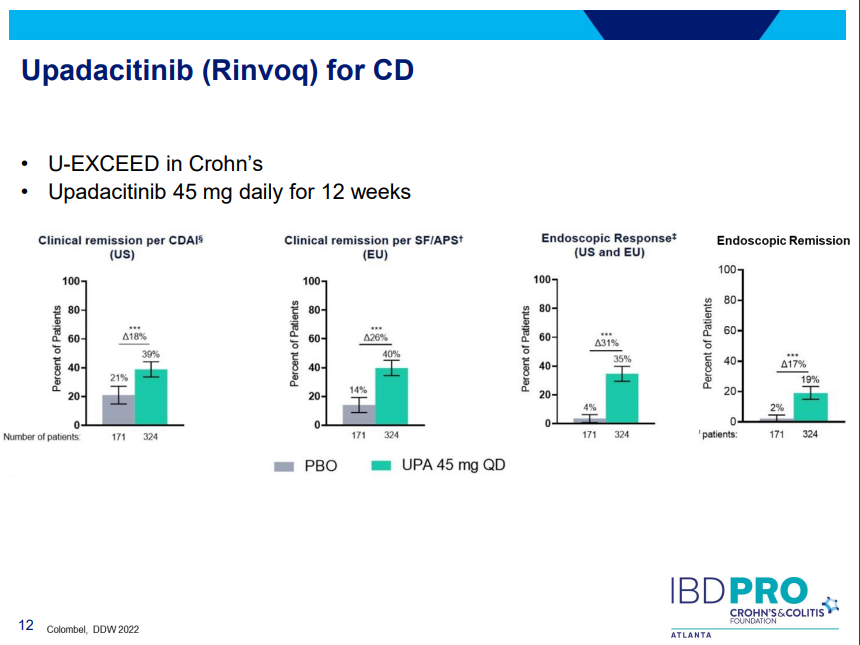
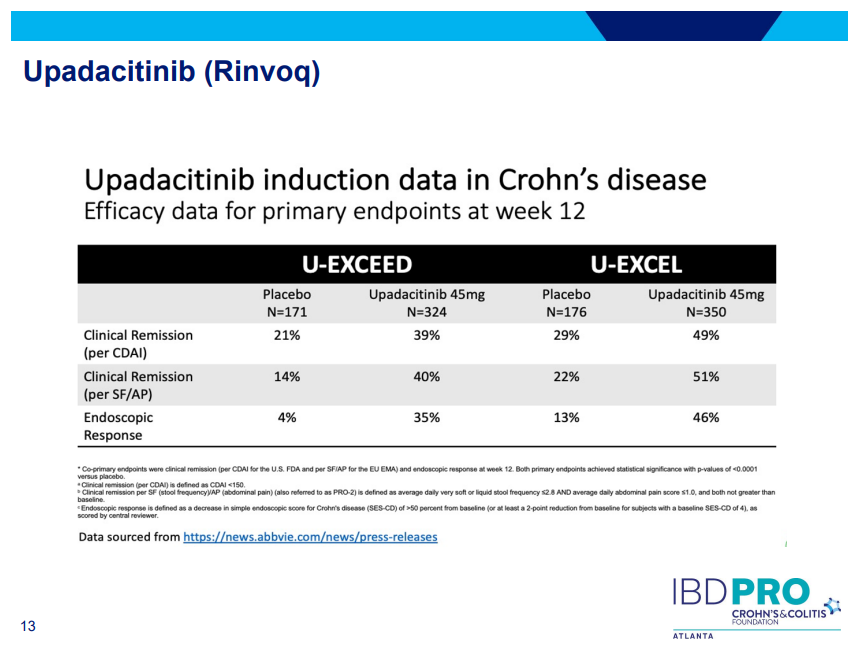
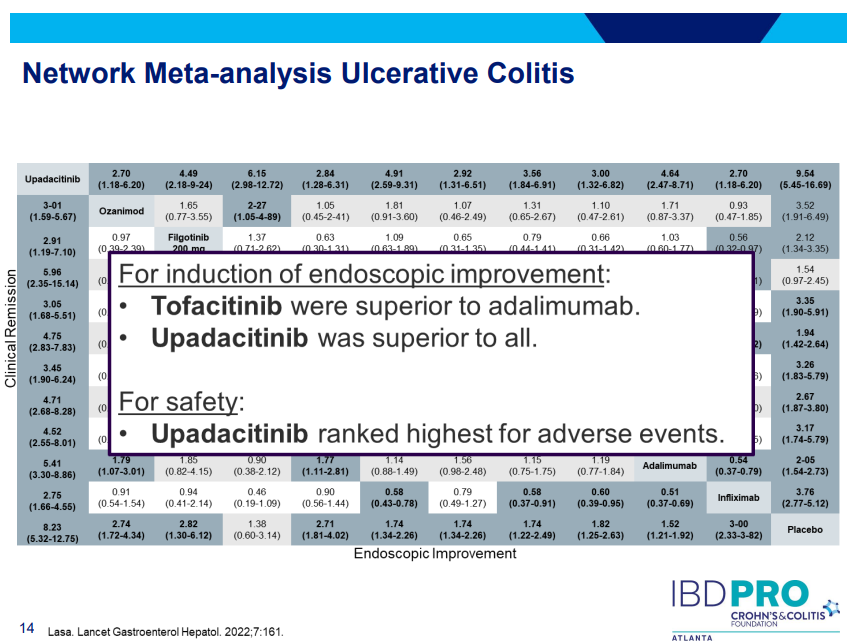
Upadacitinib (Rinvoq) -now approved for CD and UC. Higher dosing could affect liver function (especially if underlying liver disease). Also, JAK inhibitors as a class have similar safety concerns: increased herpes zoster and concerns for cardiovascular concerns (esp if >50 years)..
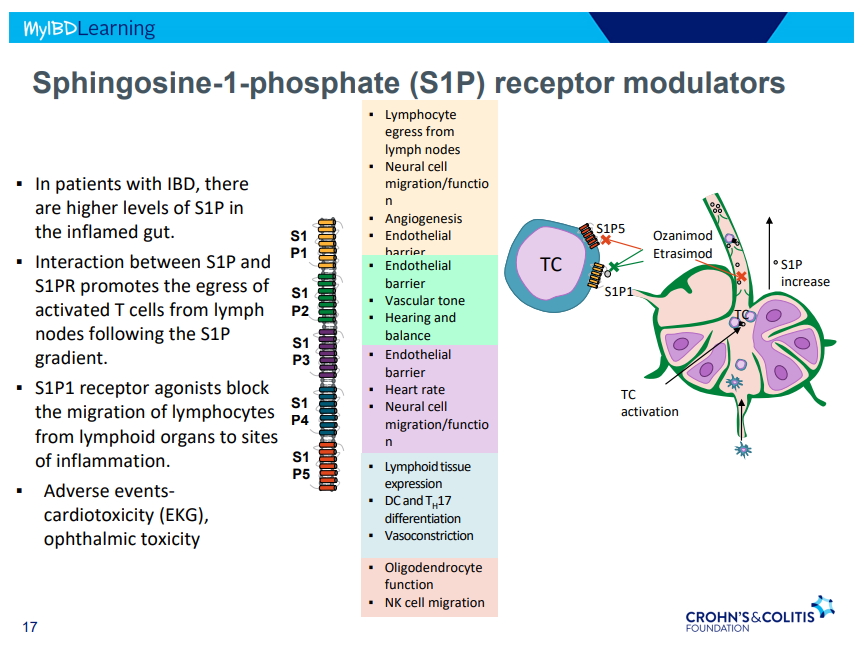
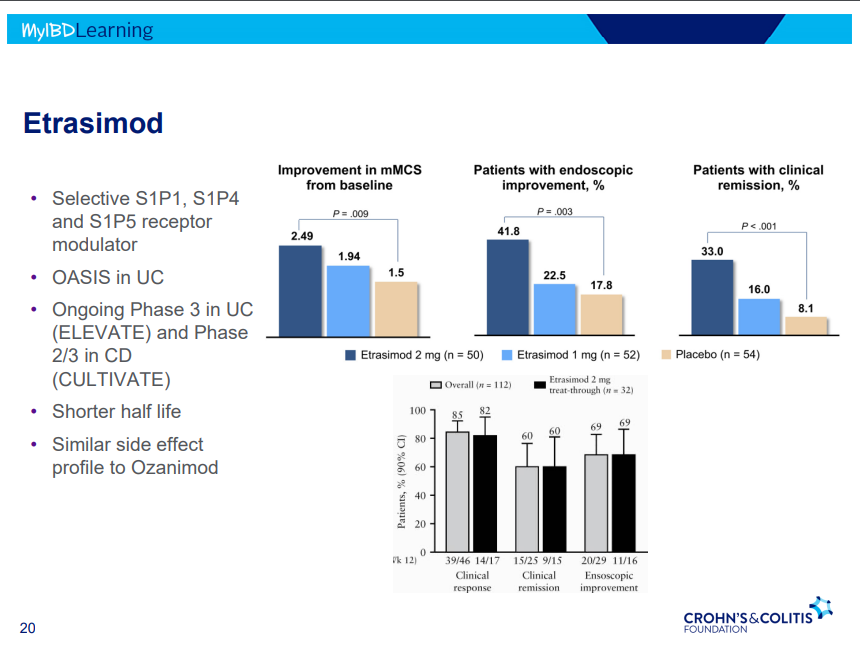
S!P receptor modulators: Oznaimod, Etrasimod & Amiselimod. Can cause bradycardia -have to check EKG prior.
There were a bunch useful lectures at CCFA 2023 regional conference in Atlanta. Here are some of my notes and slides from Doug Wolf‘s lecture; my notes may have errors of omission or transcription. Can get access to full slide set (n=37) here: Dose Escalation of Biologic Therapy and Dual Biologic Therapy
If loss of response to anti-TNF, consider dose escalation by either re-induction or increasing (doubling) dose. Re-induction is less costly
Dose escalation generally not effective for vedolizumab
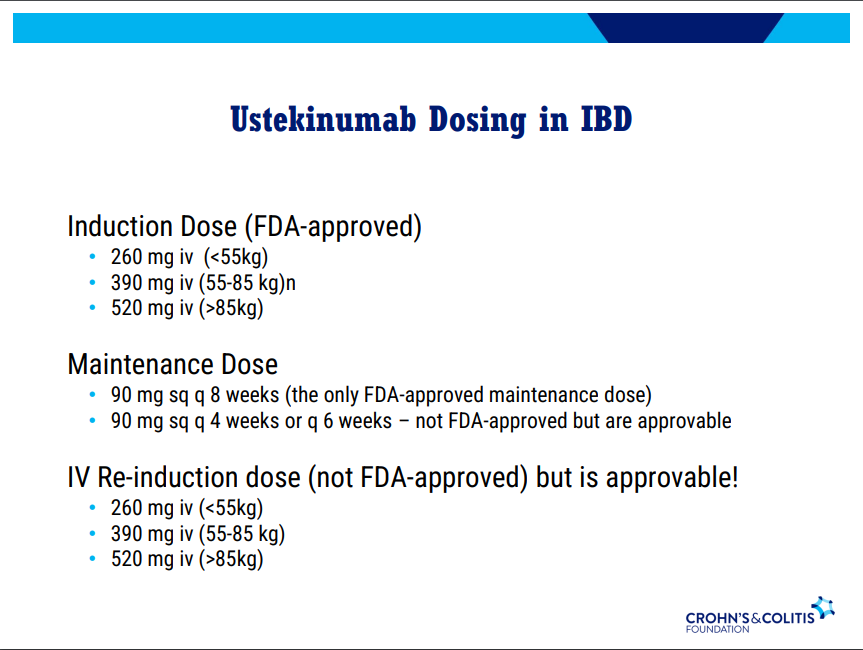
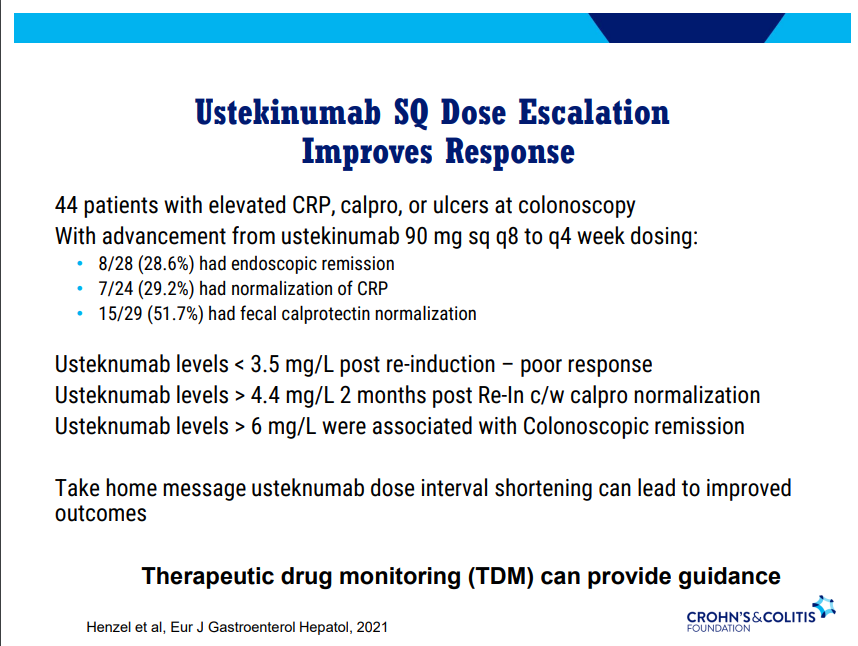
Dose escalation (increased frequency) with ustekinumab can be effective. Therapeutic drug monitoring can provide guidance. Re-induction can also be effective in half of patients (especially in patients with either no prior biologics or one prior biologic)
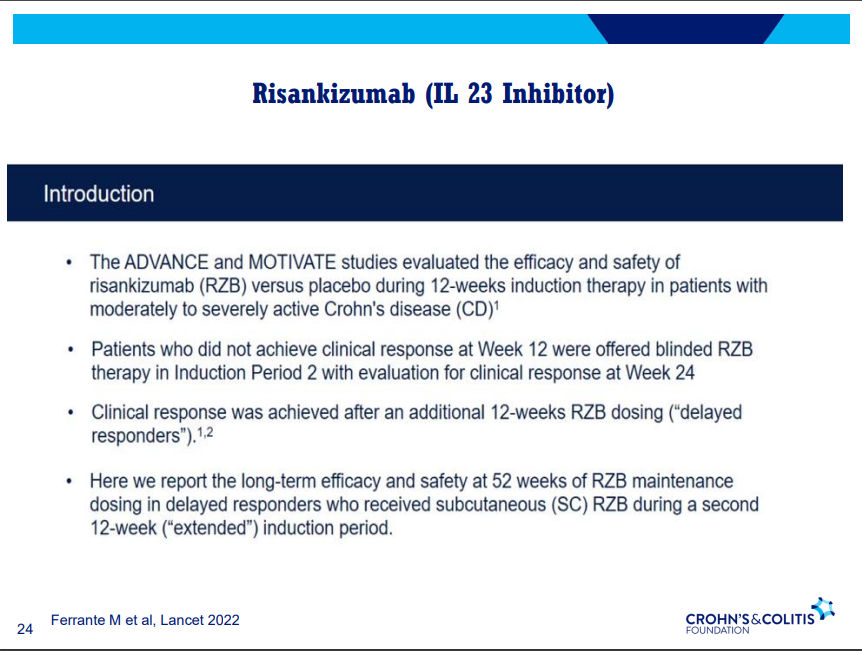
Risankizumab can still work in patients who had not responded by 12 weeks (delayed responders)
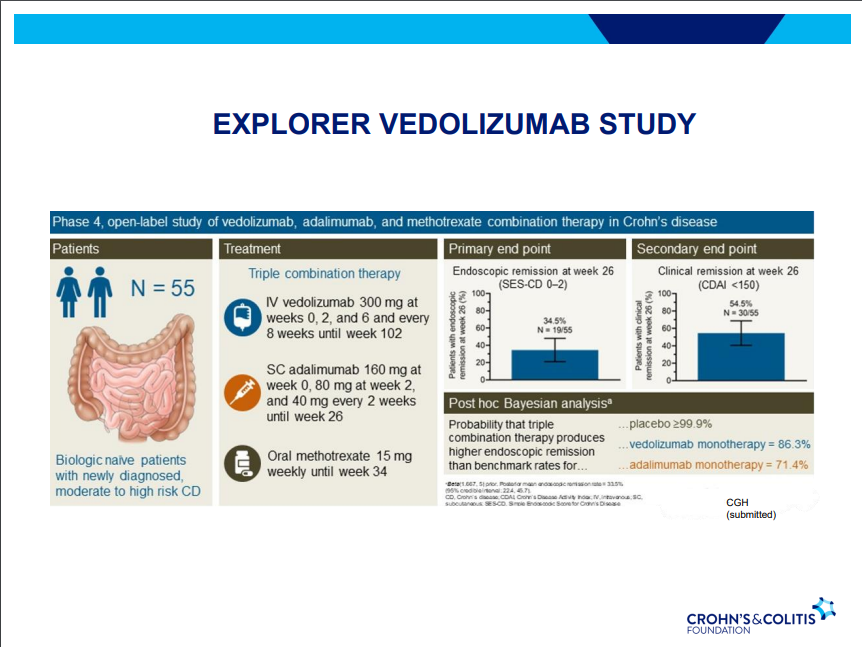
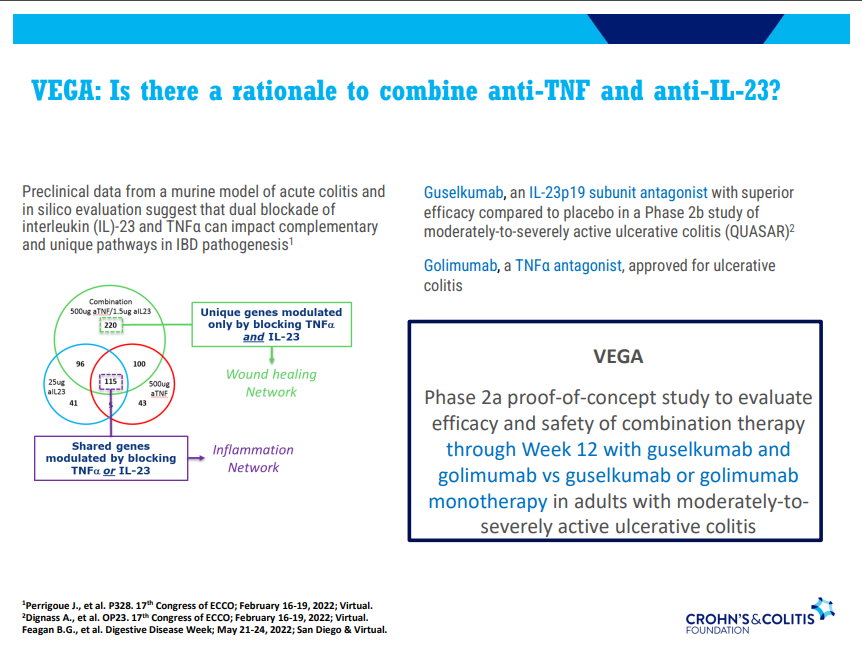
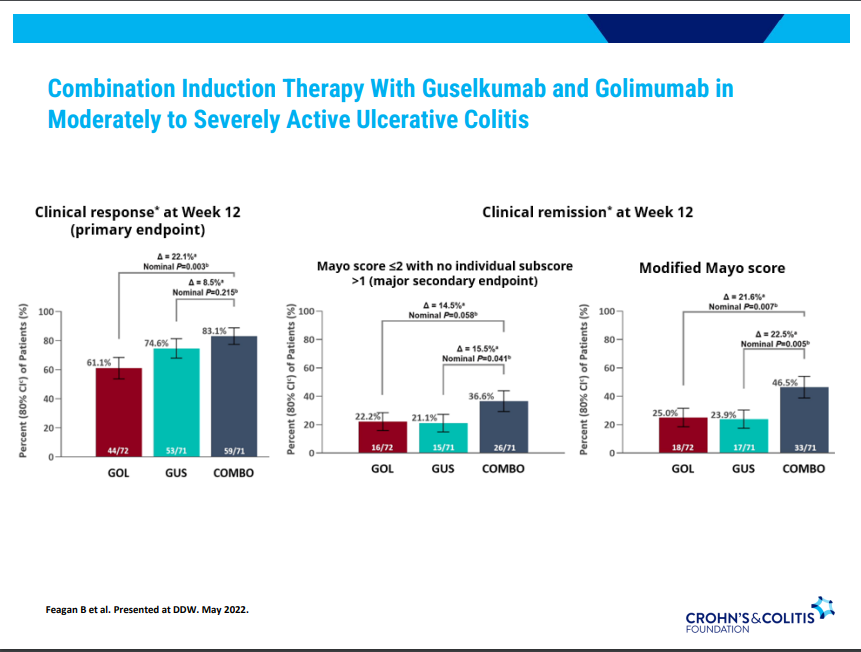
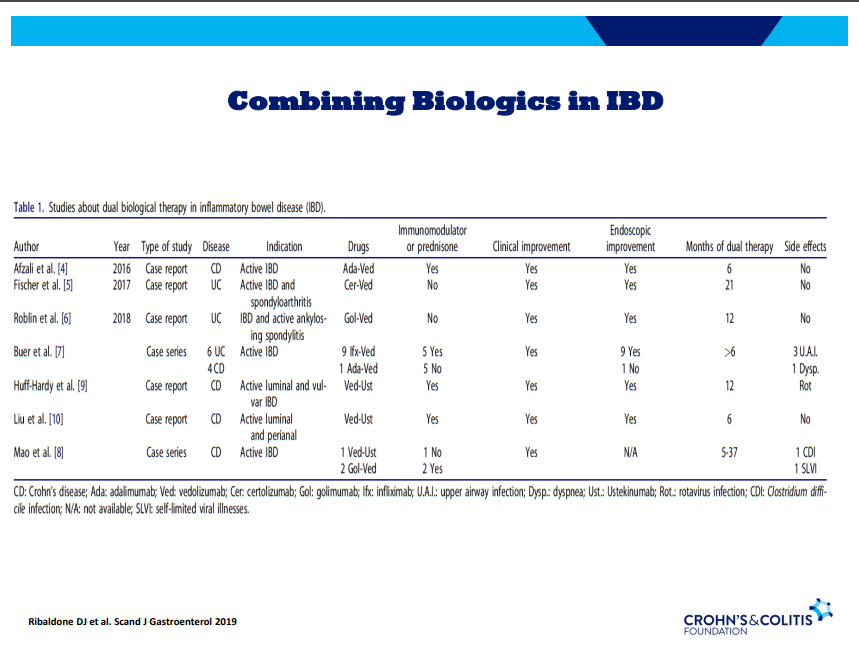
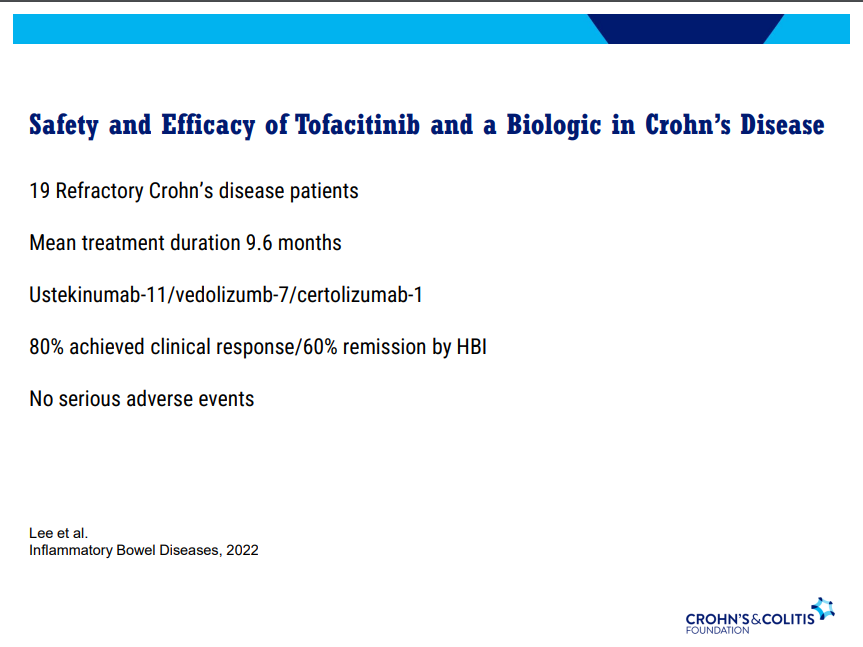
Discussed several combination treatments -no large studies thus far
I recently attended a regional CCFA conference. David Rubin gave several terrific lectures. Here are some of my notes and some slides from this lecture. My notes may contain transcription errors as well as important omissions. Can get access to full set of slides here: Biologics and Their Biosimilars
“Biologics and Their Biosimilars“
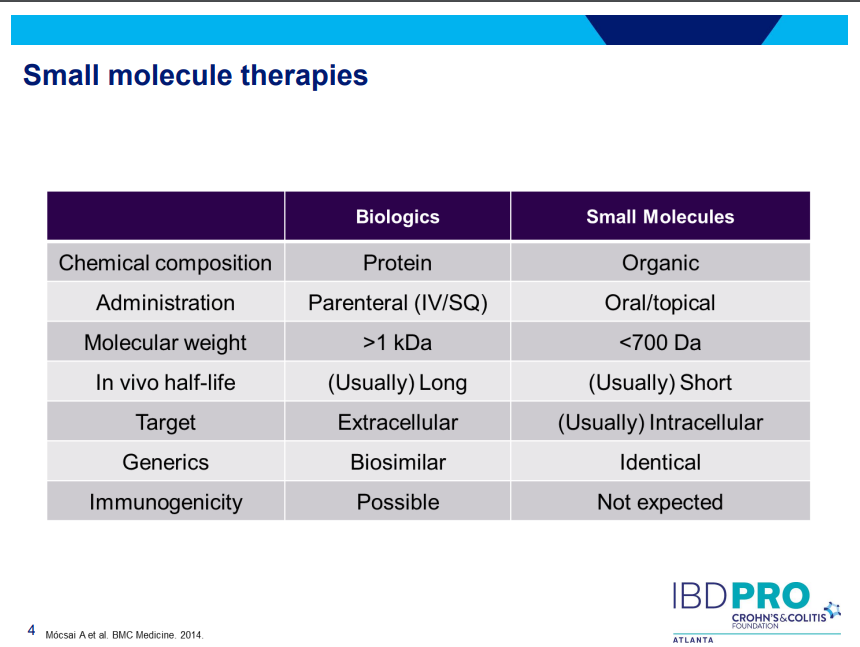
What is a Biologic Therapy?
Dr. Rubin makes a point of explaining the term to patients. It is a protein made in a living cell that targets another protein. Term “biologic” can sound scary to patients. Usually given IV because they cannot be absorbed through the small bowel.
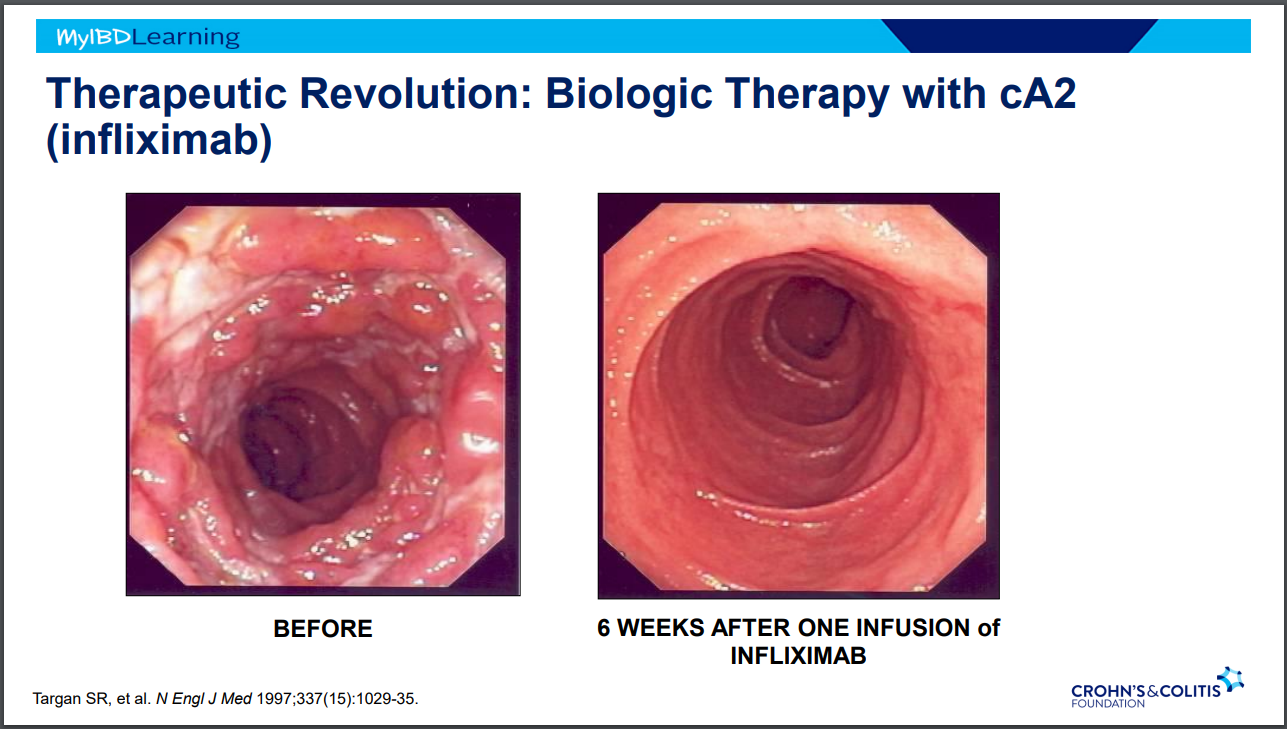
IBD Treatment Revolutions
Steroids -overnight changed mortality in IBD
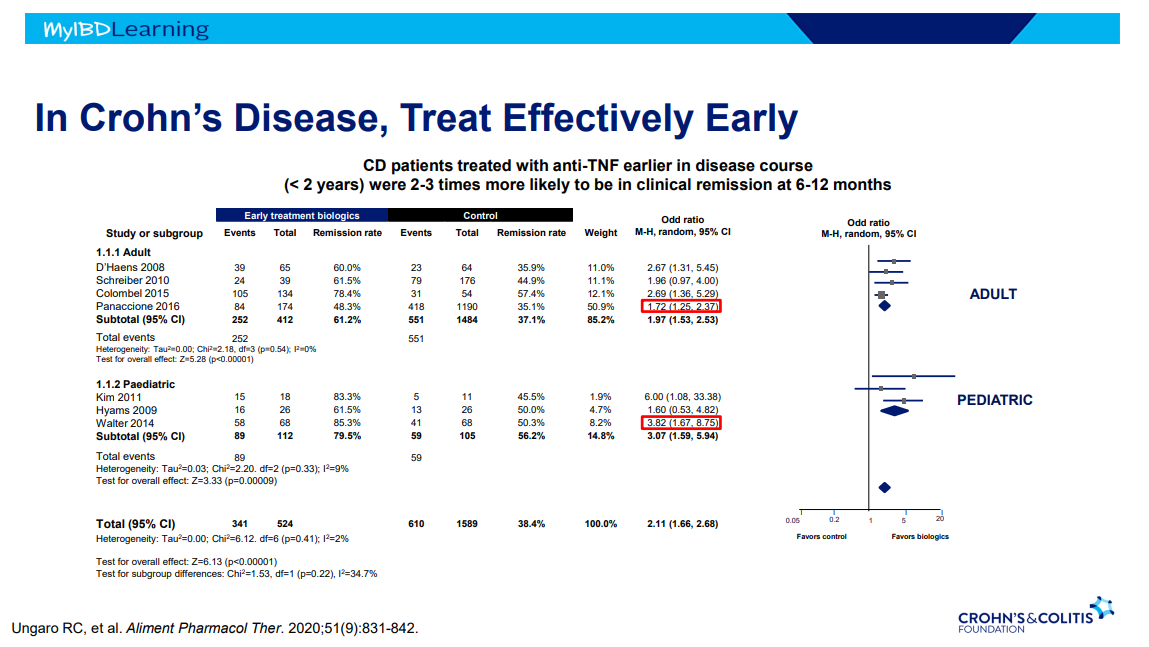
Anti-TNF Therapy in IBD -taught many lessons. Treat earlier –>better outcomes.
Anti-TNF Therapy
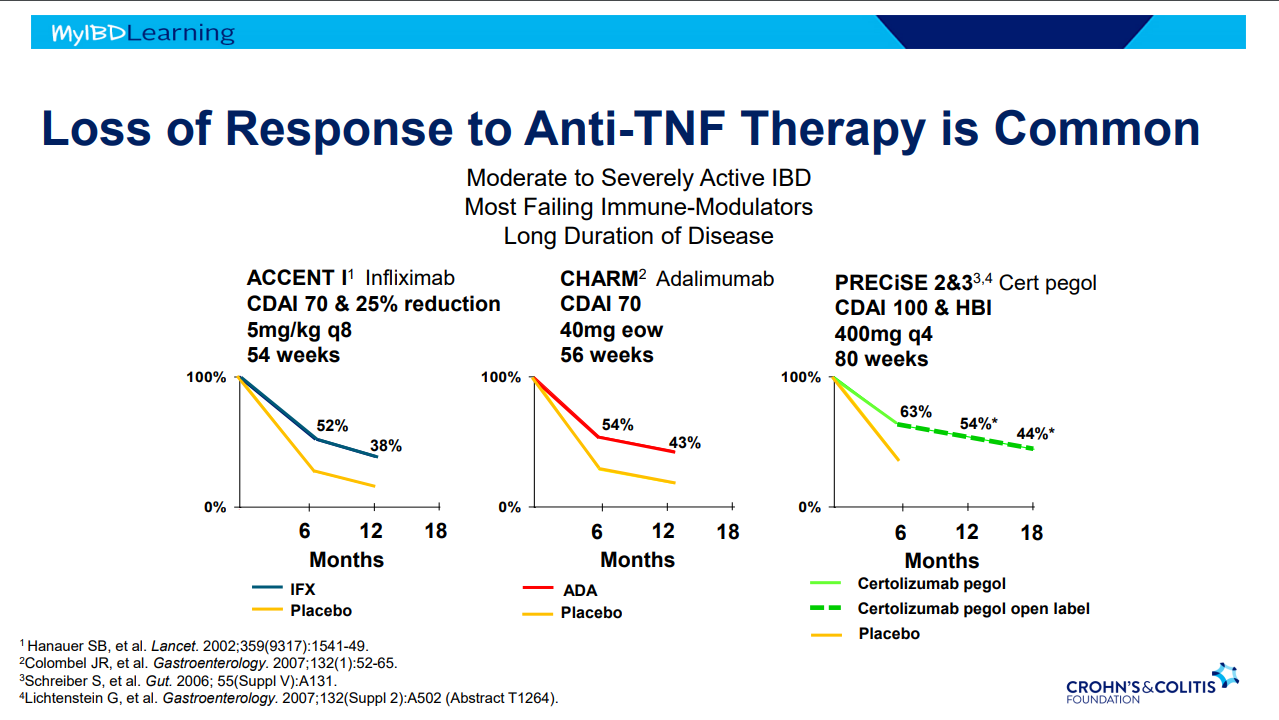
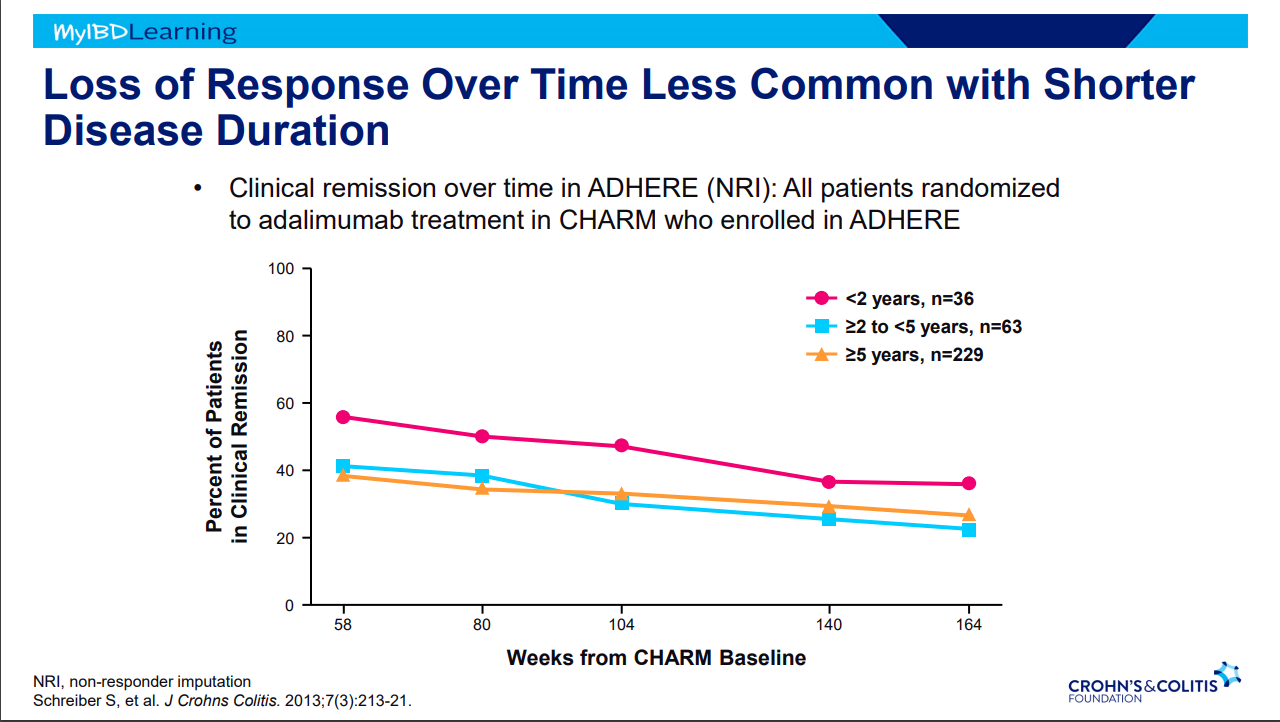
Frequent loss of response.
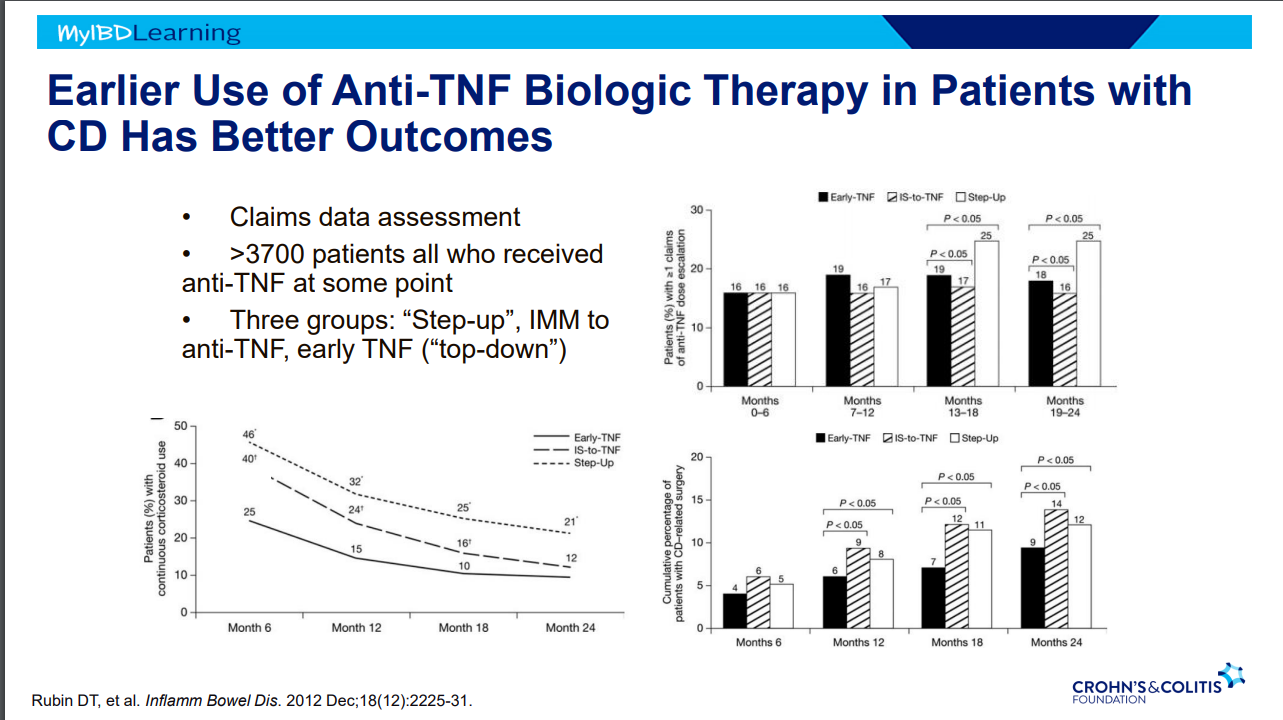
Earlier treatment with biologics result in better outcomes.
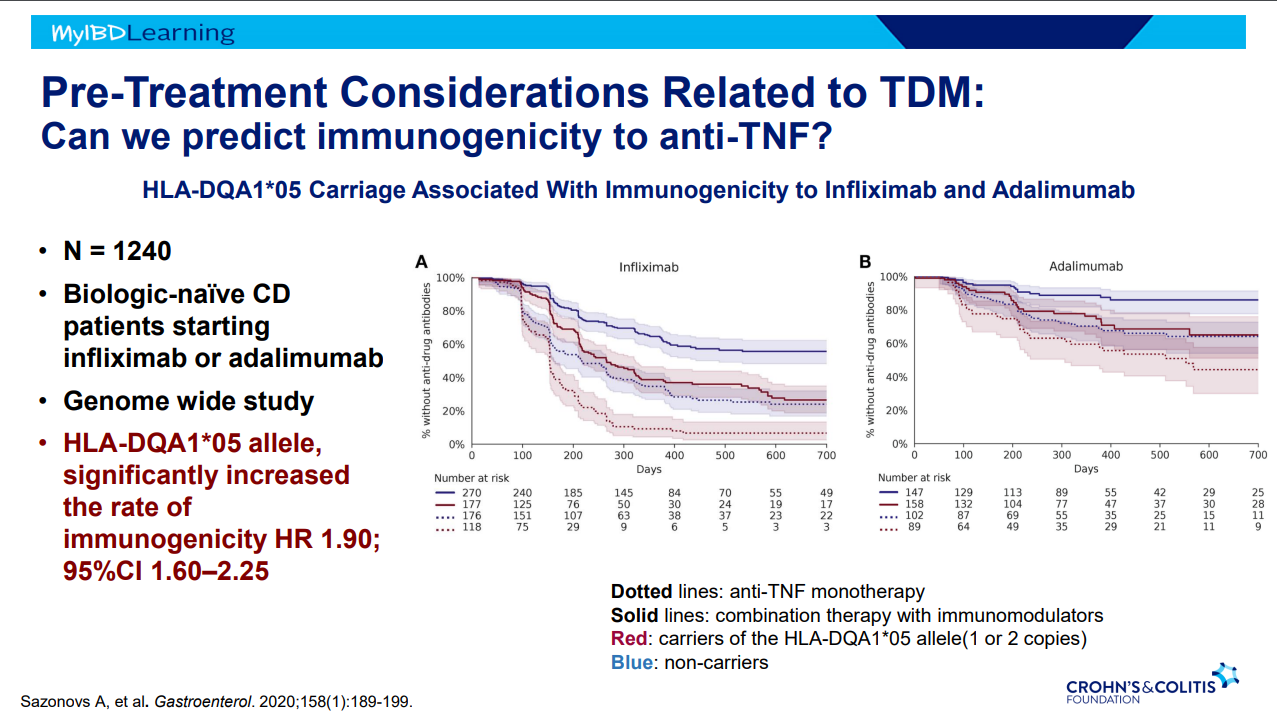
Immunogenicity is mainly an issue with anti-TNF agents and not much of an issue with other biologics. Episodic therapy is a big risk factor for anti-drug antibodies.
If staying with in-class medication, after anti-drug antibodies, need to take additional measures to prevent anti-drug antibodies (eg. Immunomodulators).
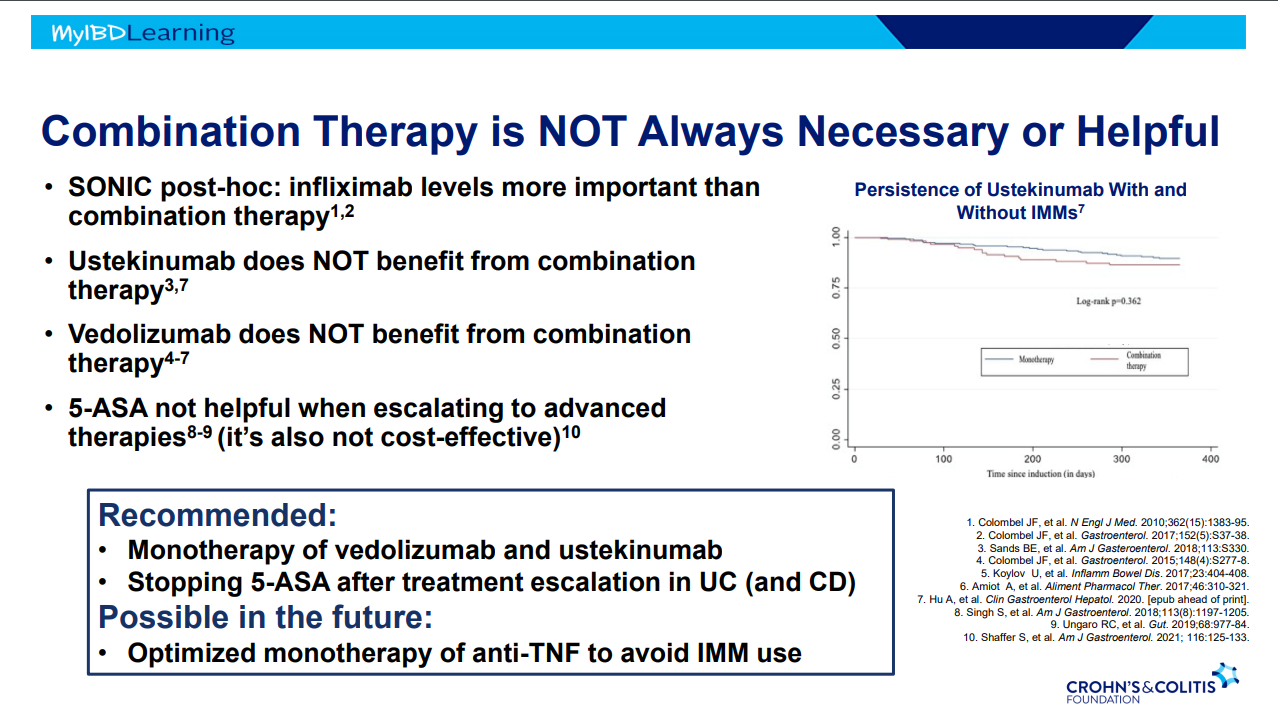
Combination therapy is more effective (SONIC, UC SUCCESS trials). This is due to using multiple mechanisms of disease control, reduction in anti-drug antibodies, and elevated serum drug levels.
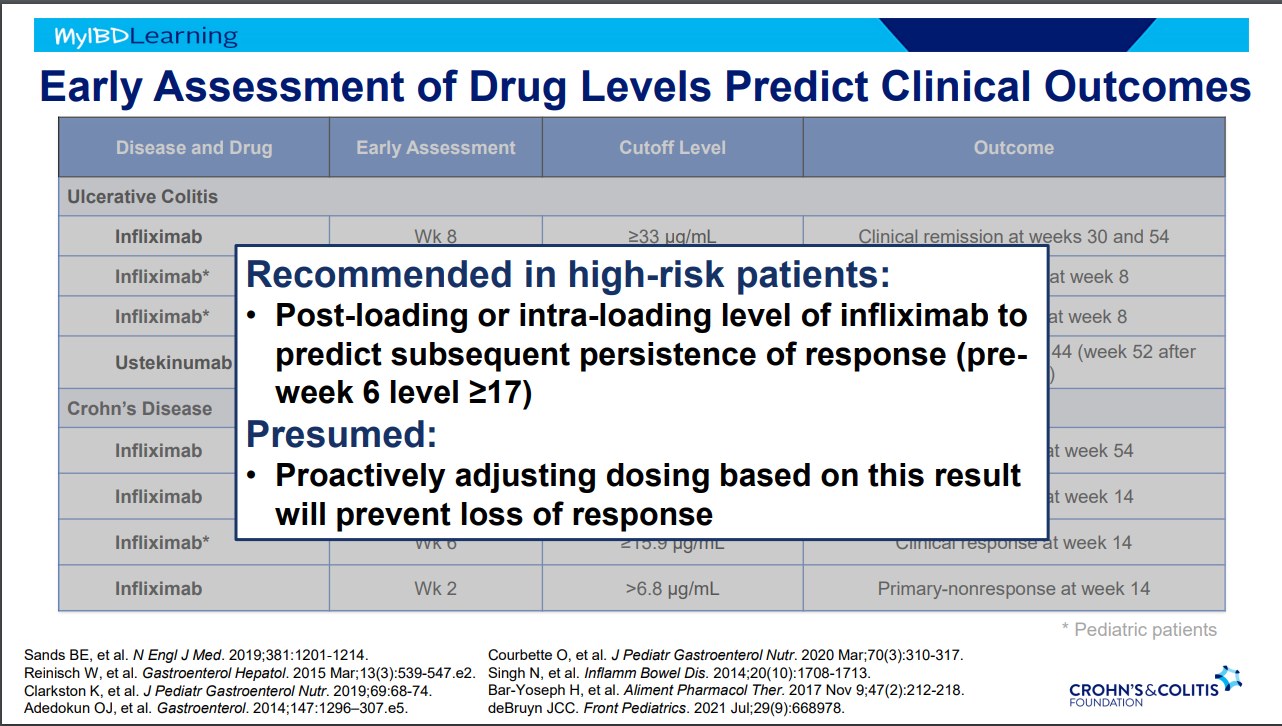
Good therapeutic levels appears to deliver similar results as combination therapy
Pre-week 6 level of 17 or greater, associated with good response in maintenance. If level is low, presumption is that higher dosing will be beneficial.
Higher levels of infliximab trough levels needed for perianal fistula healing (improved with ciprofloxacin). Higher levels could be causally-related to healing or could be a marker that there is less inflammation and a patient is responding.
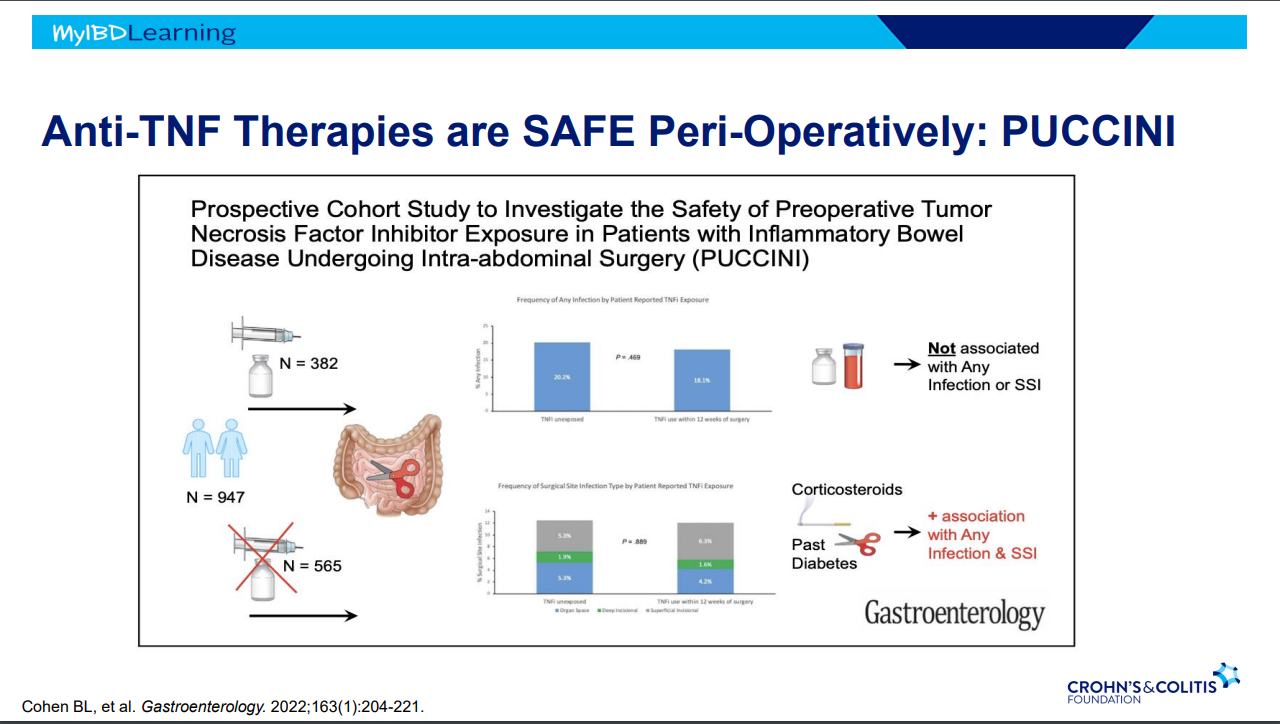
Anti-TNFs do not appear to increase risk of infections (see PUCCINI study)
Vedolizumab -terrific safety profile. No PML, no malignancy risk
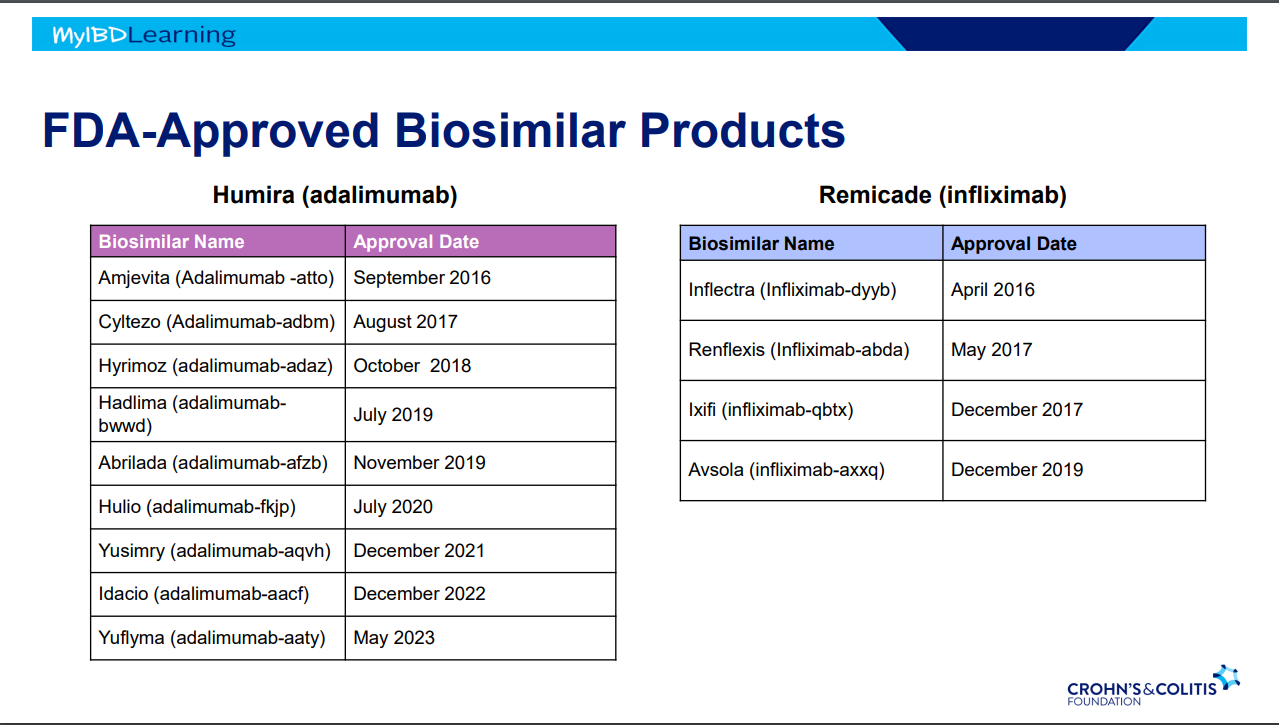
Biosimilars:
If biosimilar found effective for one approved condition, extrapolation given to all indications
IBD switching studies have NOT shown increased loss of response. Consider reassess prior to switch to help determine if patient truly in remission prior to switch. Switching often blamed for loss of response when many times the disease was not under good control prior to switch
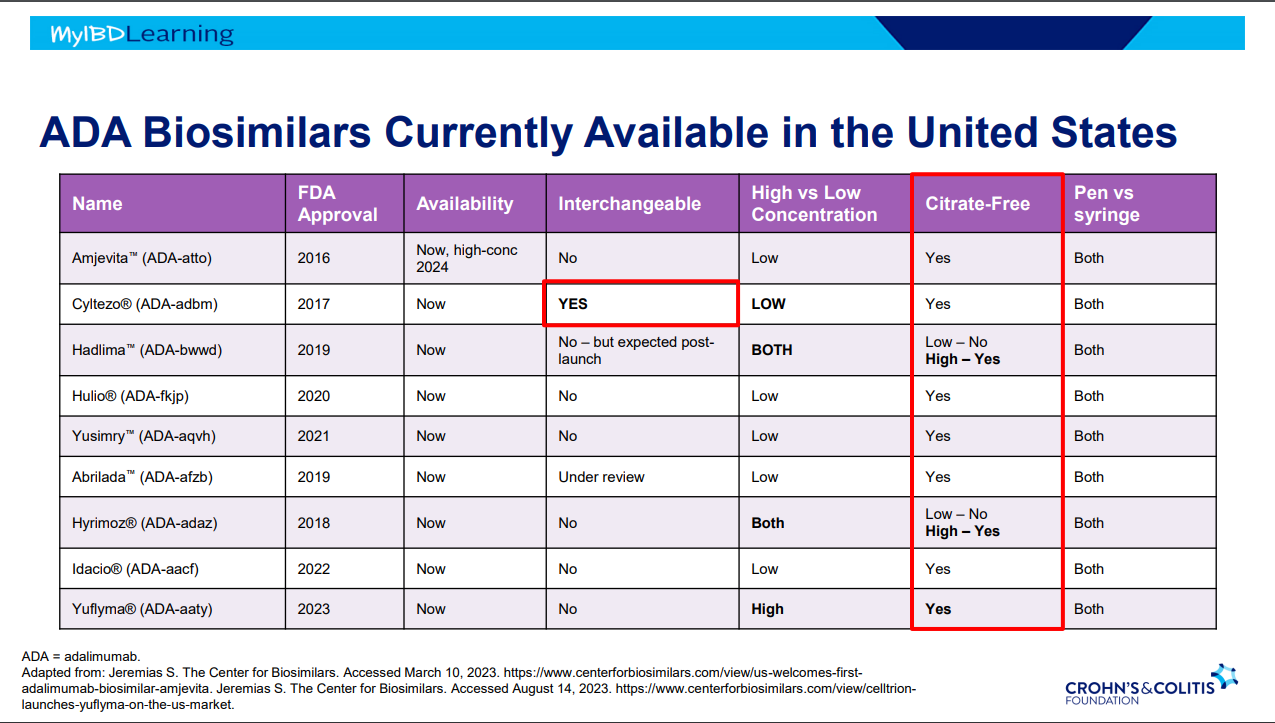
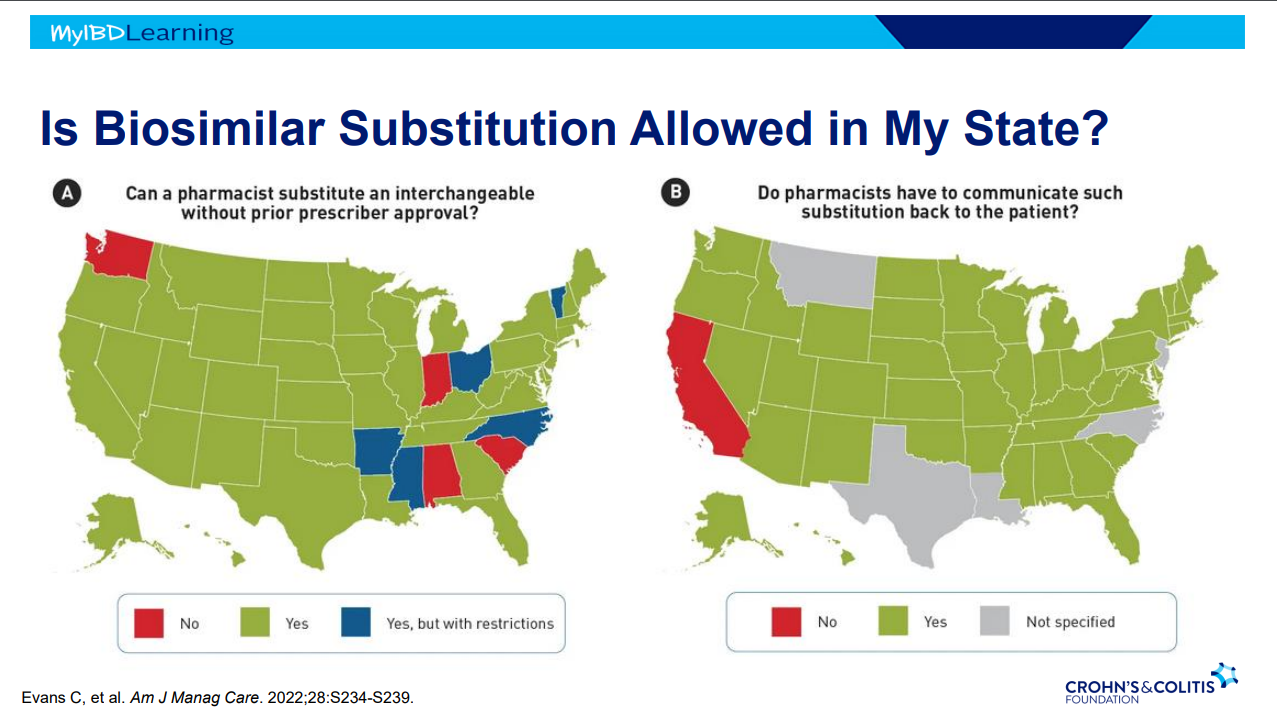
Interchangeable indicates that the drug can be switched by pharmacists
Biosimilars are saving insurers money but no proof that this is saving patients money
Anti-drug antibodies will cross-react to biosimilars
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
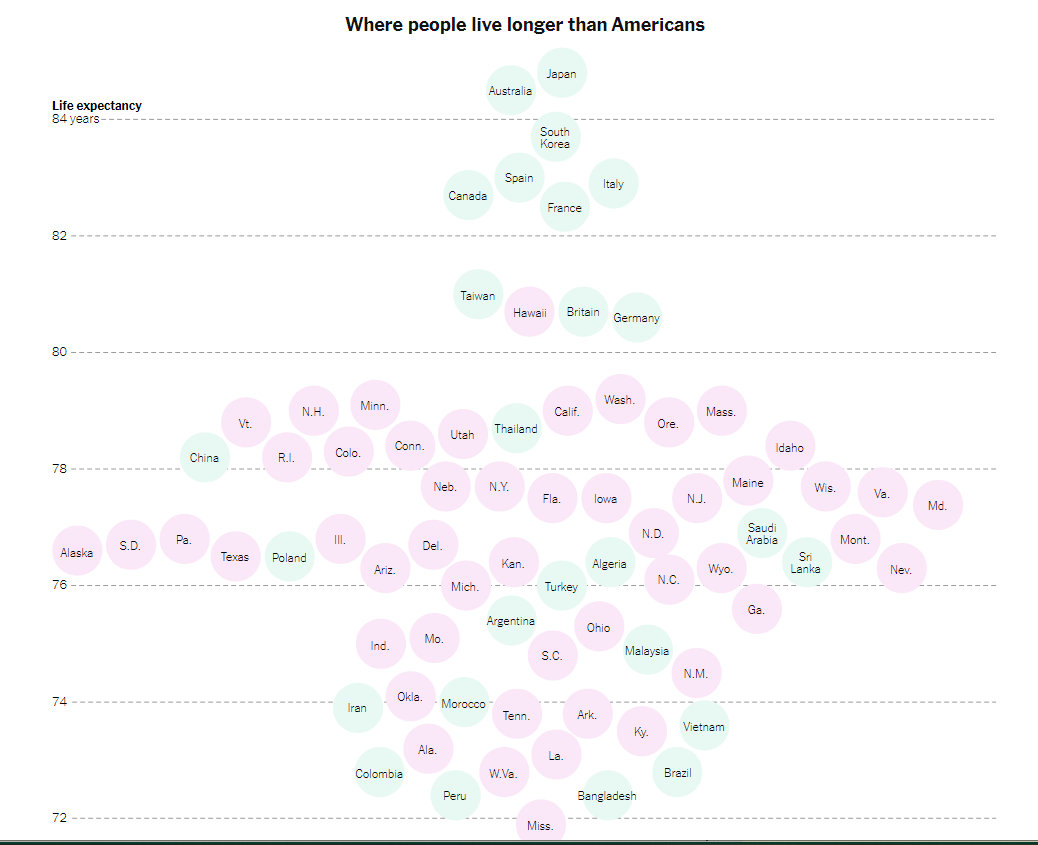
“It’s not just that life expectancy in Mississippi (71.9) now appears to be a hair shorter than in Bangladesh (72.4). Nor that an infant is some 70 percent more likely to die in the United States than in other wealthy countries….
All that is tragic and infuriating, but to me the most heart-rending symbol of America’s failure in health care is the avoidable amputations that result from poorly managed diabetes…A toe, foot or leg is cut off by a doctor about 150,000 times a year in America, making the United States a world leader of these amputations.
America’s dismal health care outcomes are a disgrace. They shame us. Partly because of diabetes and other preventable conditions, Americans suffer unnecessarily and often die young. It is unconscionable that newborns in India, Rwanda and Venezuela have a longer life expectancy than Native American newborns (65) in the United States. And Native American males have a life expectancy of just 61.5 years — shorter than the overall life expectancy in Haiti.“
The article recommends
Expanding Access to Health Care
Work on improving health behaviors: “smoking, eating habits and exercise — affect life expectancy even more than access to health care”…
Work on poverty and education: “America’s health dysfunction is rooted in a broader national dysfunction, including deep intergenerational poverty and despair. The medical system can efficiently amputate a foot, but an improvement in self-care of diabetes sometimes requires an injection of hope and improvements in education, job training, earnings and opportunity.”
This pediatric retrospective study (n=291, 2010-2020) showed a high response to infliximab in patients with inflammatory bowel disease (n=234 Crohn’s disease (CD), n=53 ulcerative colitis (UC)) over a 10-period. Mean duration of treatment among study participants was 2.9 years. Key findings:
53% (n=135) started with doses of 10 mg/kg and 64% (n=87) of those who started on 5 mg/kg were dose-escalated; thus, approximately 76% of patients in their cohort needed doses of 10 mg/kg.
Only 12% of patients discontinued treatment over the observed timeframe.
Patients with UC (P ≤ 0.01) and patients with extensive disease (P = 0.01) had lower durability, despite a higher starting dose of IFX (P = 0.03). Figure 2 indicated that durability in CD was ~93% compared to ~60% for UC with HR of 5.12. The HR for extensive disease (n=77) was 3.74 compared to those with limited disease (n=108). Still, ~75% of those with extensive disease continued on treatment
Common adverse events included 18 with skin findings (14 with psoriasis, 3 nonspecific rash, 1 with lupus), 23 with infusion reactions, 7 with AST/ALT >3 times ULN (or >120 IU/L), and 3 with serious infections.
Like the theme song from the 1996 Olympics (Reach, Gloria Estefan) reaching higher (dosing) resulted in being stronger (i.e.. better outcomes).
My take: This study showed really good outcomes associated with “accelerated” infliximab dosing.
The view before starting a climb at NRocks (Circleville, WV)Highest point of our climb
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
9/5/23 CNN: Delta flight forced to turn around because of diarrhea incident ““It’s just a biohazard issue, we had a passenger who had diarrhea all the way through the airplane so they want us to come back to Atlanta,” a DL 194 pilot said to air traffic control.”
When a family member saw this, he wondered if someone on the plane yelled: “Is There a Gastroenterologist on This Plane?”
My take: In this case, as with a lot of GI symptoms, having a good cleaning crew is usually more important than having a good physician. And, what a terrible situation!
The retrospective study by Zimmerman et al involved 170 pediatric patients (IFX (n = 84) and TAC (n = 86)) with acute severe colitis (ASC) form 2005 to 2017; TAC was generally used prior to 2014 and patients were more likely to be receiving 6MP as a long-term maintenance agent; the mean TAC level was 10.7 ng/mL. The mean dose of infliximab (IFX) initially was 7 mg/kg. Key findings:
The rate of colectomy 6 months from rescue therapy was similar whether patients received IFX or TAC (22.6% vs 26.7%, respectively, P = 0.53).
The mean decline in Pediatric Ulcerative Colitis Activity Index scores from admission to discharge in those treated with IFX (31.9) or TAC (29.8) was similar (P = 0.63).
Similar rates of adverse effects were seen. 4 patients in the TAC group experienced neurologic symptoms.
About half of the steroid-refractory ASC patients failing either agent as initial rescue therapy required colectomy, even if they switched to the alternative agent.
17.9% of patients receiving high-dose IFX required colectomy by 6 months compared to 25% in the “typical” IFX dosing group; this was not statistically significant, likely due to limitations of sample size.
In the systematic review/meta-analysis study by Bolia et al., the authors identified 7 studies with 166 children (111 steroid-refractory, 52 steroid-dependent, 3 no steroids). The majority of cases (150/166 [90%]) were naïve to biologics. None of the participants in these studies have been treated recently (only 10 patients since 2014 and none after 2016). The two most recently published studies in 2018 and 2019 had enrollment in 2014-2016 and 2000-2012, respectively. Key findings:
An initial response to tacrolimus therapy was seen in 84%
No difference was observed between children with high (>10 ng/mL) or low tacrolimus levels (127/150 [85%] vs 12/16 [75%], P = 0.3).
The pooled frequency of 1-year colectomy-free survival in children treated with initial oral tacrolimus was 64% (95% CI: 53%–75%). Twelve (7.2%) patients required cessation of therapy because of side effects.
My take: Both of these studies indicate that tacrolimus could be a useful agent for ASC and may find a role as a bridge therapy for biologic agents with slower onset of action.
Treatments for “Bad” Inflammatory Bowel Disease (Part 3) **An alternative agent to cyclosporine is tacrolimus. Hamel B, Wu M, Hamel EO, Bass DM, Park KT. Outcome of tacrolimus and vedolizumab after corticosteroid and anti-TNF failure in paediatric severe colitis. BMJ Open Gastroenterol. 2018;5(1):e000195
A couple good review articles (though behind paywall):
PT Reeves, L James-Davis, M Khan. Neoreviews 2023;24(7):e403-e413. Gastrointestinal Bleeding in the Neonate: Updates on Diagnostics, Therapeutics, and Management This reviews covers the most important etiologies of GI bleeding in the neonate. A few interesting points were the potential use of calprotectin as a potential screen for necrotizing enterocolitis; “the median fecal calprotectin levels in infants with NEC were between 210 and 400 mg/g of stool.” The authors also point out that there is “limited evidence for performing endoscopy in infants with GIB…][In one study] Only 3 of 56 infants underwent therepeutic intervention during endoscopy. Five percent (n=3) of these neonates exhibited gastrointestinal perforation in the acute postoperative period after endoscopy.”
The article notes that meconium is typically passed in 24 to 48 hours after gastrograffin enema and recommends abdominal imaging every 8 to 12 hours after enema administration to exclude perforation along with adequate intravenous hydration (“at least 150 mL/kg per day”).
The actual article has many other useful points. For example:
CFTR is not expressed in hepatocytes; “however, liver injury may occur patients with CF due to proximity to cholangiocytes (which may be inflamed) and/or through increased intestinal permeability.”
Elastase levels are not affected by exogenous pancreatic enzyme supplementation and is expected to display levels within the normal adult range by 2 weeks of age.
Sodium deficiency is common and needs to be prevented with sodium supplementation in first 12 months of life (one-eighth teaspoon (= 12.5 mEq) of salt in first 6 months, and one-fourth teaspoon (=25.2 mEq) from 6-12 months)
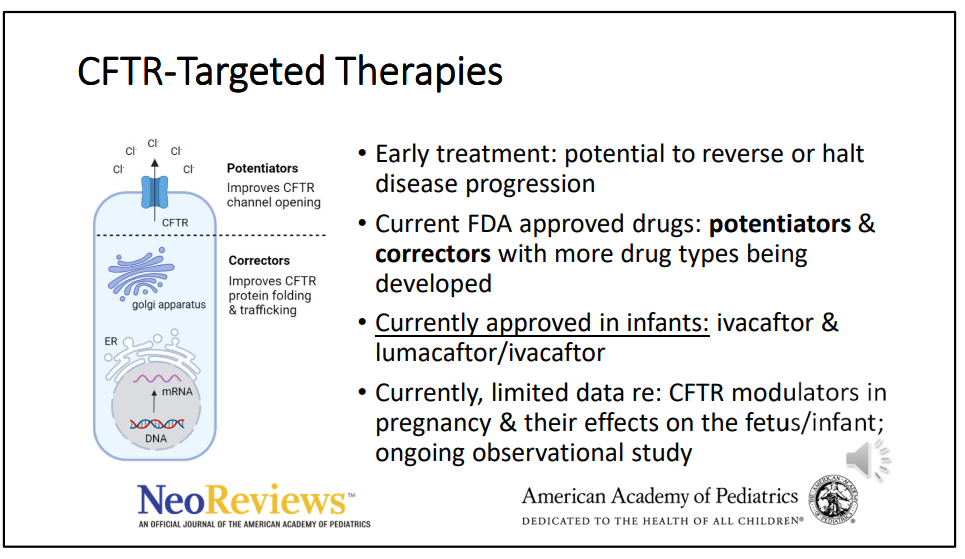
The newest CFTR modulator, elexacaftor/tezacaftor/ivacaftor is approved for children 2 years of age and older
There are case reports of in utero exposure to CFTR modulators associated with resolution/prevention of disease (eg. pregnant women starting CFTR-targeted treatment at 32 weeks gestation which resolved meconium ileus).
K McNelis, ME Rogers, S Kocoshis. Neoreviews. 2023 Jul 1;24(7):e431-e439. Pediatric Intestinal Transplantation Management and Outcomes This is another useful review for pediatricians. Pediatric intestinal transplantation is most commonly (65%) related to short bowel syndrome, 20% due to motility disorders, 9% due to mucosal diseases, 5% due to retransplantation and 1% are due to a variety of causes. The evaluation and management of patients needing intestinal transplantation is succinctly summarized. “Overall, survival of pediatric patients after intestinal transplantation is 72.7% at 1 year and 57.2% at 5 years. The most common causes of death are sepsis/multiorgan system failure and cardiovascular/stroke (Fig 2).” Also, “current statistics about organ transplantation can be publicly accessed by health care team members, patients, and families at srtr.transplant. hrsa.gov.” This site also includes data on transplantation for kidney, pancreas, heart, lung and liver.
After a literature review, the authors included 10 studies reporting semen parameters (268 patients with IBD) and 16 studies reporting adverse pregnancy outcomes (over 25,000 patients with IBD). Key findings:
Biologic, thiopurine, or methotrexate use were not associated with decreased sperm count, motility, or abnormal morphology compared with nonexposed patients.
Biologic, thiopurine, or methotrexate use among male patients with IBD are not associated with increased odds of adverse pregnancy outcomes