Methods: This was a two-part study: “(i) a detailed single-patient case of wheat-triggered, endoscopy-confirmed colitic FPIES treated with dupilumab 300 mg subcutaneously every two weeks and (ii) a prospective follow-up of seven additional FPIES patients all of whom initiated dupilumab for approved comorbidities. Serial flow cytometry quantified dendritic-cell OX40L and CD8+ CRTH2+ T-cell subsets before and after treatment; open food challenges assessed clinical tolerance.”
Key Findings:
Index case: Within two injections of dupilumab, the wheat sensitive patient tolerated a 50 g wheat protein challenge without gastrointestinal symptoms—this was the first uneventful exposure in 20 years. Discontinuation of dupilumab led to relapse; re-initiation again restored clinical tolerance
Cohort: All seven additional patients (ages 2–58 yr; triggers: milk, soy, rice, wheat, shellfish) achieved unrestricted dietary tolerance within three months
An important finding in the index case as well as the follow up cohort is the dupilumab induced drop in dendritic cell OX40L. OX40L is a TNF-superfamily co-stimulatory molecule induced on dendritic cells and other antigen-presenting cells.
My take: Dupilumab appears to be a promising medication for FPIES and warrants further study. If confirmed to be effective, it is likely to be targeted to those with approved comorbidities and those with more severe presentations.
Part A -In this phase 3 trial, we randomly assigned, in a 2:2:1:1 ratio, patients 1 to 11 years of age (n=102) with active eosinophilic esophagitis who had had no response to proton-pump inhibitors to 16 weeks of a higher-exposure or lower-exposure subcutaneous dupilumab regimen or to placebo (two groups)
Part B- At the end of Part A, eligible patients in each dupilumab group continued the same regimen and those in the placebo groups were assigned to higher-exposure or lower-exposure dupilumab for 36 weeks
Key findings:
In Part A, histologic remission occurred in 25 of the 37 patients (68%) in the higher-exposure group, in 18 of the 31 patients (58%) in the lower-exposure group, and in 1 of the 34 patients (3%) in the placebo group
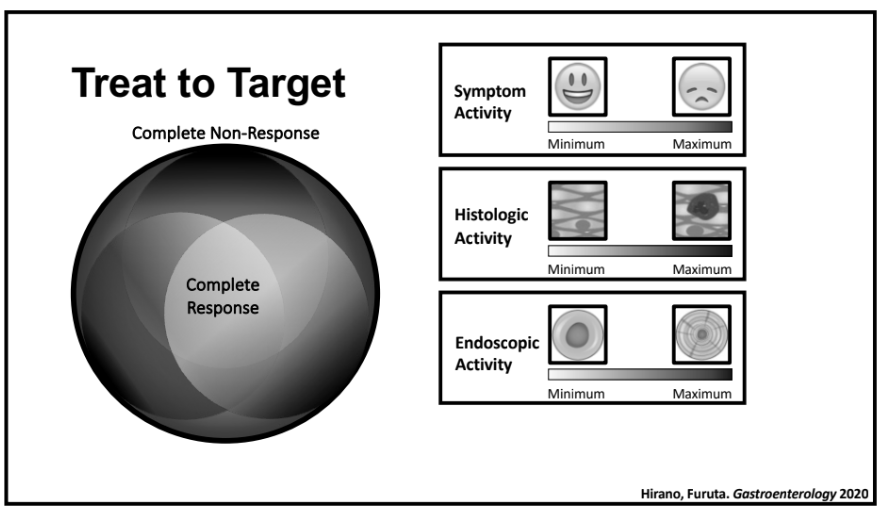
The higher-exposure dupilumab regimen led to significant improvements in histologic, endoscopic, and transcriptomic measures as compared with placebo
The improvements in histologic, endoscopic, and transcriptomic measures between baseline and week 52 in all the patients were generally similar to the improvements between baseline and week 16 in the patients who received dupilumab in Part A
Similar adverse effects were noted across all groups. There was an increased rate (at least 10%) of COVID infections in participants receiving dupilumab whereas the incidence of vomiting was at least 10 percentage points lower among patients who received dupilumab (either group) than among those who received placebo
My take: Dupilumab is an effective option for eosinophilic esophagitis.
Rationale for the retrospective study: ” Although it is the first Food and Drug Administration–approved treatment for EoE, eligibility criteria for the clinical trial program excluded several characteristics of the most severe EoE patients seen in clinical practice…Therefore, the purpose of this study was to determine the real-world efficacy of dupilumab in patients with severe, treatment-refractory, and fibrostenotic EoE.”
This cohort of 46 patients with severe disease including 39 (85%) who had prior esophageal dilatation (mean of 9). Patients had a mean age of 39 and had had symptoms for a mean of 13 years. Patients were considered treatment-refractory as all had received PPIs and topical steroids; in addition, most (87%) had tried elimination diets.
Key findings:
The peak eosinophil counts decreased markedly, and postdupilumab histologic response rates were 80% and 57% for fewer than 15 eosinophils per high-power field and 6 or fewer eosinophils per high-power field, respectively. Mean eosinophil count dropped from 70 to 9 following dupilumab treatment.
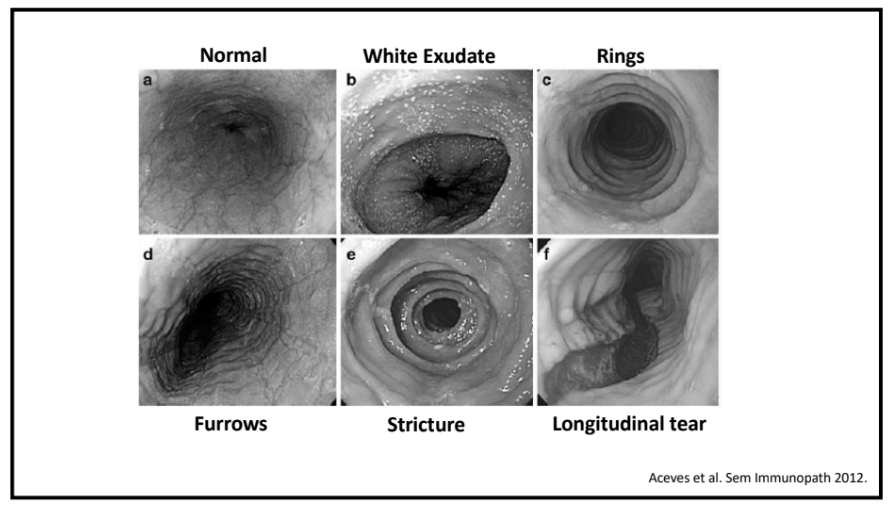
The Endoscopic Reference Score (EREFS) decreased from 4.62 to 1.89 with improvement in all categories: exudates, rings, edema, furrows and strictures.
Global symptom improvement was reported in 91% (P < .001).
My take: Many clinical studies are not representative of typical patients with various ailments, often excluding those with the most severe manifestations. This study indicates that dupilumab is an effective agent for patients with severe fibrostenotic eosinophilic esophagitis.
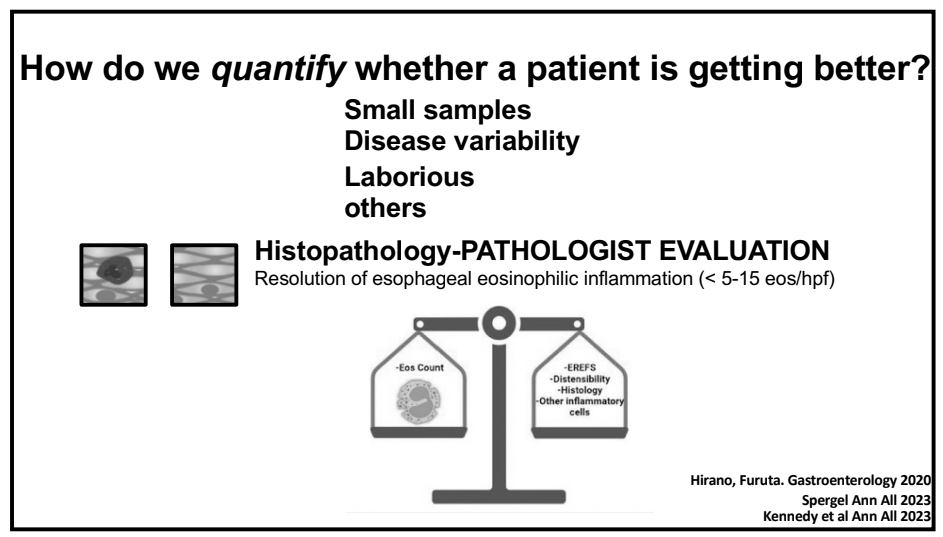
We recently had Glenn Furuta, MD give our group a terrific lecture on eosinophilic esophagitis (EoE).
Some of the key points:
The burden of EoE continues to increase.
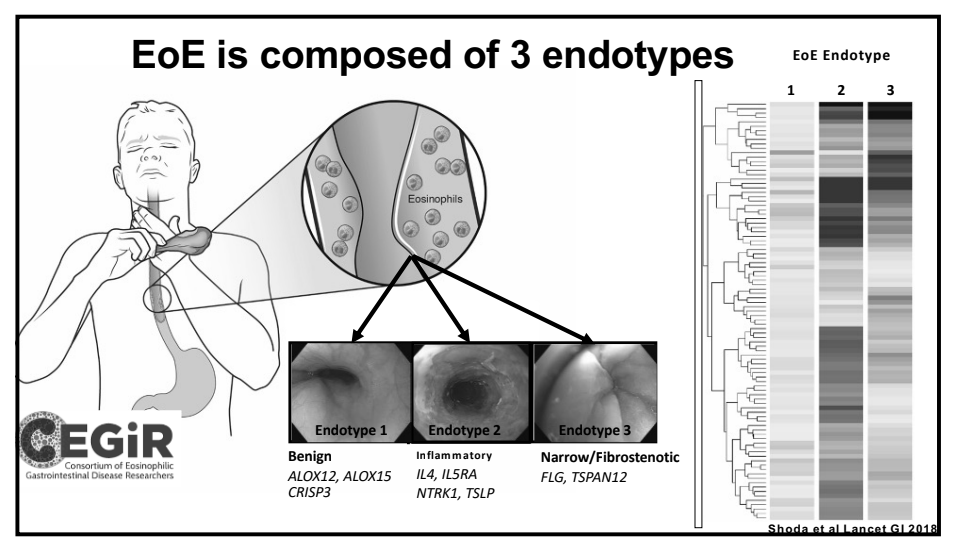
There are clearly several phenotypes of EoE. Some patients may never develop stricturing/fibrostenotic disease but natural history data continues to evolve.
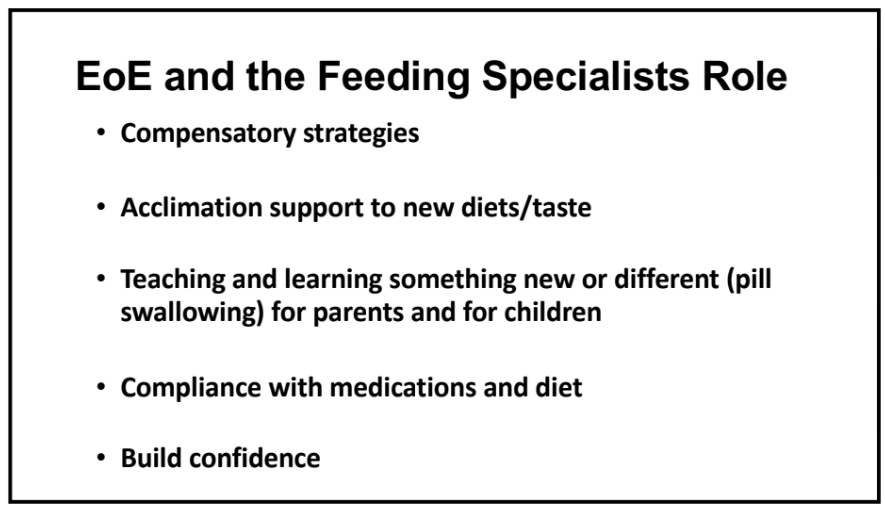
After treatment response, many patients can continue with symptoms. In adults and adolescents, this has been termed ‘esophageal hypervigilance.’ Feeding therapy may be helpful in this circumstance.
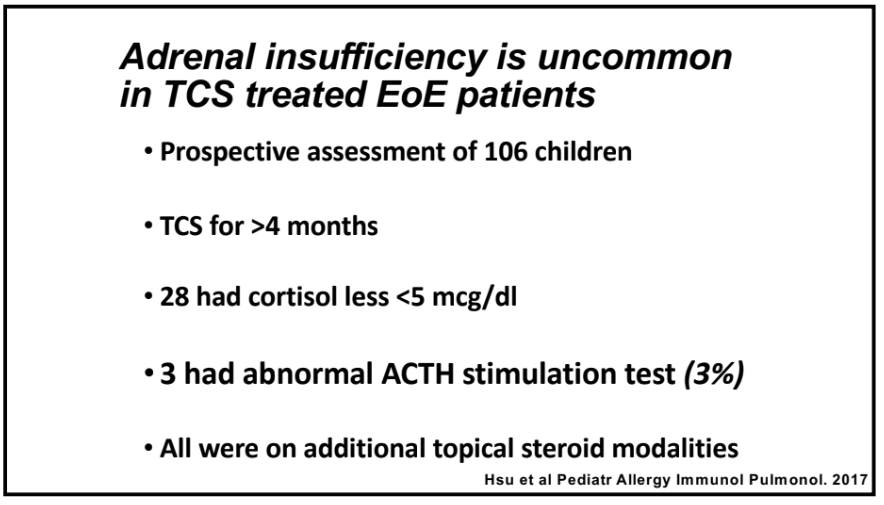
Adrenal insufficiency: Currently their group tries to screen for this after 4 months of topical corticosteroids and then yearly. It is unusual for them identify adrenal insufficiency if the patient is receiving only a single steroid agent; patients receiving steroids for other conditions like asthma are at higher risk.
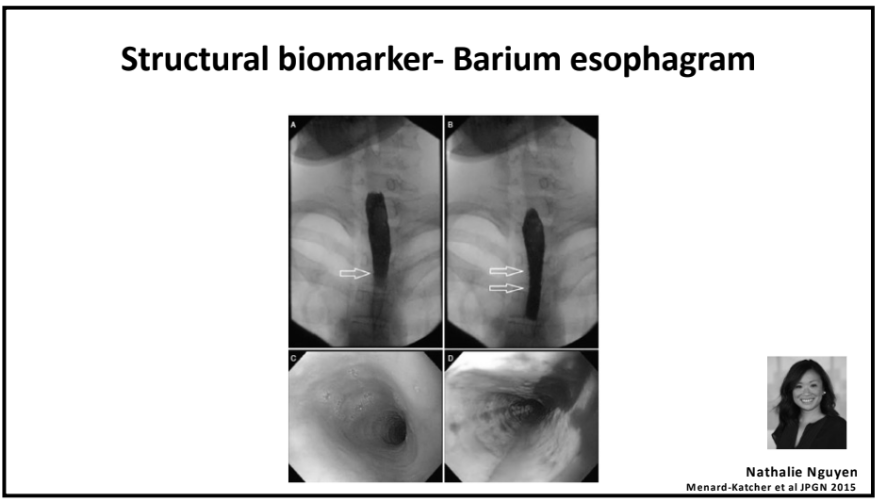
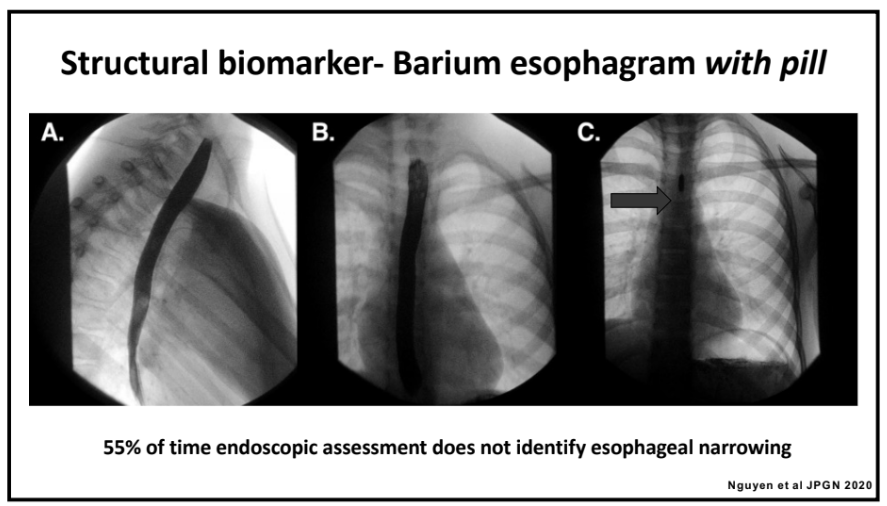
An esophagram with a barium coated pill can be a useful adjunct to determine if there is esophageal narrowing (this can be missed on endoscopy).
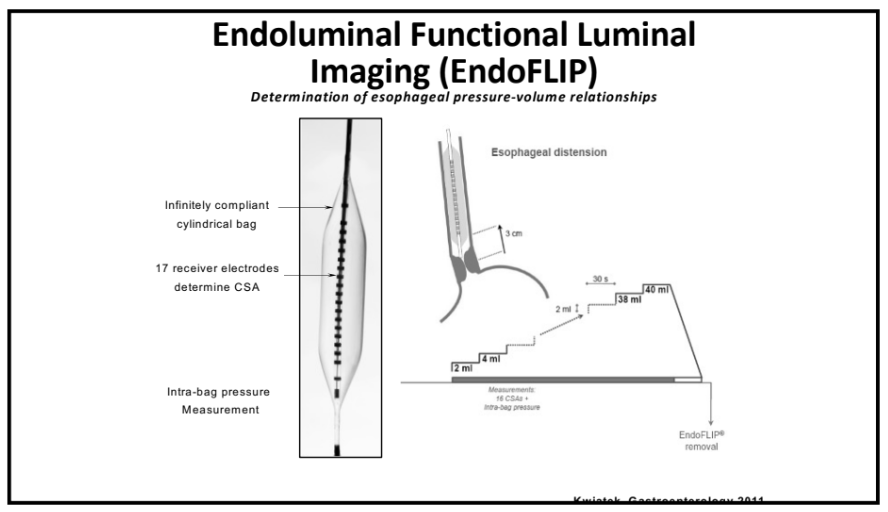
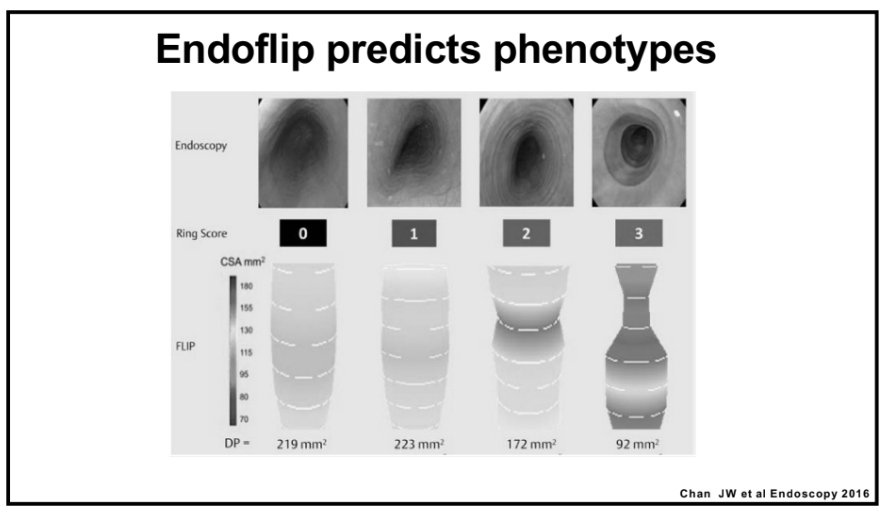
For select patients, endoFLIP can characterize distensibility/esophageal function
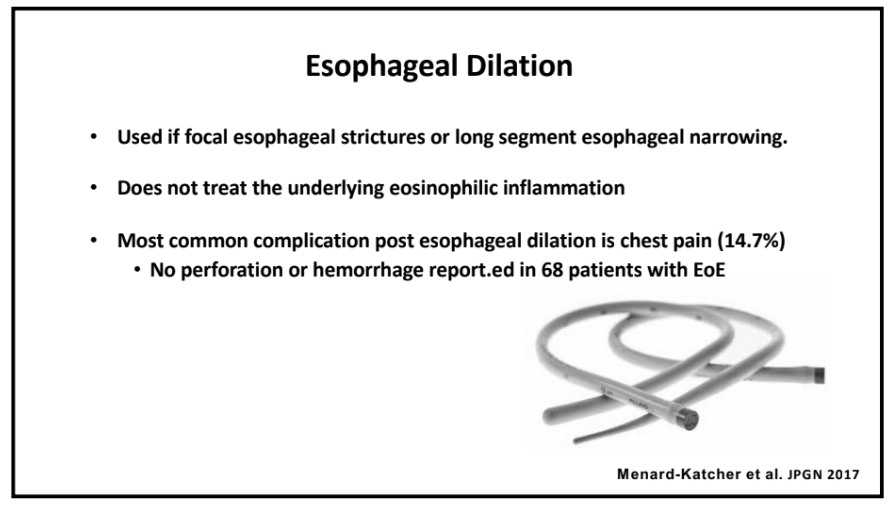
Esophageal strictures: Their group uses Bougie dilators and has had a good experience. No perforations. ~15% with chest pain afterwards.
Corticosteroids (topical) can reduce the risk of food impactions in adults.
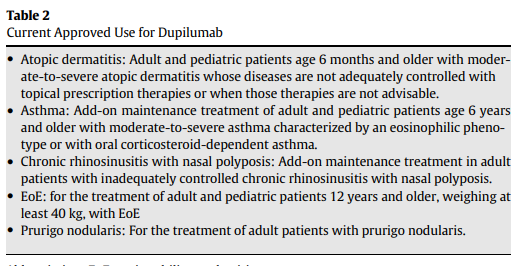
Reviewed use of Dupilimab and its recent approval in EoE for children as young as 1 yr of age (>15 kg)
“Regeneron Pharmaceuticals, Inc. (NASDAQ: REGN) and Sanofi today announced that the U.S. Food and Drug Administration (FDA) has approved Dupixent® (dupilumab) for the treatment of pediatric patients aged 1 to 11 years, weighing at least 15 kg, with eosinophilic esophagitis (EoE).”
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
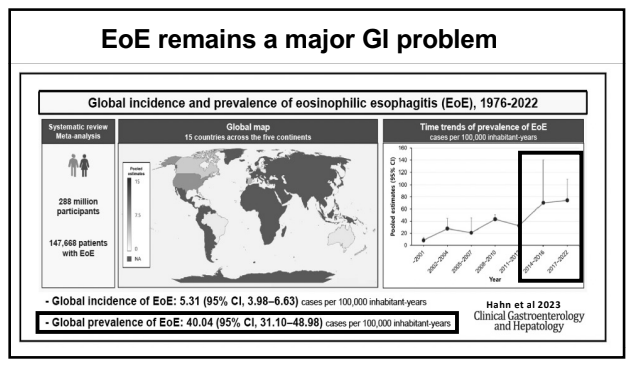
This research utilized 40 studies which met the eligibility criteria, including over 288 million participants and 147,668 patients with EoE from 15 countries across the five continents.
Key findings:
The global pooled incidence and prevalence of EoE were 5.31 cases per 100,000 inhabitant-years and 40.04 cases per 100,000 inhabitant-years, respectively.
The pooled prevalence and incidence of EoE were higher in high-income countries, males, and North America.
The pooled prevalence and incidence of EoE have increased from 1976 to 2022.
Time trends of incidence (A) and prevalence (B) of EoE, 1976 to 2022. Pooled estimates, cases per 100,000 inhabitant-years.
“This review summarizes the data leading to FDA approval for dupilumab and provides a practical approach for clinical use of dupilumab.” Dupilumab, a humanized monoclonal antibody that blocks interleukin (IL)-4 receptor alpha, is currently the only FDA-approved medication for EoE. It is noted that in the trials leading to FDA approval, all patients were PPI refractory and ~70% had received topical steroids (with about half either intolerant or nonresponsive).
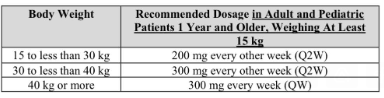
Dosing: 300 mg weekly injection with a single-dose prefilled autoinjector pen or a syringe with a needle shield. It is recommended that refrigerated medicine is brought to room temperature for at least 45 minutes prior to injection. It “can remain unrefrigerated up to 14 days.”
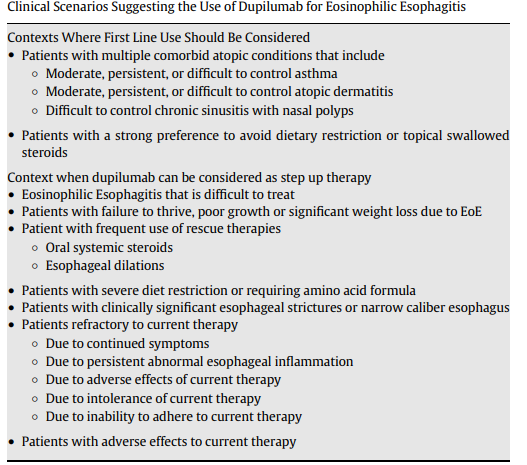
In Figure 1, the articles details positioning of use of dupilumab in EoE management algorithm:
New diagnosis, patient preference
Additional atopic condition with approved dupilumab use (strong indication)
Lack of response to current treatment (diet, PPI, swallowed steroids) or adverse effects from current treatment (strong indications)
“It is reasonable to repeat endoscopy with biopsy 24 weeks after initiation of dupilumab in many patients…However, endoscopy may be completer earlier” in selected patients.
At least 5 other biologics are in phase 2 or phase 3 studies (listed in Table 1).
My take: EoE is increasing in prevalence and new therapies (often expensive) are emerging.
Also, there is a fairly good patient education 7-page pamphlet from the makers of Dupixent encouraging patients with symptoms suggestive of EoE to speak with their physicians.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
This article summarizes updated recommendations for eosinophilic esophagitis from the Joint Task Force for the American Academy of Allergy Asthma Immunology and American College of Allergy Asthma Immunology and the American Gastroenterology Association (JTF-AGA). It offers a good number of recommendations regarding when using dupilumab should be considered.
Other Key Points:
“Dupilumab can be considered as first-line therapy in patients presenting with severe EoE”and in patients with multiple atopic diseases.
In addition, it recommends “performing a repeat EGD, along with obtaining biopsies, 5 to 6 months after either starting dupilumab therapy or whenever adjusting the dupilumab dose.” In some cases, like stricture dilatation, the authors indicate that earlier EGD may be appropriate.
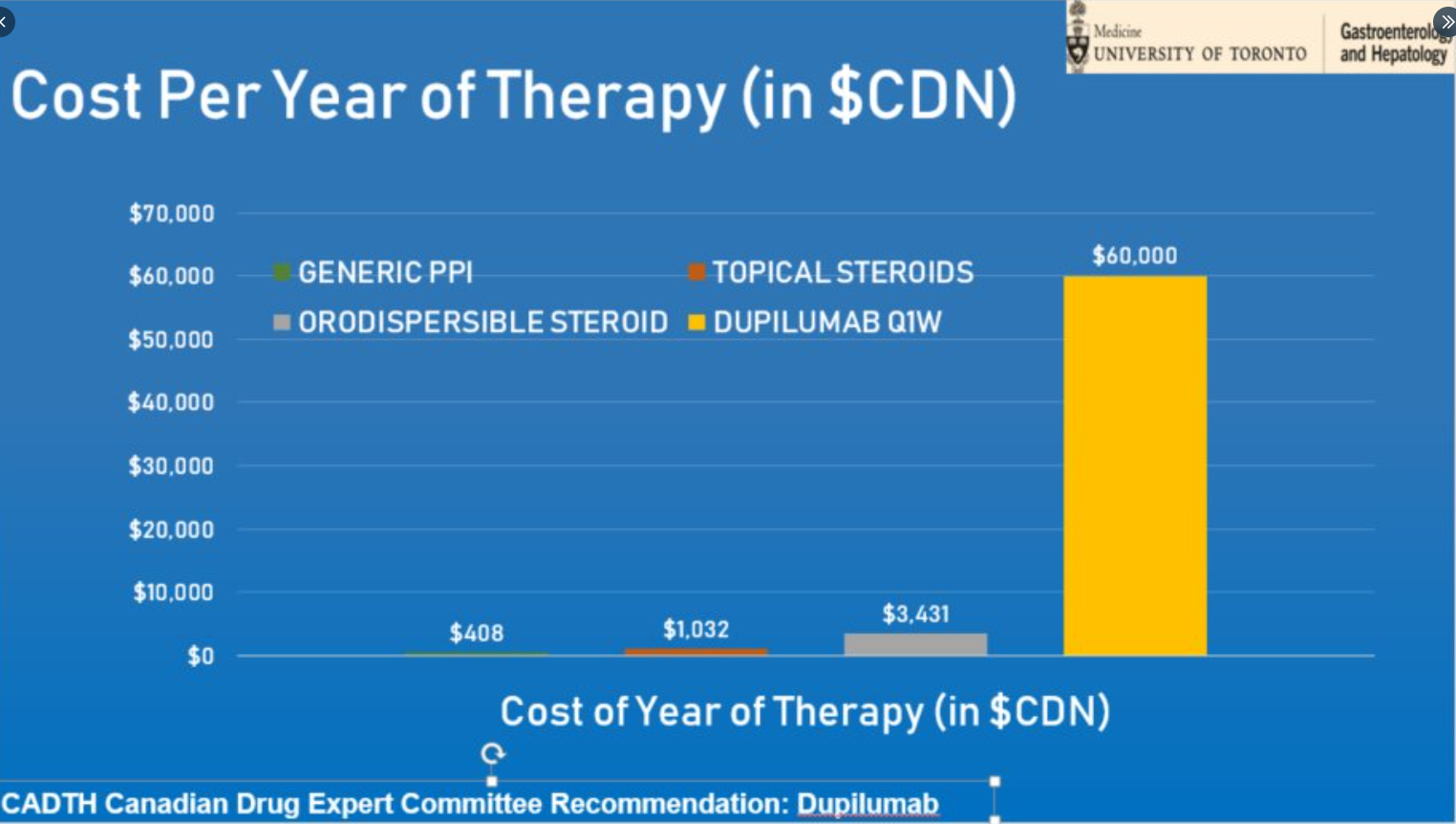
The advantages/disadvantages of current treatment options are summarized in Table 3. For dupiliumab, the disadvantages include its high price of dupilumab and weekly injections. Conjunctivitis has been an adverse effect identified in its usage with other indications.
My take: Dupilumab is a major advance for patients with EoE. Due to the need for weekly injections and its costs, it is likely a 2nd line agent for most kids with EoE.
Yesterday’s post reviewed the landmark study leading to dupilumab’s FDA approval. Today’s case report shows that we have a lot we need to learn about its use.
The authors present a case report of a patient with eosinophilic esophagitis (EoE) who had ongoing active EoE while receiving topical steroids (TS) and PPI (and previously dietary elimination therapy). He achieved remission after the addition of dupilumab. “When his TS were weaned after achieving remission, his disease relapsed with worsening of his dysphagia and a peak eosinophilic count (PEC) of 55 eosinophils per high power field (eos/hpf). Upon restarting TS to his ongoing dupilumab, symptoms fully resolved, and he achieved histologic remission (PEC 10 eos/hpf).”
My take: This study indicates that there are some patients need dupilumab and topical steroids in combination, rather than monotherapy. Reliable biomarkers to more easily determine response and/or to predict optimal therapy are clearly needed.
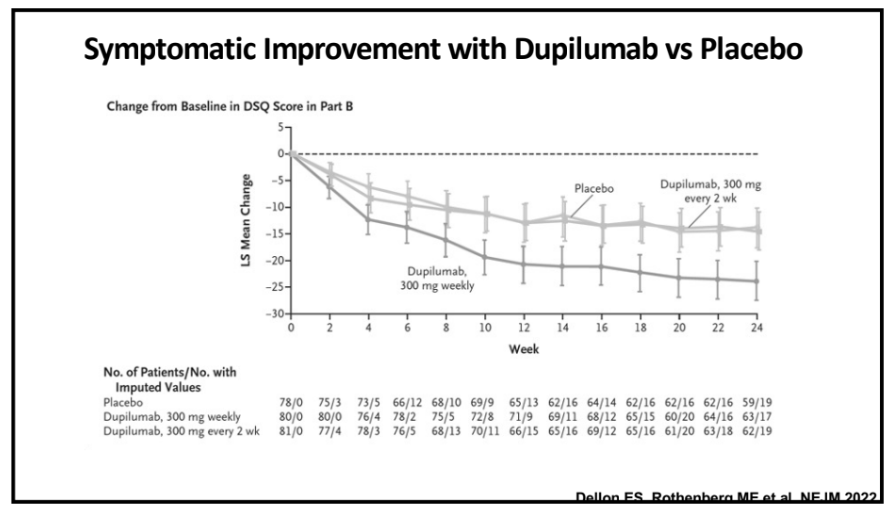
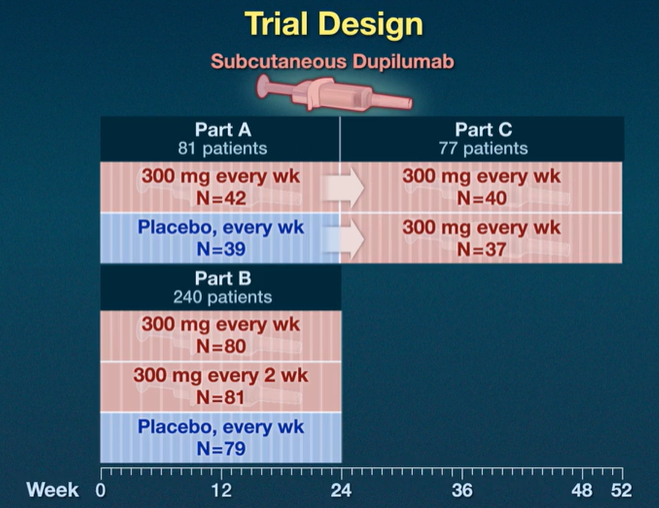
This study was pivotal for receiving FDA approval of dupilumab (dupixent) for the treatment of EoE (the only FDA approved therapy). Background: “Dupilumab, a fully human monoclonal antibody, blocks interleukin-4 and interleukin-13 signaling, which have key roles in eosinophilic esophagitis..Standard-of-care treatments for eosinophilic esophagitis include food elimination diets, proton-pump inhibitors (PPIs), swallowed topical glucocorticoids (applied to the esophagus by swallowing), and, in the case of strictures, esophageal dilation.11,12 However, the rates of response are variable (30 to 40% of patients may not have a response to first-line treatments).”
Key findings from three-part study (see images below):
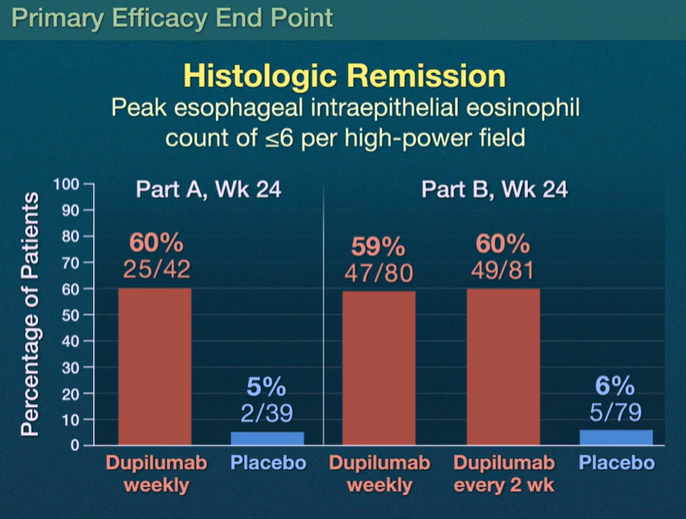
Part A: Histologic remission occurred in 25 of 42 patients (60%) who received weekly dupilumab and in 2 of 39 patients (5%) who received placebo
Part B: Histologic remission occurred in 47 of 80 patients (59%) with weekly dupilumab, in 49 of 81 patients (60%) with dupilumab every 2 weeks, and in 5 of 79 patients (6%) with placebo
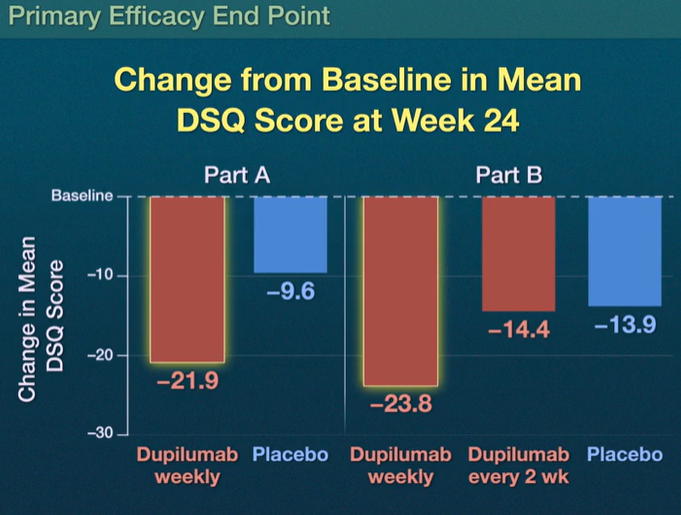
Dysphagia Symptom Questionnaire (DSQ) scores: the scores improved with weekly dupilumab as compared with placebo, with differences of –12.32 (95% CI, –19.11 to –5.54) in Part A and –9.92 (95% CI, –14.81 to –5.02) in Part B (both P<0.001) but not with dupilumab every 2 weeks (difference in Part B, –0.51; 95% CI, –5.42 to 4.41)
The most common adverse effect was injection site reactions. There were 10 serious adverse events; none of these “were considered by the trial investigators to be related to the trial regimen.”
In the associated commentary, (pg 2379-2380), Dr. Alex Straumann notes that since EoE is localized to the esophagus, whether a patients should be treated with a systemically acting medication, “particularly in light of the fact that topical glucocorticoids have been shown to be as efficacious as systemically acting prednisone.”
My take (borrowed in part from editorial): It remains unclear whether dupilumab “is better than the good old topical glucocorticoids in improving disease outcomes, particularly in light of considerable costs associated with this treatment.” Due to its cost (see below), dupillumab is likely best situated as a 2nd line treatment at this time for most patients.
Thank you to those who have helped me this past year with this blog –colleagues, friends and family. Wishing all of you a good 2023. Here are some of my favorite posts from this past year: