This was a multicenter, retrospective, case-control study of patients hospitalized with ASUC who underwent colectomy, comparing patients treated with tofacitinib (n=41) prior to colectomy with infliximab-treated controls (n=68).
Key findings:
Compared with tofacitinib-treated patients, infliximab-treated patients had higher overall rates of overall (44 [64.7%] vs 13 [31.7%]; P = .002) and serious (19 [27.9%] vs 3 [12%]; P = .019) postoperative complications
My take: This study supports the safety of JAK inhibitor therapy for ASUC. It showed a significantly lower rate of overall postoperative complications in ASUC patients treated with tofacitinib compared with infliximab; the authors note that “these findings can likely be extrapolated to upadacitinib, a selective JAK inhibitor, given its similar mechanism of action.”
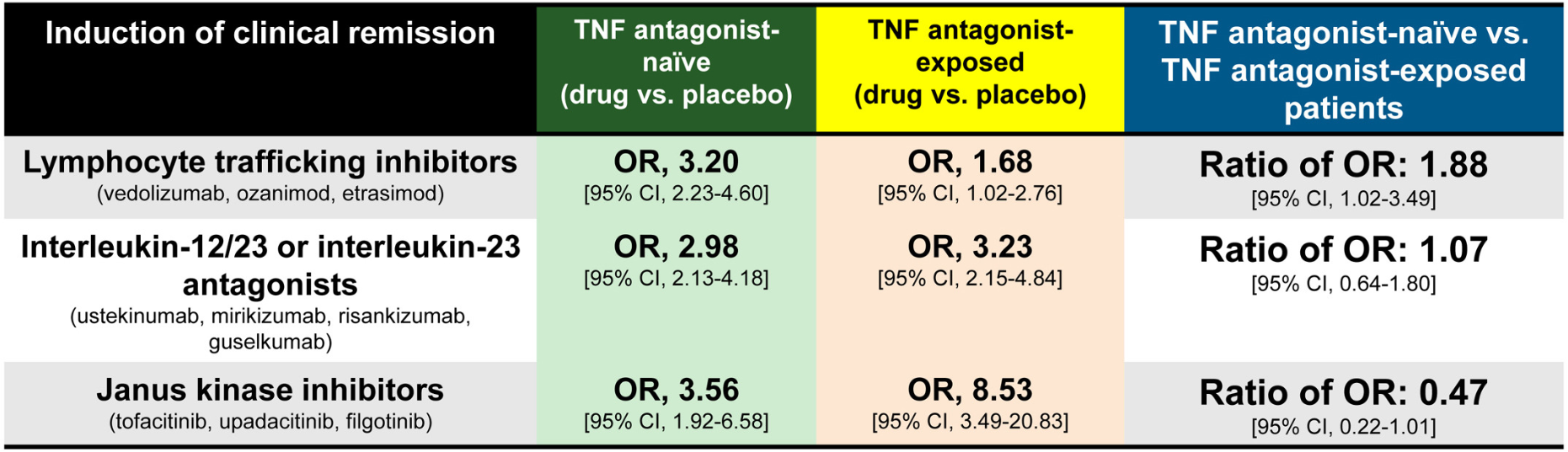
Methods: Meta-analysis of 17 randomized controlled trials in 8871 adults with moderate-severe UC. The authors calculatedthe ratio of odds ratio of achieving remission with active drug vs placebo, in TNF antagonist–naïve vs TNF antagonist–exposed patients.
Key findings:
JAK inhibitors: Less efficacious in TNF antagonist–naïve vs exposed patients (6 trials; ratio of OR, 0.47)
IL-23 antagonists: No significant difference was observed in efficacy of selective interleukin-23 antagonists vs placebo in TNF antagonist–naïve vs exposed patients (6 trials; ratio of OR, 1.07)
Lymphocyte trafficking inhibitors: More efficacious in TNF antagonist–naïve vs exposed patients (5 trials; odds ratio [OR], 1.88)
Discussion:
This study “confirmed prior observations that exposure to TNF antagonists significantly reduces the efficacy of lymphocyte trafficking inhibitors in inducing remission, including both vedolizumab and S1P receptor modulators, by approximately 50%.In contrast, prior exposure to TNF antagonists was associated with a significant increase in the efficacy of JAK inhibitors in inducing remission, with 2-fold higher efficacy in TNF antagonist–exposed vs TNF antagonist–naïve patients”
In the SELECT-COMPARE trial in patients with rheumatoid arthritis, there was also an improved response to upadacitinib in patients with prior adalimumab.
“The current findings raise the intriguing possibility that exposure to TNF antagonists could result in lasting effects on the immune system that differentially alter responsiveness to therapies with distinct mechanisms of action”
My take: This study suggests that JAK inhibitors are a good choice for secondary therapy after anti-TNF agents. Other factors, besides efficacy, including safety, extraintestinal manifestations, and cost, have to be considered as well.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
This is a 60 page open access article. Table 1 lists 34 “GRADE” statements and Table 2 lists 35 consensus statements. This article is also jointly published in the following:
Gut
Am J Gastroenterol
Inflammatory Bowel Diseases
Journal of Crohn’s and Colitis
Aliment Pharmacol Ther
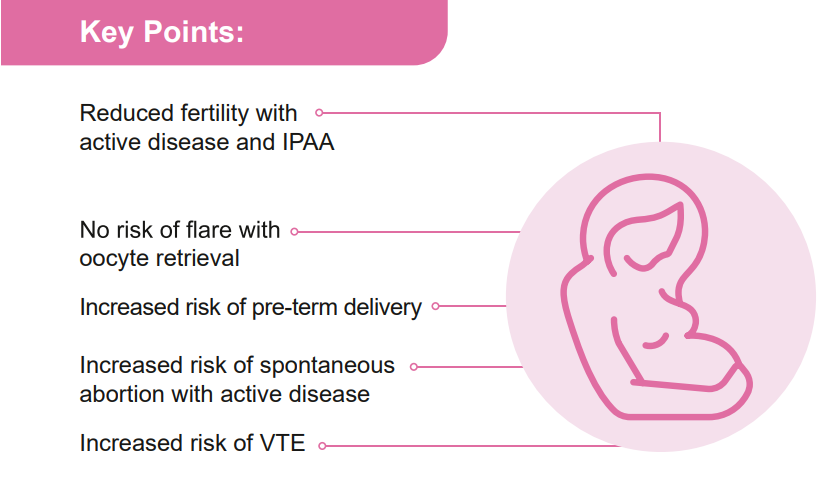
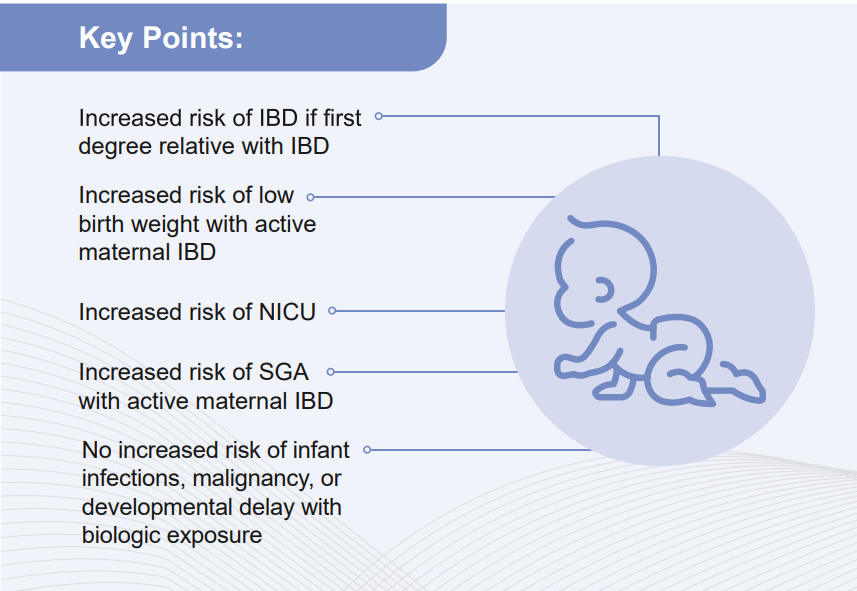
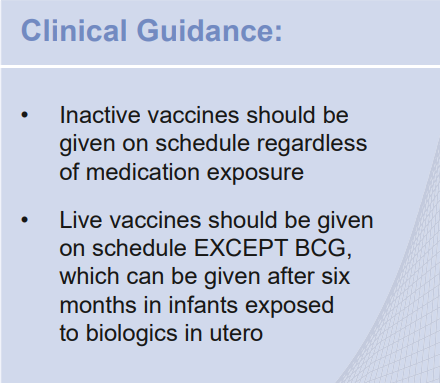
For Moms:
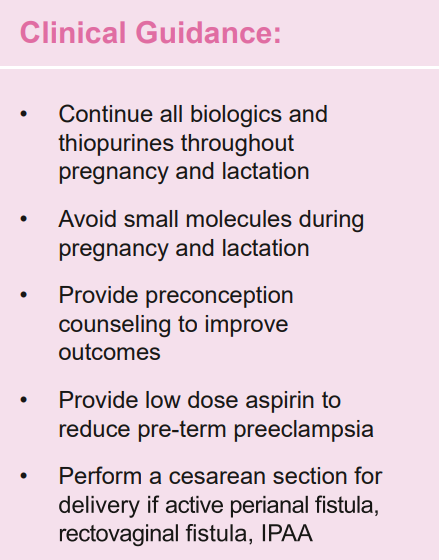
For Babies:
My take: This is a useful reference –mainly helpful for gastroenterologists rather than pediatric providers.
Mehtods: This international, multicenter, retrospective cohort study consecutively enrolled JAK-inhibitor-treated patients with IBD who subsequently developed acne (aka JAKne).
Key findings:
Among 2183 JAK inhibitor–treated patients with IBD, 272 developed acne
70% of acne cases occurred within the first 3 months of treatment initiation
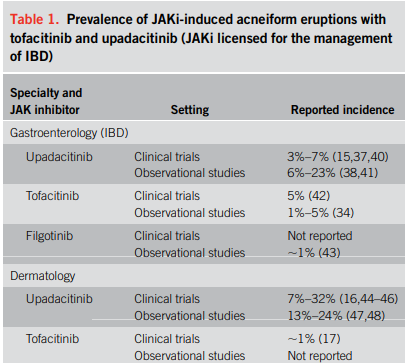
The crude prevalence rates of acne were 15.9% for upadacitinib, 4.3% for tofacitinib, and 1.9% for filgotinib, with dose-dependent relationships observed for upadacitinib and tofacitinib
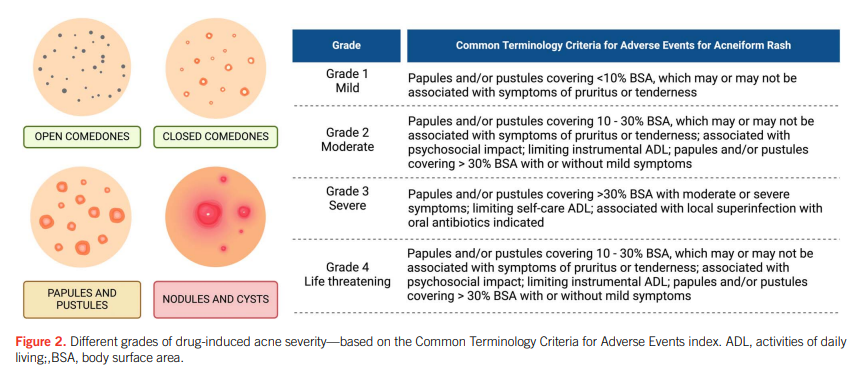
Most cases were mild-moderate in severity. Mild (<10% of body surface area) was noted in 68%, Moderate (10-30% of BSA) was noted in 24%, and Severe (>30% of BSA) was note in 8%
Among those who developed acne, areas that were affected included the face in 89%, the back in 33%, the chest in 27% and the scalp in 1%
40% received pharmacologic intervention
18% of patients who developed acne had JAK inhibitor dose reduction or discontinuation
My take: JAKne is a common adverse effect. Early identification, proactive counseling, and timely interventions, such as dose reduction, acne therapies or referral to dermatology, are crucial in managing this side effect.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
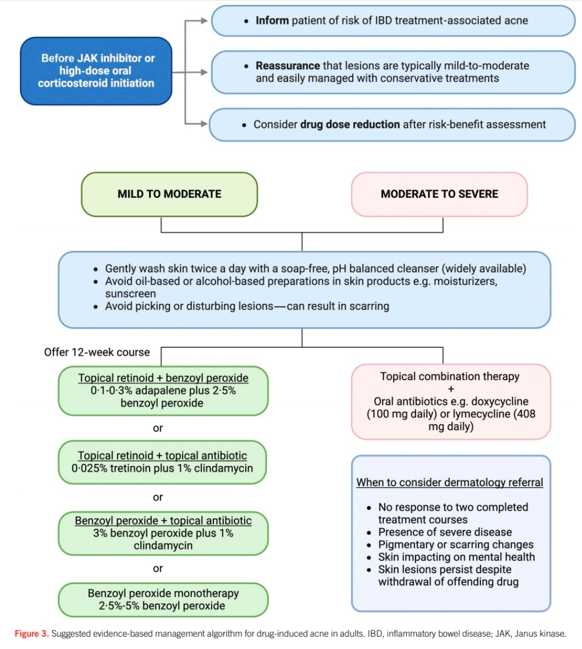
“Corticosteroids and Janus kinase inhibitors (JAKi) are commonly used for the treatment of inflammatory bowel disease (IBD) and are known to aggravate a prior tendency to acne or trigger the development of new acneiform eruptions. Both randomized controlled trials and real-world studies have identified acne as one of the most common treatment-emergent adverse events in JAKi… This review examines the characteristics of drug-induced acne in IBD treatments, provides a practical guide for gastroenterologists to manage mild-to-moderate occurrences, and highlights when to seek specialist dermatology advice.”
My take: This is a helpful review of acne management in the setting of IBD.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
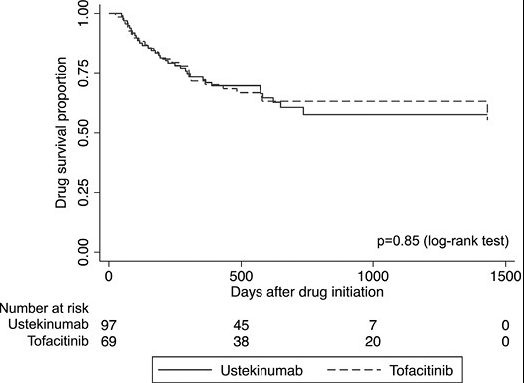
In this real-world cohort of anti-TNF-exposed patients with ulcerative colitis, tofacitinib (n=69) and ustekinumab (n=97) demonstrated similar effectiveness in achieving steroid-free clinical remission (SCFR) at 12 and 52 weeks. The median follow-up was 88.0 and 62.0 week, respectively. 35 of 66 in the tofacitinib cohort had dose reduction from the starting dose of 10 mg twice daily. This reduction occurred at a mean of 144 days. 59 of 97 in the ustekinumab cohort received either Q4W dosing (n=43) or Q6W (n=16).
Key findings:
53% of patients receiving tofacitinib and 32% of patients receiving ustekinumab achieved SFCR at 12 weeks. Tofacitinib-treated patients had higher baseline Mayo endoscopic subscores and CRPs.
At 52 weeks, approximately 50% of patients in both treatment groups achieved SFCR. There were also high proportions (>60%) of patients in both treatment groups who had endoscopic response within 52 weeks.
Both drugs were well-tolerated, as only 1 patient in each treatment group discontinued therapy due to an AE during >260 patient-years of follow-up.
My take: This shows similar response to either tofacitinib and ustekinumab in a cohort that had refractory disease as patients were anti-TNF failures and most had prior vedolizumab as well.
On May 30, 2018, the US Food and Drug Administration (FDA) expanded the indication of tofacitinib (Xeljanz; Pfizer), an oral Janus kinase (JAK) inhibitor, for the treatment of adults with moderately to severely active ulcerative colitis. However, the optimal dosing remains unclear.
In this “real-world” study by Yu et al, a retrospective review of 162 patients was conducted (2012-2022). 52% continued 10 mg twice daily while 48% underwent dose de-escalation to 5 mg twice daily. The primary outcome was evidence of UC disease activity–related events: hospitalization/surgery, corticosteroid initiation, tofacitinib dose increase, or therapy switch.
Key findings:
Cumulative incidence rates of UC events at 12 months were similar in patients with and without dose de-escalation (56% vs 58%; P = .81)
An induction course with 10 mg twice daily for more than 16 weeks was protective of UC events (hazard ratio [HR], 0.37) while ongoing severe disease (Mayo 3) was associated with UC events (HR, 6.41)
Twenty-nine percent of patients with UC events had their dose re-escalated to 10 mg twice daily, with only 63% able to recapture clinical response at 12 months
Discussion Points:
“Although the product label recommends dose de-escalation after 8 or 16 weeks, clinical practice is variable in the real-world setting… In this retrospective real-world study of moderate to severe UC patients with almost half undergoing dose de-escalation, we observed that more than half of patients experienced a UC disease activity–related event within 12 months after dose de-escalation, particularly in patients with an induction course of fewer than 16 weeks and active endoscopic disease at 6 months after induction…”
” Although dose de-escalation is preferable for long-term maintenance therapy to reduce the potential lifetime risk of medication-related adverse events [eg. VTE], it must be balanced with sustained remission to prevent short- and long-term disease-related complications.”
“In the OCTAVE study which reported higher rates of long-term remission, patients de-escalated only after having shown clinical and endoscopic remission after 52 weeks on tofacitinib 10 mg twice daily”
My take (borrowed from authors): “Emphasis should be placed on clinical and endoscopic evidence of improvement before consideration of dose de-escalation to ensure the highest probability of treatment success.” This advice, though, may conflict with product labelling which states that “tofacitinib induction with 10 mg twice daily beyond 16 weeks is not recommended; in fact, it is recommended to stop after 16 weeks if adequate response has not been achieved.”
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
This is third day summarizing some of the talks at the regional CCFA conference. Erin Forster presented on Treatment with Oral Advanced Therapy. Below are my notes and some of the slides; my notes may have errors of omission or transcription. Can get access to full slide set: (n=22) here: Treatment with Oral Advanced Therapy
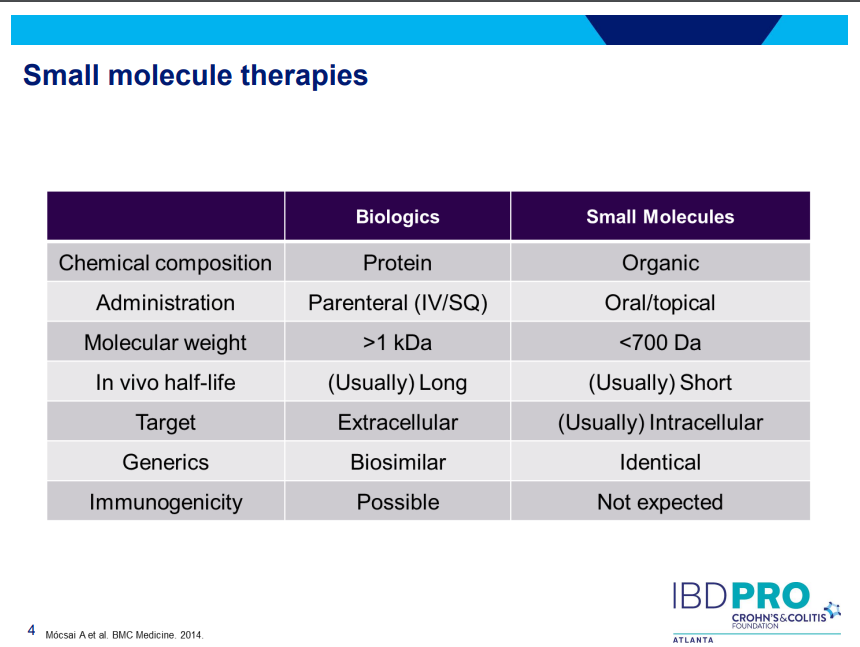
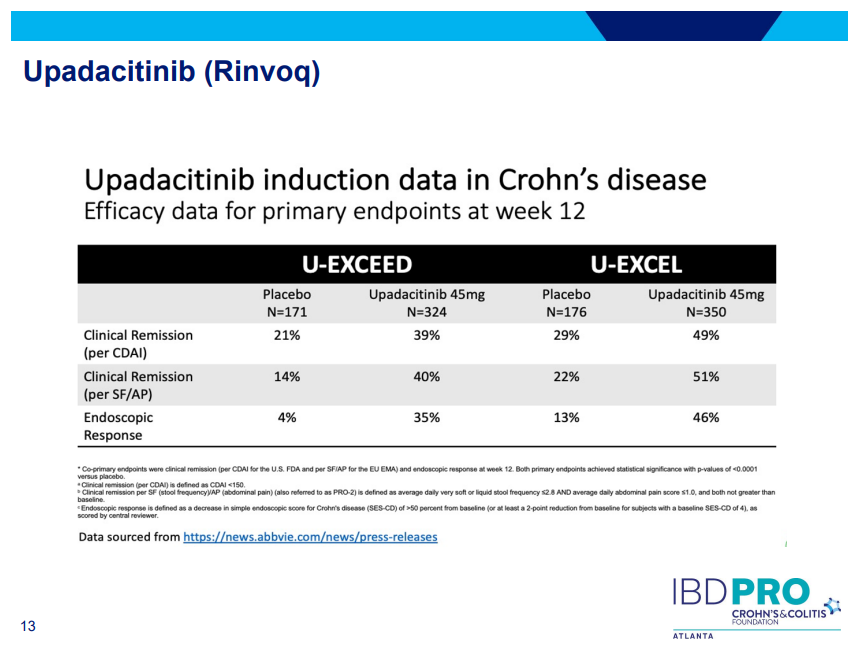
JAK inhibitors (Tofacitinib, Upadacitinib) have rapid onset of action and are taken orally
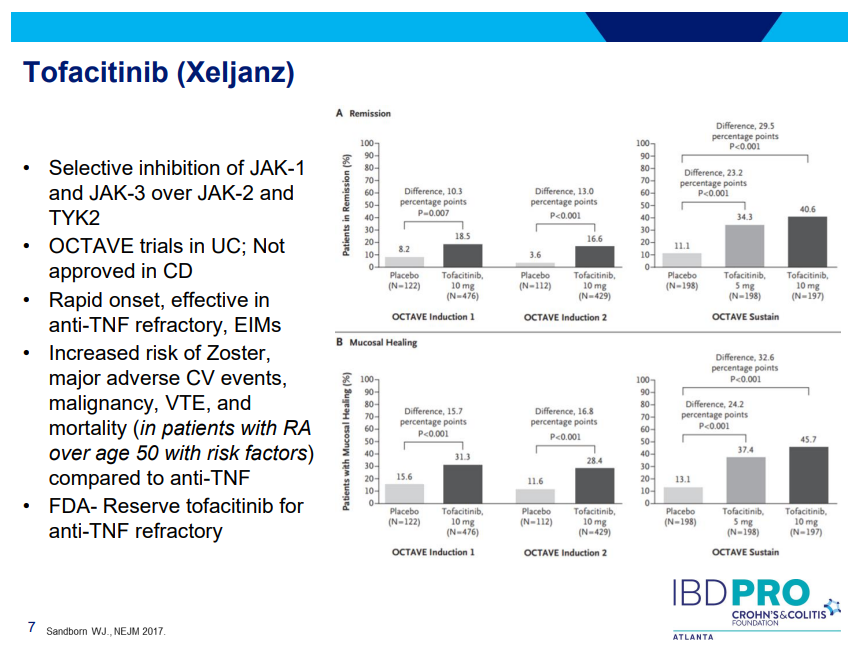
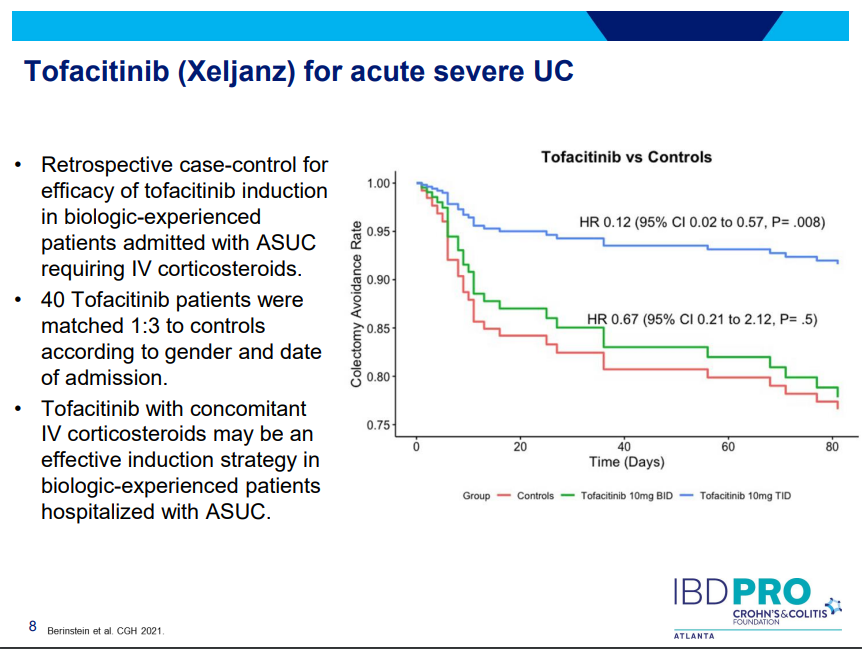
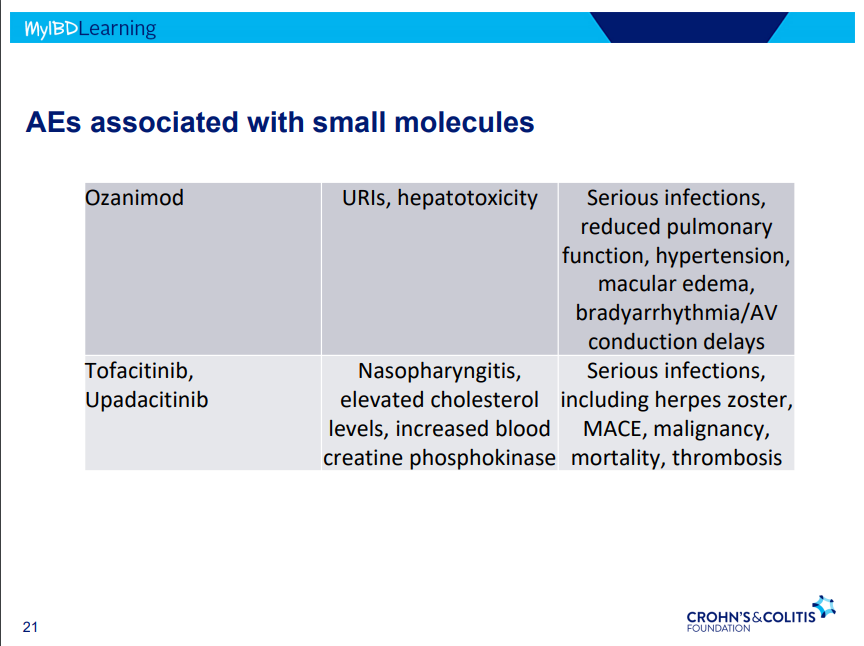
Tofacitinib (Xeljanz) -concern about cardiovascular events was derived from elderly rheumatologic patients. Cardiovascular events are rare. Higher dose (TID) (in the hospital) associated with lower colectomy rates in acute severe ulcerative colitis.
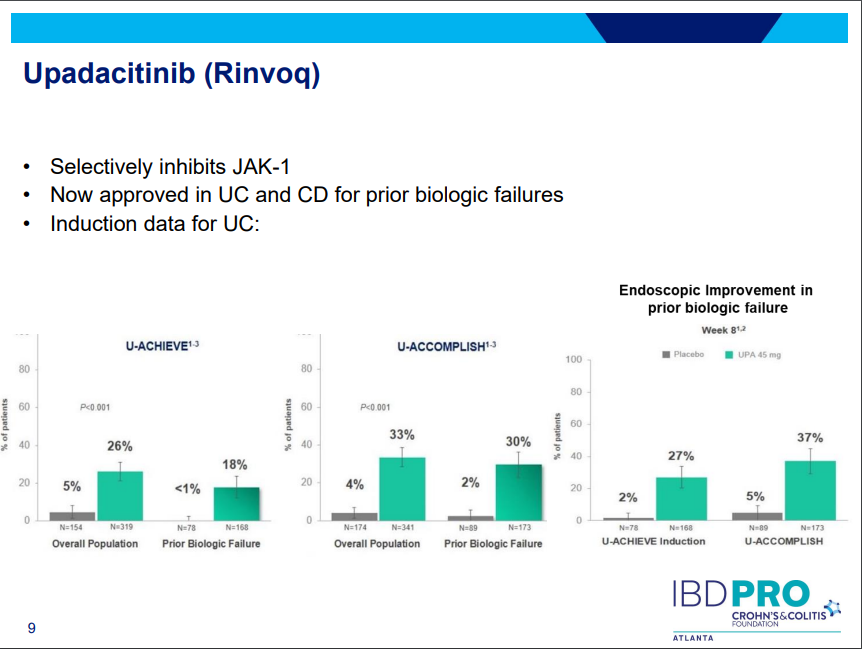
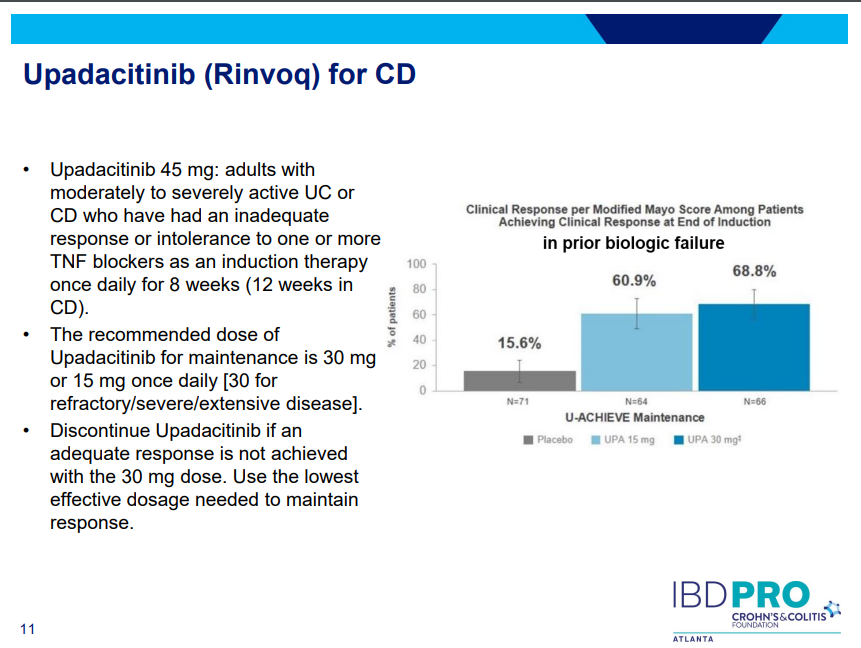
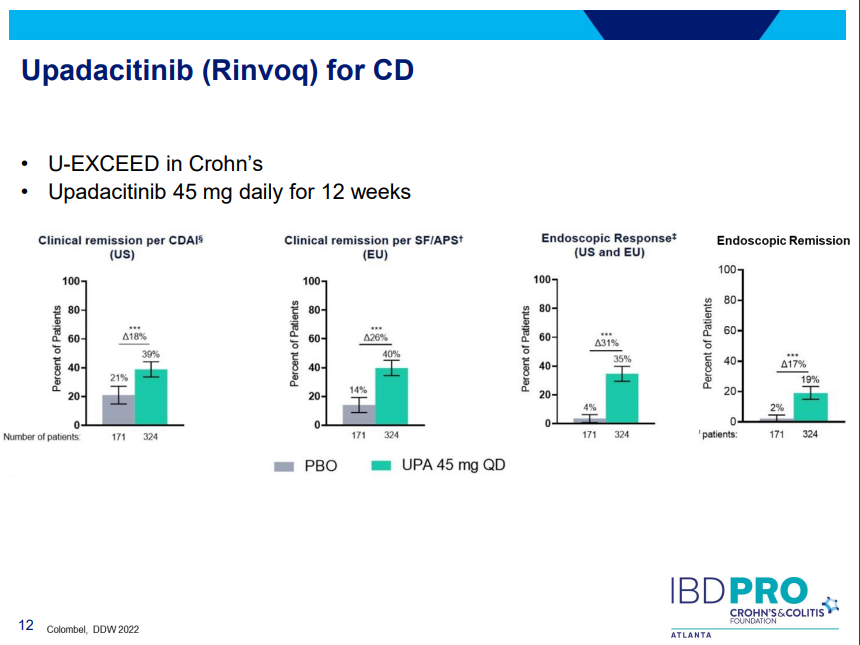
Upadacitinib (Rinvoq) -now approved for CD and UC. Higher dosing could affect liver function (especially if underlying liver disease). Also, JAK inhibitors as a class have similar safety concerns: increased herpes zoster and concerns for cardiovascular concerns (esp if >50 years)..
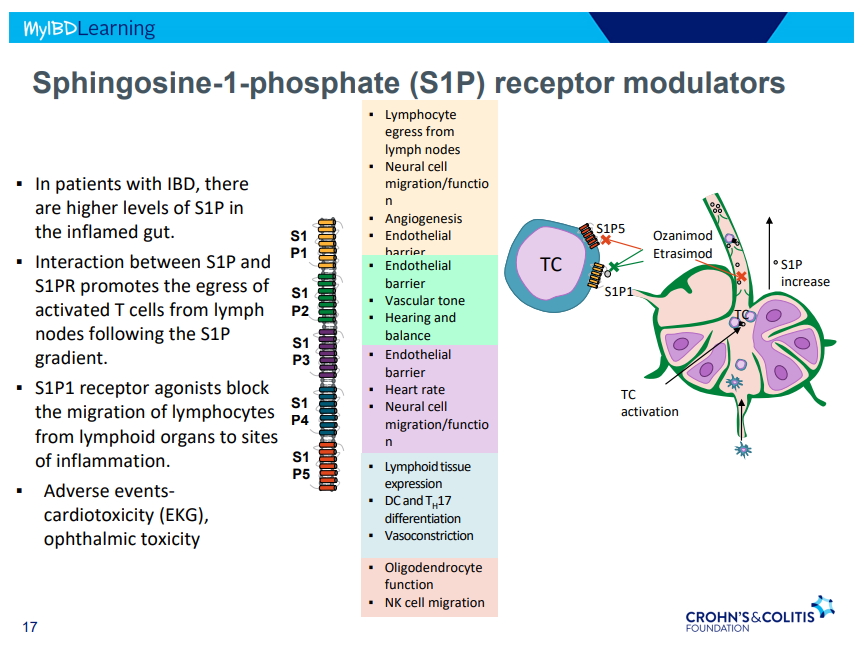
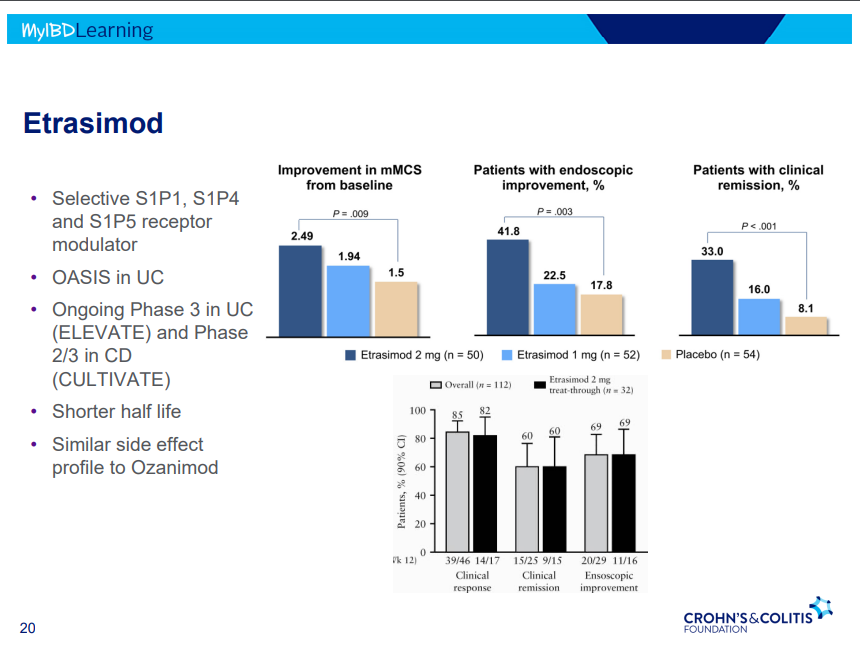
S!P receptor modulators: Oznaimod, Etrasimod & Amiselimod. Can cause bradycardia -have to check EKG prior.
In this study with 39,734 commercially-insured initiators of IBD medications (18-64 year old), 34% had a colonoscopy by 12 months and 42% at 15 months. The authors state that “it is evident that patients without any colonoscopy during this interval are not being followed under an optimal long-term T2T (treat-to-target) paradigm.”
This retrospective study examined 123 patients with Crohn’s disease and 40 with ulcerative colitis who had dose intensification with ustekinumab (to either every 4 weeks, n=91, or every 6 weeks, n=72). Dose escalation was effective in both achieving and maintaining corticosteroid-free clinical remission for 61% of patients with Crohn’s disease and 40% with ulcerative colitis at 24 months; endoscopic remission was noted in 43% with Crohn’s disease and 55% with ulcerative colitis.
Using data from multiple studies with 1157 patients, only 9 tofacitinib patients developed Clostridioides difficile infection (CDI) which was lower than the placebo group. CDI were all mild–moderate in severity and resolved with treatment in 8 patients. Six of 9 patients continued tofacitinib treatment without interruption. The low rate of infection was likely in part due to screening for CDI prior to treatment. In addition, “it is possible than the lower rates of CDI …may be due to better-controlled disease…, thus reducing susceptibility to infection.”
One clinical pearl in the discussion: “When considering treatment [for CDI], initial therapy with oral vancomycin should be considered instead of metronidazole, and treating for at least 21 days should also be considered [in patients with IBD due to]…lower rates of CDI recurrence.”
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
In this prospective study (n=198), the authors examined lipid profile changes at week 10 in patients starting IBD medications: corticosteroids, thiopurines, methotrexate, anti-TNF-α agents, vedolizumab, ustekinumab, and tofacitinib.
Key findings:
Relative increases in total cholesterol, HDL-c, and LDL-c were significant after prednisone (+26%, +31%, +12%) and tofacitinib therapy (+20%, +25%, +26%), respectively
No changes were observed in other drug classes
Findings did not correlate with calprotectin or CRP values, likely indicating a direct medication effect
My take: Recent studies have provided some reassurance regarding tofacitinib and the risk of major adverse cardiovascular events (MACEs) (see posts below). Nevertheless, it seems prudent to monitor lipids in patients receiving JAK inhibitors.
The Oro Valley/Tucson Loop shared use bike path extends over 130 car free miles throughout unincorporated Pima County, Marana, Oro Valley, and Tucson. We managed a 40 mile bike trip.