CL Bowlus et al. Hepatology 2023; 77: 659-702. Open Access! AASLD practice guidance on primary sclerosing cholangitis and cholangiocarcinoma
This is a lengthy article with a great deal of useful information. Here are some of the important recommendations most relevant for pediatric gastroenterologists/hepatologists:
- In patients with PSC without known inflammatory bowel disease (IBD), diagnostic colonoscopy with histological sampling should be performed and may be repeated every 5 years if IBD is not initially detected
- In patients with PSC in whom IBD is diagnosed, high‐definition surveillance colonoscopy with biopsies should start at age 15 years and be repeated at 1‐year to 2‐year intervals to evaluate for colonic dysplasia
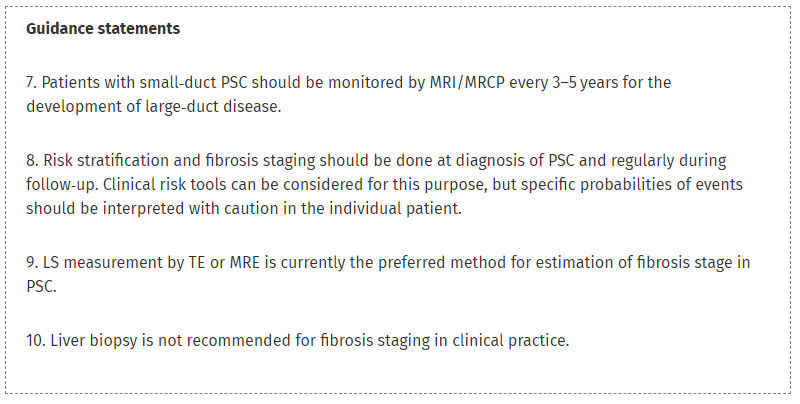
- New clinical risk tools for PSC are available for risk stratification, but probabilities of events in individual patients should be interpreted with caution
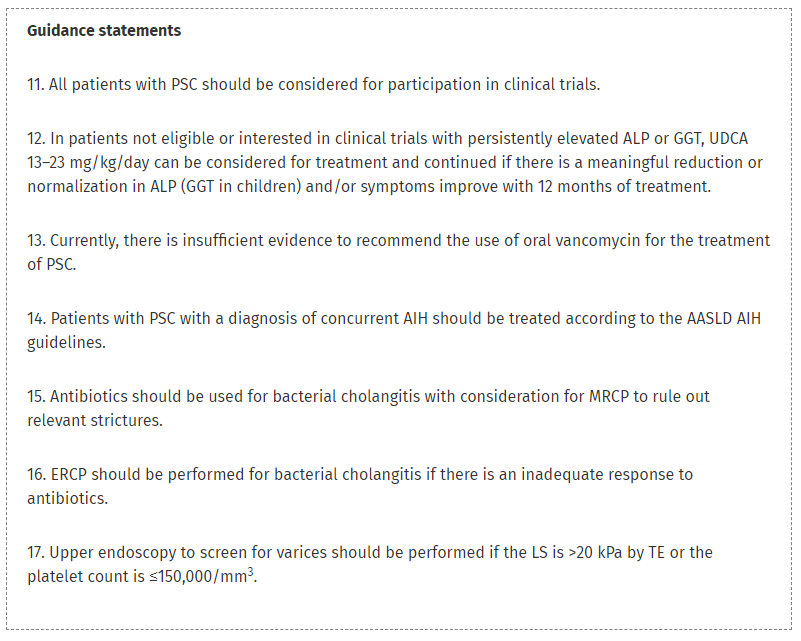
- All patients with PSC should be considered for participation in clinical trials; however, ursodeoxycholic acid (13–23 mg/kg/day) can be considered and continued if well tolerated with a meaningful improvement in alkaline phosphatase (γ‐glutamyl transferase in children) and/or symptoms with 12 months of treatment
- Upper endoscopy to screen for varices should be performed if the LS is >20 kPa by TE or the platelet count is ≤150,000/mm3
- Bone density examinations should be performed to exclude osteopenia or osteoporosis at diagnosis and at 2‐year to 3‐year intervals thereafter based on risk factors

Related blog posts:
- Aspen Webinar 2021 Part 5 -Autoimmune Liver Disease & PSC
- Long-Term Outcomes of Pediatric Patients with Sclerosing Cholangitis in the Setting of Inflammatory Bowel Disease
- Active Colitis More Likely in Children in Clinical Remission Who Have PSC and IBD
- Big Study of PSC in Children
- Primary Sclerosing Cholangitis (PSC) –Natural History Study
- Easy Advice for Pediatric Hepatologists: PSC Surveillance Recommendations
- PSC in IBD (2022)
- Recurrent PSC in Children After Liver Transplantation
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.