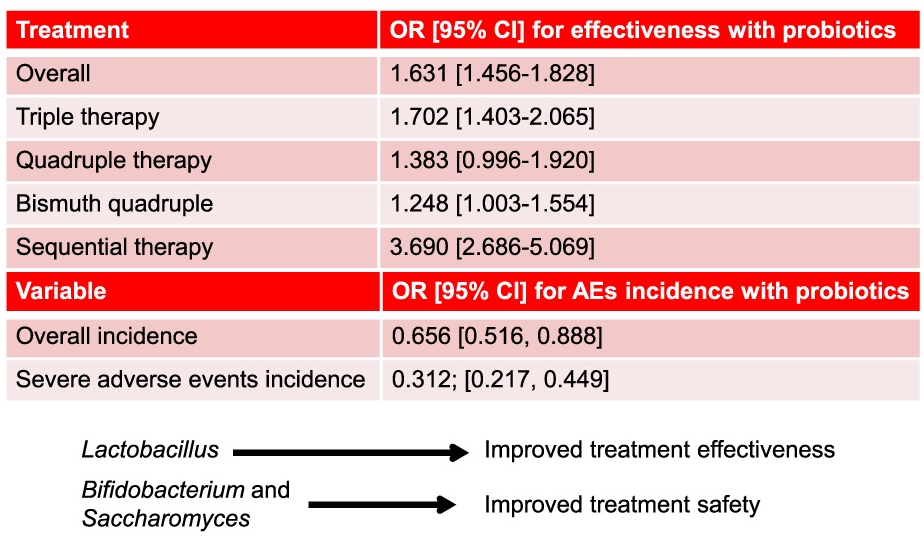
Methods: Prospective European registry with 36,699 treatments were recorded, where 8,233 (22%) were prescribed with probiotics. The analysis of the effectiveness of probiotics was restricted to those receiving first-line therapy.
Key findings:
Overall, the eradication rate was 90.6% with probiotics and 86.1% without probiotics.
With quadruple therapy, the eradication rate was 93.1% with probiotics and 89.3% without probiotics
Discussion Points:
“The prevalence of H pylori infection remains close to 45% in the European population”
The population receiving probiotics may have been expected to have a higher risk of eradication failure (eg. antibiotic resistance and more prior treatments) and/or higher expectations of adverse effects
This was NOT a randomized study which limits a more definitive conclusion on the effectiveness of adding a probiotic
My take: In highly-motivated families, probiotics may be worthwhile as part of an H pylori eradication regimen. This could, of course, necessitate changes in nomenclature. Would quadruple therapy with probiotics be called 5-drug (quintuple) treatment?
This article summarizes the recent changes in the treatment options for Clostridioides difficile (C diff).
Key points:
Fidaxomicin targets C diff with limited collateral microbiome disruption. This leads to significantly lower recurrence rates compared to vancomycin. Thus, it is preferred 1st line therapy for initial and recurrent C diff. In “the coming years, fidaxomicin is expected to come off patents” which will improve access and affordability.
Bexlotoxumab which lowered recurrence rate is no longer being produced
FMT via Openbiome is no longer available. In those in which FMT was used, options include the following:
live-jslm (REBYOTA), a broad consortium enema-based formulation
live-brpk (VOWST), a narrow consortium of Firmicutes in an encapsulated form. This treatment in adults: four capsules daily for three days
Both treatments are not recommended for patients who are severely immunocompromised. In these patients, prolonged vancomycin course with taper or using every other day therapy with fidaxomicin for days 7-25 could be considered
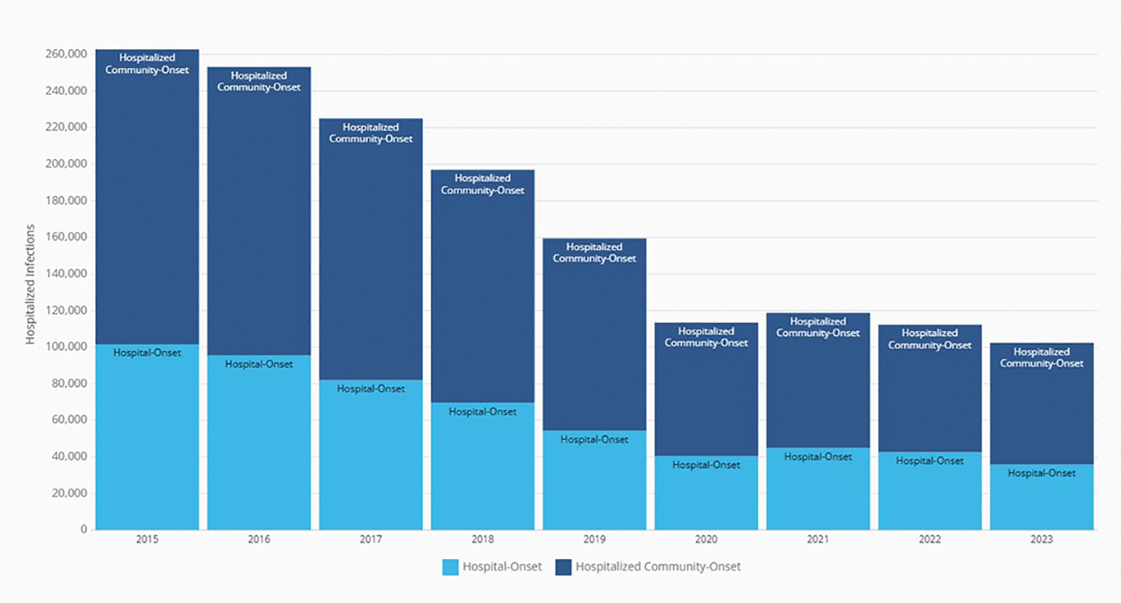
My take: I have been seeing less C diff cases recently. This may be due to better antibiotic stewardship, changes in C diff strains, or improved testing approaches.. My observation is supported by recent reports:
Annual number of hospitalized community-onset and hospital-onset CDI events reported to the National Healthcare Safety Network, 2015 to 2023. (From CDC’s Antibiotic Resistance & Patient Safety Portal (Available at https://arpsp.cdc.gov/profile/nhsn/cdi).)
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
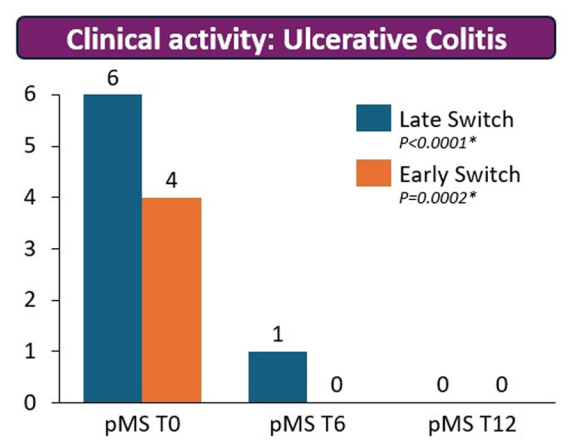
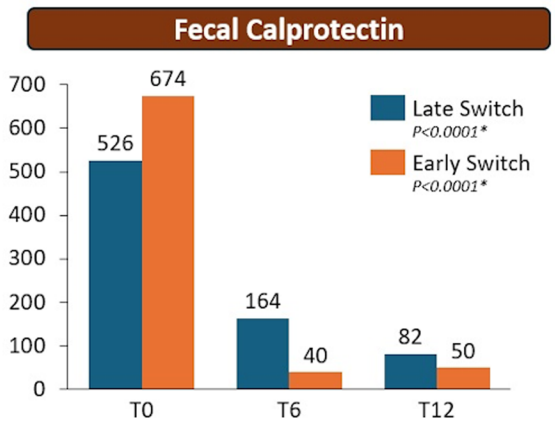
Methods: The RE-WATCH study was an observational, multicenter, retrospective study performed in four IBD referral centers. Inclusion criteria meant that only patients receiving on label SC-IFX at a dosage of 120 mg every other week were included in the study. The initiation of IFX therapy as the baseline timepoint.
Key findings:
There were no statistical differences between the two groups, early vs. late switch, after one year in terms of the respective endoscopic response (71.4% vs 70.8%, P = .95), steroid-free clinical remission (62.5% vs 68.7%, P = .51), or IFX retention rate (75.0% vs 66.7%, P = .35).
There was higher endoscopic remission rates in early switch patients as compared to late switch patients; however, this trend was not significant (69.6% vs 52.1%, P = .07).
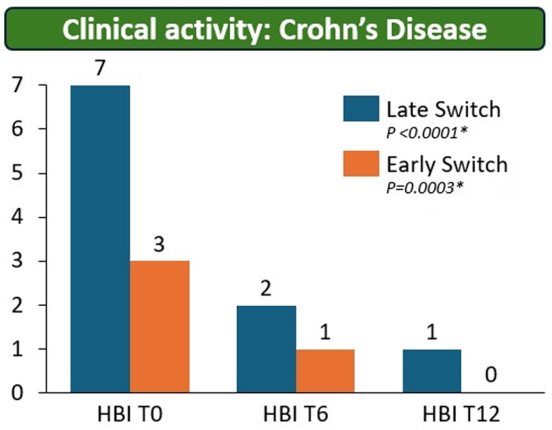
A return to IV-IFX was required in 1 of 43 early switch patients and in 3 of 44 late switch patients (2.3% vs 6.8%, P = .31)
While the early switch group appears to fare a little better, there is likely a selection bias. For example, the early group had a much lower rate of severe endoscopic score at baseline (20% vs. 54%) and lower rate of Crohn’s fistulizing disease (8% vs 33%).
partial Mayo score (pMS)Harvey–Bradshaw index (HBI)
My take: These results indicate that outcomes are similar between patients switching from to IFX SC at both early (after induction) and late (after 6 months).
It is worth noting that prior studies have shown that home-based therapies (eg. home infusion), compared to office-based therapies, have been “associated with suboptimal outcomes including higher rates of nonadherence and discontinuation of infliximab.” This is a concern for SC biologics as well.
Last week, the following article explained why the newest changes, announced yesterday (see link below), to the vaccine schedule recommendations are not a good idea:
“Proponents of the push to align U.S. recommendations with those of so-called peer nations such as Denmark, Japan and Germany — all of which recommend fewer shots than the United States — have billed it as a common-sense corrective. But, as innumerable doctorsandscientists have explained, when it comes to public health, countries with fewer shots on their must-have list are not actually our peers.
In Denmark, to take the administration’s favorite example, prenatal care is free and universal. More than 95 percent of pregnant women are screened for hepatitis B, and those who test positive are promptly treated and duly monitored…
None of this is true in the United States.
Here, nearly a quarter of pregnant women lack adequate prenatal care, and those who face the highest risk of contracting and spreading vaccine-preventable diseases are often the least likely to have access to doctors or pharmacies. When U.S. health officials tried to stamp out hepatitis B through vaccination programs aimed at high-risk groups, they failed miserably. It was not until they carried out a universal, at-birth vaccination policy in 1991 that hepatitis B infections finally plummeted — by about 99 percent.
In fact, if the U.S. public health system has one thing going for it relative to other nations, it’s probably vaccines. As the C.D.C.’s own data indicates, routine childhood vaccination has prevented hundreds of millions of illnesses and tens of millions of hospitalizations here. It has also saved half a trillion dollars in medical costs, a figure that jumps into the multitrillions once you factor in indirect, societal costs like lost productivity and lost wages.
The United States tends to have higher rates of measles vaccination than Europe, and fewer measles cases as a result. Compared with Denmark, we also tend to have lower hospitalization rates for rotavirus (which causes diarrhea and can be fatal in infants and children) and respiratory syncytial virus, or R.S.V. (which is a leading cause of hospitalization among children). The reason for those disparities is not in dispute: We vaccinate routinely against both viruses. Denmark does not…
In the meantime, the Food and Drug Administration is angling to make an even bigger and more enduring impact on Americans’ access to vaccines…top officials at the agency have proposed a roster of new requirements for the shots, including several that critics say would be logistically impossible and could leave us with no F.D.A.-approved Covid or flu vaccines…
We don’t have to wonder what that future will look like. We can glimpse it already in communities across the country where measles and whooping cough are resurgent and where infants and young children have already died from both. We can also see it foretold in the current flu season: This year’s flu vaccine has proved an imperfect match to the currently circulating strains. New shots, based on mRNA technology, would have one day enabled us to avoid this kind of misfire. But the nation’s leaders have imperiled that future with the decisions they made this year…
Mr. Kennedy has brought us to this precipice by aggressively subverting nearly every process and protocol that previously governed our public health institutions. He has granted political appointees enormous sway over agency scientists. He has excluded people with meaningful expertise from his planning and deliberations. And he has fired dissenters all the way up to the C.D.C. director and replaced them with lackeys, sycophants and wellness grifters.”
My take: RFK Jr and this administration has already done great damage to our health care and the toll will be evident for a long time. But, they are not done yet.
Link to yesterday’s announcement: NY Times 1/05/25: Kennedy Scales Back the Number of Vaccines Recommended for Children“Public health experts expressed outrage at the sweeping revisions, saying federal officials did not present evidence to support the changes or incorporate input from vaccine experts…and will endanger the health of children in the United States…The C.D.C.’s new schedule continues to recommend vaccines against some diseases, including measles, polio and whooping cough, for all children. Immunization against six other illnesses — hepatitis A, hepatitis B, meningococcal disease, rotavirus, influenza and respiratory syncytial virus, the leading cause of hospitalization in American infants — will be recommended for only some high-risk groups or after consultation with a health care provider.”
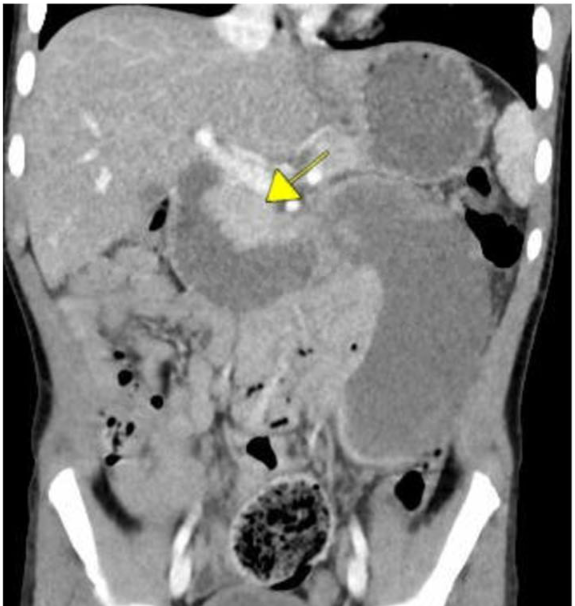
This 5-year single-center study from 2018 to 2022 identified a total of 13 patients with duodenal hematoma (DH). There were a total of 21,569 EGDs, and 16,978 EGDs with duodenal biopsies were performed during the study period.
Key findings:
1 DH in 1306 (0.08%) EGDs with duodenal biopsies. Ten of the thirteen patients had normal duodenal histology, and the other three each had findings of celiac disease, peptic duodenitis, and graft-versus host disease
None of the patients had a history of anticoagulant or antiplatelet agent therapy
Symptom onset occurred within 24 h for 8/13 (62%),48 h for 11/13 (85%), and 72 h for all 13 patients after EGD. Emesis occurred in all 13 patients and abdominal pain 7/13 (58%)
All patients were admitted with a mean length of stay of 18 days
Treatment: jejunal feedings in 4 of the 13 patients (31%), and parenteral nutrition in 10 of 13 (77%) patients. Most patients (62%) utilized opioids for pain management following DH
A similar study was conducted at the same center in 2015. It was noted that there was a lower rate of duodenal biopsies in the current cohort: 78.7% versus 92.4%
Computed tomography coronal image with hematoma
My take: Duodenal hematoma is a major complication leading to the need for parenteral nutrition and prolonged hospitalization. BMT and organ transplantation appear to increase this risk based on prior studies.
Using electronic medical record data, the study’s authors reviewed more than 5 million births at over 40 hospitals across all 50 states between 2017 and 2024. The number of infants who did not receive the shot at birth rose from 2.92% in 2017 to 5.18% in 2024, according to the report…
Since 1961, the AAP has recommended that a single shot of vitamin K be given at birth to protect against bleeding. All babies are born deficient in vitamin K.”
My take: Avoidance of Vitamin K in the newborn period indicates a mistrust of the medical system as well as desire for a more “natural” birth experience. However, this increases the chance than an infant will have permanent severe brain damage. When parents refuse Vitamin K, they are playing Russian roulette with their newborn’s life.
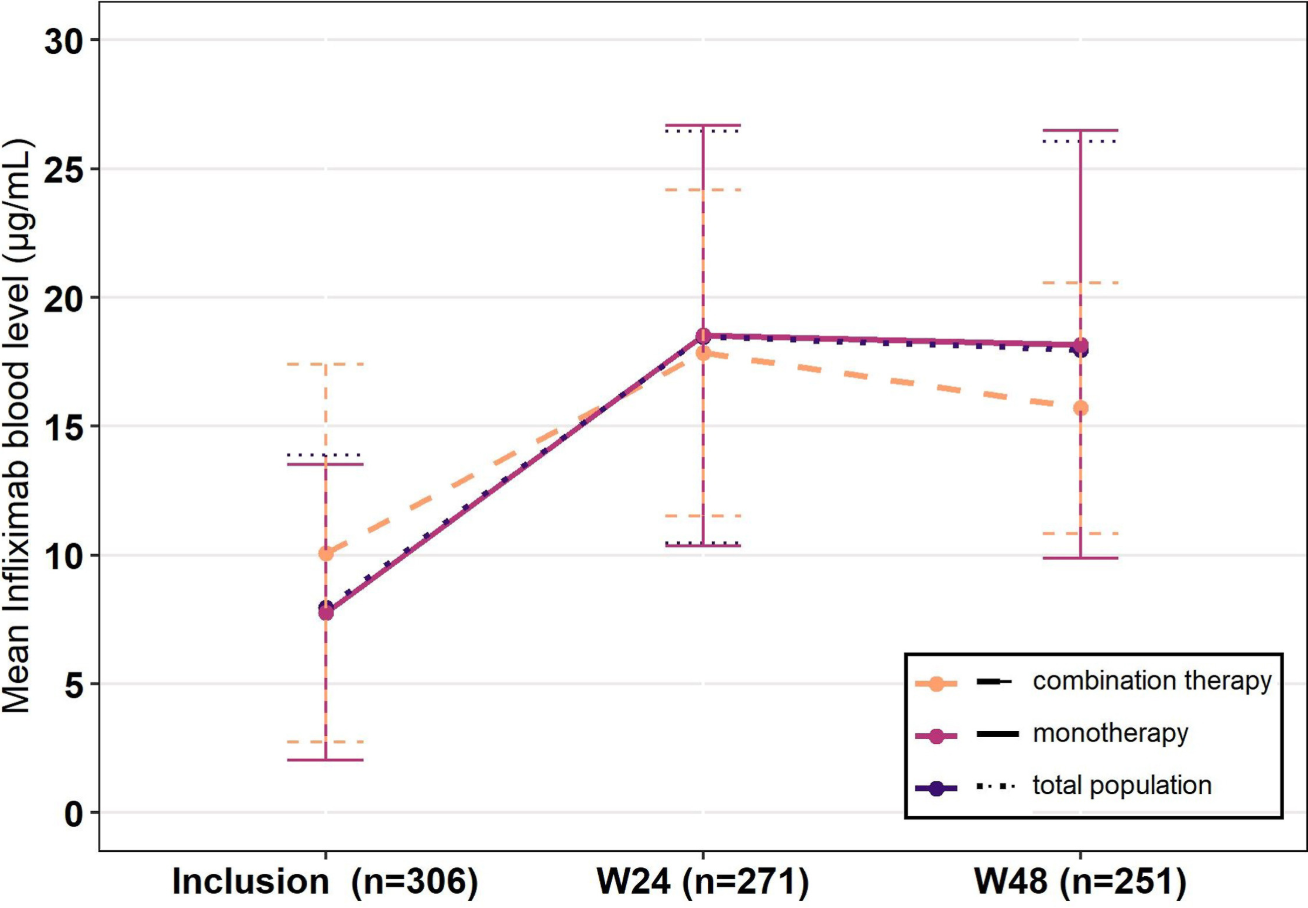
Methods: The PEREM (PErsistence, effectiveness and safety of subcutaneous infliximab after switch from intravenous infliximab in IBD patients in REMission) study, a prospective national French cohort trial, enrolled 426 patients with IBD. Participants were in steroid-free clinical remission for at least 6 months on IV-IFX when they switched to SC-IFX. 56% were on IV-IFX standard dosing (5 mg/kg 8-weekly) and 16% received combination therapy with an immunomodulator drug at baseline. All patients were switched to SC-IFX standard dosing (ie, 120 mg every other week). The treatment could be intensified during follow-up, either to 120 mg every week or 240 mg every other week.
Key Findings:
At week 48, SC-IFX persistence was 95.4%
86.9% of patients were in steroid-free clinical remission
Mean infliximab levels were 8.0 μg/mL at inclusion and 18.0 μg/mL at week 48 (P < .0001)
Among the 19 (4.5%) patients who stopped SC-IFX, 6 (1.4%) switched back to IV-IFX
Dosing at 10 mg/kg/Q4W had 100% SC IFX persistence compared to 95% for 5 mg/kg/Q8W; however, at the 48 week followup, there were only 6 patients in the higher dose compared to 149 in the lower dose
Ongoing use of combination therapy was not associated with better persistence. Though, only 7 patients were receiving combination therapy at the 48 week followup
From the discussion:
“The high persistence observed in the PEREM study is partly explained by the long-term control of the disease by the time of switch, the median time since last flare being over 5 years before inclusion. Henceforth, the persistence observed here is in accordance with results on long term maintenance of IV-IFX, the yearly persistence of IV-IFX without intervention being 87%.”
SC-IFX was associated with higher levels. However, this was expected and higher levels are needed with SC administration. The “different bioavailability of SC-IFX compared with IV-IFX is responsible for different goals of infliximab blood levels depending on its route. In particular, a level above 20 μg/mL has been associated with higher rates of remission20” with SC-IFX.
My take: This study shows that SC-IFX is a good option for patients in long-term remission. With SC-IFX therapy, more effort is needed to make sure patients are adherent with therapy and monitoring in order to achieve optimal outcomes.
Eric Topol has summarized more recent advances that indicate that future treatments could be safer and less costly. Instead of manipulating T-cells outside the body, an inside the body (in vivo) approach looks promising. Substack post, 12/14/25: The Exhilarating Movement From Treatment to Cures for Autoimmune Diseases
An excerpt:
“This inside the body, off-the-shelf strategy has already been shown to be safe and successful in Phase 1 trials of refractory SLE and in patients with systemic sclerosis or severe myositis…Several companies are in clinical trials with in vivo CAR T for autoimmune diseases including Capstan Therapeutics, Kite Therapeutics, Umoja Biopharma, and Shenzhen Magic-RNA. The striking progress in this field towards universal, potential one-shot cures is tempered by residual anticipated high cost, the cytokine release syndrome and neurotoxicity that can occur with CAR T. The mRNA and non-viral vectors are considered a better choice than a lentivirus vector because of the latter’s potential risk of mutagenesis and cancer…
The Soft Reset: Inverse Vaccines to Achieve Tolerance…
Tolerogenic vaccines [are] the opposite of standard vaccines that boost the immune system…Inverse vaccines are being pursued in celiac disease (Anokion, with positive clinical trial results reported earlier this year) , multiple sclerosis (ANokion, Moderna, BioNTech), and Type 1 diabetes (Diamyd Medical), rheumatoid arthritis (Janssen clinical trials.
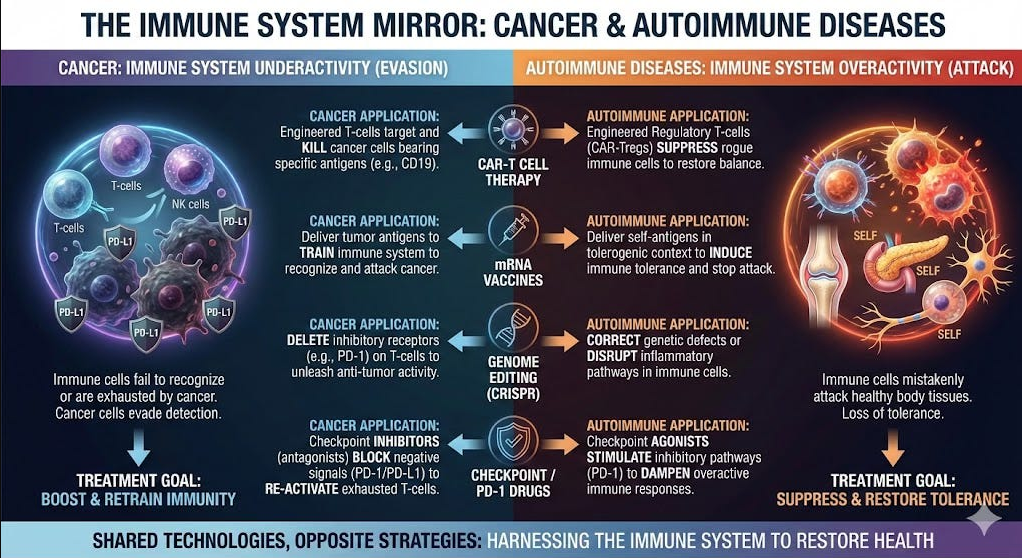
How Progress in Cancer Fuels Autoimmune Disease Innovation
Cancer biology is the mirror image of autoimmunity. Predisposition to cancer occurs when the immune system is hypoactive, losing its protection, whereas autoimmune disease reflects hyperactivity and a dysregulated state…The B cells are a common culprit, hence the successful use of CAR T vs B cells for both diseases. The checkpoint inhibitor PD-1 (prototype Keytruda) is to cancer (cut the brakes on the immune system) as PD-1 agonists (slam on the brakes) are to autoimmune diseases. Similarly, cancer vaccines to rev up immunotherapy are the opposite of inverse, tolerogenic vaccines…
[There is a] reciprocal relationship between CAR T for cancer and autoimmunity. What’s important to emphasize is all the work to achieve in vivo, universal CAR T works for both diseases. Anything that helps cancer immunotherapy has the big dividend of also helping the efforts for curing autoimmune diseases. The new field of structural immunotherapeutics has legs to achieve precise control of our immune system vs either sets of diseases…
We’e seeing the initial stages of a renaissance vs autoimmunity. Curinginstead of just treating autoimmune diseases.”
Background: “Recent studies demonstrate only 11% of youth between 9 and 21 years of age in the United States (US) had documented lipid screening, and 30%-60% of youth with dyslipidemia may be missed by targeted screening alone (ie, risk factors) compared with ULS [universal lipid screening]. Identification of youth living with familial hypercholesterolemia (FH) has the added benefit of triggering reverse cascade screening of family members, which can further identify at risk youth and adults.”
“In 2024, the Family Heart Foundation (FHF) established the Leveraging Evidence and Data (LEAD) for Pediatric Cholesterol Screening Initiative…The focus was not on creating new screening guidelines, but on developing strategies that will lead to better implementation of the current NHLBI/AAP screening recommendations, and with the overall goal of reducing global ASCVD [atherosclerotic cardiovascular disease] burden.”
“In FH,untreated elevated levels of LDL-C in childhood significantly increase the risk for premature atherosclerotic cardiovascular disease (ASCVD), which is the leading cause of death both in the US and worldwide. However, early initiation of statin therapy for children living with FH reduces the ASCVD risk in adulthood.”
Key points:
“Three common barriers to pediatric ULS were identified.
First, many parents and caregivers are not aware of the current pediatric lipid screening guidelines.
Second, the major rationale for ULS in young children and adolescents—early identification of a treatable genetic condition—may not be clear to patients, families, and/or clinicians.
Third, the values and concerns of families may be dismissed by clinicians if there is a misunderstanding of the rationale for ULS
Practical ways to improve ULS:
Improve education of parents and clinicians that ULS can reduce the risk of premature death from the leading cause
Point-of-care testing
EHR prompts
Develop physician “FH champions”
The article notes that a survey in 2017 showed that many PCPs were unaware of the national guidelines. In addition, “few were comfortable prescribing a lipid-lowering therapy.”
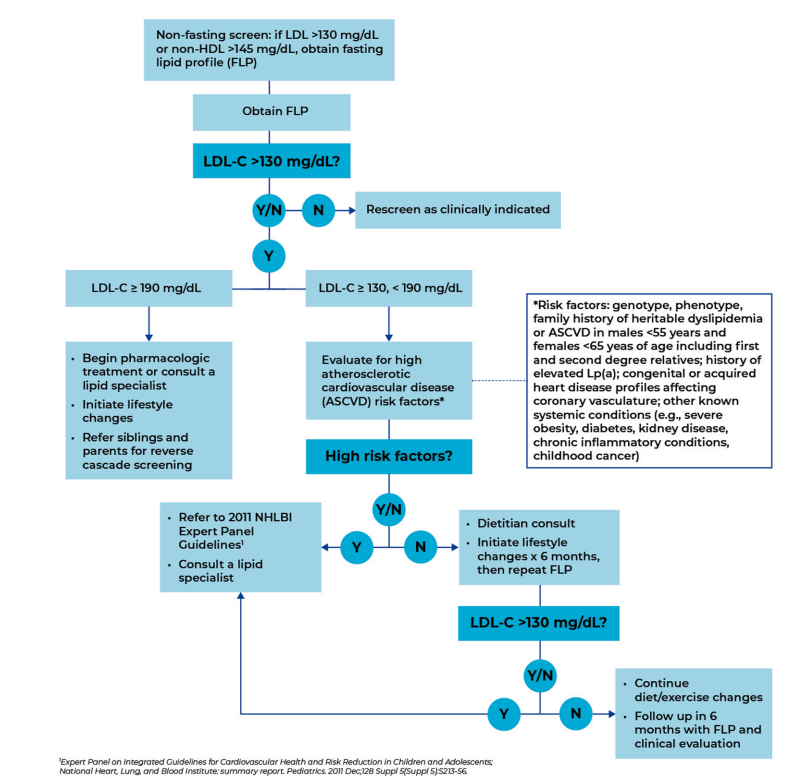
Recommended PCP Screening Algorithm:
My take: It is unfortunate that this article, which has an aim to improve awareness for universal pediatric lipid screening (ULS), is not an open access article. Incentives to implement lipid screening could help — screening rates are quite low despite guidelines that were published 14 yrs ago.
Related blog posts:
The Case for Universal Cholesterol Screening During Childhood (2024) — An excellent summary of the need/rationale for ULS. Heterozygous FH (HeFH) is the second most common potentially fatal genetic disorder in humans, affecting 1 in 250-300 people.8…Homozygous FH (HoFH) [is] much rarer, occurring in 1:250 000-1:360 000 people.. Proof that screening can make a difference:
Treatment Outcomes in Children and Adolescents with Hypercholesterolemia In a 20-year follow-up study, Luirink et al studied a cohort of individuals with genetically confirmed HeFH who had initiated statin therapy in childhood. When compared with their HeFH parents who had not had the benefit of childhood therapy, statins virtually eliminated excess ASCVD risk in adulthood. At age 40, 26% of parents had experienced a cardiac event and 7% had died of ASCVD, whereas only 1% of the those treated as children had needed a vascular procedure (coronary artery stenting) and none had died.
With regard to incentives, a recent commentary (DM Cutler, RS Huckman. NEJM 2025; 2025;393:2177-2180. Has Corporatization Met Its Match? The Challenge of Making Money by Keeping People Healthy) notes that the U.S. health system has financial incentives that rewards care for individuals who are sick rather than keeping patients healthy. “The system focuses its resources primarily on treatment rather than prevention…The dearth of successful business models aimed at keeping people healthy highlights one of the central challenges of the growing corporatization of health care: how to make money producing health, not just health care. The path to doing so will require fundamental changes in the incentives for individuals and institutions and, potentially, broader structural change by policymakers to increase access to or financial support for basic preventive care.”
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
Background: “Long-term relief of drooling remains a challenge due to the side effects of anticholinergics,13 and botulinum neurotoxin type A injections provide only a temporary relief of drooling with potential loss of effect after repeated injections.15…Surgery for drooling is often considered if moderate to severe drooling persists in children after the age of 12 years.”
Submandibular duct relocation (SMDR) “is currently considered the first choice among these surgical procedures and involves the relocation of the submandibular duct papillae to the base of the tongue, allowing saliva to flow posteriorly into the oropharynx and trigger the swallowing reflex…Since the saliva is rerouted to the oropharynx, an adequate pharyngeal swallowing phase is a prerequisite for this surgery to prevent saliva aspiration and choking. Thus, SMDR is contraindicated in patients at risk of aspiration… In these cases, SMGE [submandibular gland excision] or SDL [submandibular duct ligation] can be considered.19“
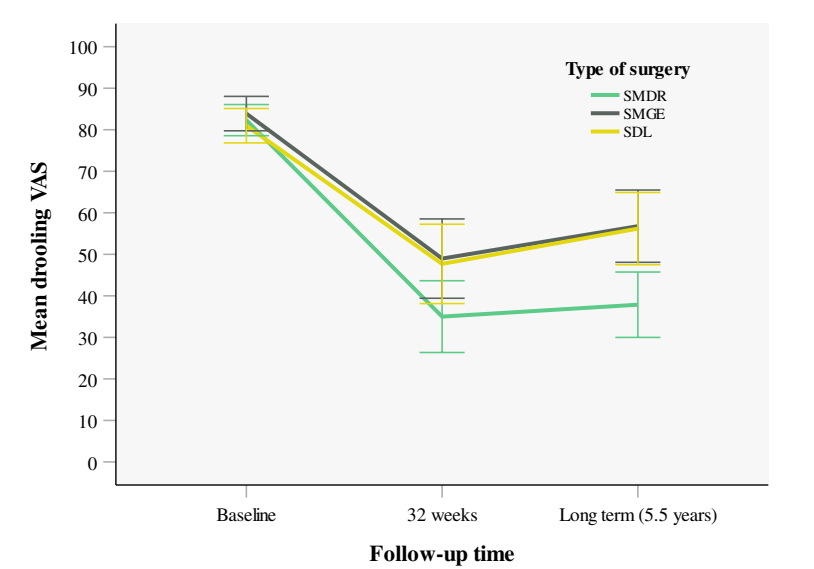
Methods: This was a retrospective cohort study with 255 patients. The authors used the visual analog scale (VAS) for drooling as the primary outcome to compare the long-term treatment outcomes of submandibular duct relocation (SMDR), submandibular gland excision (SMGE), and submandibular duct ligation (SDL) for the treatment of anterior drooling in individuals with neurodevelopmental disabilities.
Key findings:
A mean reduction in VAS was observed of 44.9 points for SMDR (P < .001), 27.2 for SMGE (P < .001), and 25.4 for SDL (P < .001).
A significant degree of drooling recurrence was observed after SDL and SMGE at long-term follow-up
Discussion points:
“SMDR is an invasive treatment requiring a night of postsurgical intubation and observation in intensive care. In specifically vulnerable children, less invasive alternatives such as SDL might therefore be preferential.”
“Since drooling is predominantly caused by insufficient swallowing, maintaining a balance between saliva production and clearance through swallowing is essential. SMGE and SDL inhibit saliva secretion from the submandibular glands, thereby reducing the overall volume of saliva produced.19,20 However, these procedures do not actively influence the swallowing process…A durable effect after SMGE and SDL is therefore achievable only if the reduction in saliva production reaches a threshold where the volume of saliva produced matches or falls below the individual’s capacity to swallow it effectively. On the other hand, after SMDR, the swallowing frequency itself probably increases.”
Selection bias: “SMDR was contraindicated for patients with inadequate swallowing… leads to a selection of less vulnerable patients with more favorable characteristics to undergo the SMDR procedure.” Thus, the improved results from SMDR over the other techniques is likely related to selection bias, though the authors adjusted the analysis “for differences in cognitive and oral motor functioning.”
My take: Excessive drooling is a common problem in children with neurodevelopmental disabilities. This study provides useful data on surgical management.