A recent study (MT Dolinger et al. Inflamm Bowel Dis 2021; 27: 1210-1214) and the associated editorial (D Geem, S Kugathasan. Inflamm Bowel Dis 2021; 27: 1361-1362) describe the use of multiple therapies (biologics and small molecule therapy) to target refractory pediatric inflammatory bowel disease. Since the term “combination therapy” is already in broad use for those receiving a biologic agent and an immunomodulator, I plan to refer to these new combinations as ‘dual immunotherapy’ for IBD.
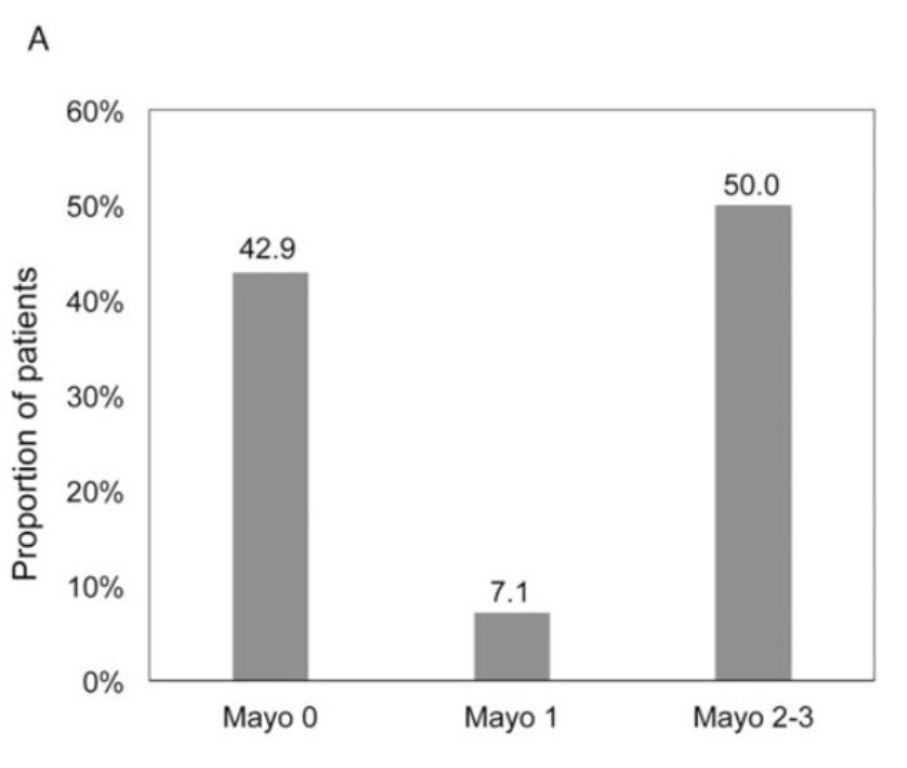
Dolinger et al (Dual Biologic and Small Molecule Therapy for the Treatment of Refractory Pediatric Inflammatory Bowel Disease) described 16 children with dual immunotherapy. Nine (56%) were treated with vedolizumab/tofacitinib, 4 (25%) with ustekinumab/vedolizumab, and 3 (19%) with ustekinumab/tofacitinib. Twelve (75%; 7 ulcerative colitis/IBD-unspecified, 5 Crohn’s disease ) achieved steroid-free remission at 6 months. One patient on 30 mg of vedolizumab/tofacitinib and prednisone daily developed septic arthritis and a deep vein thrombosis.
In the editorial (It Takes Two to Make It Right: Dual Biologic and Small Molecule Therapy for Treatment-Refractory Pediatric Inflammatory Bowel Disease), Geem et al make a number of key points:
- Except for “anti-TNF medications (infliximab and adalimumab), no other biologic therapies are FDA-approved for children with IBD”
- “Clinical disease remission is achieved in only 40-60% of patients on anti-TNF medications”
- With ustekinumab, “limited pediatric data reveal that in patients who have failed at least 1 biologic therapy, 38.6-58% achieve clinical remission by week 52…[And] vedolizumab …demonstrated steroid-free remission in 20% by week 22 in a single-center prospective observational cohort study.”
- The response to dual immunotherapy is most likely due to the synergistic effects of two medications rather than the start of a new medication. The authors note a prior study which showed a positive experience of adding ustekinumab in 5 children who developed severe paradoxical psoriasis with infliximab and in another subset of pediatric patients, there was improvement with combination vedolizumab/infliximab (Paediatr Drugs 2020; 22: 409-416)
My take (borrowed from editorial): “Given the phenotypic heterogeneity of pediatric IBD and the multiple inflammatory immune pathways implicated in its pathogenesis, the approach of biologic monotherapy–may not be suitable for all patients…patients may require specific combinations…to quell multiple arms of their dysregulated immune response.” More trials are needed to determine the safety of these regimens (especially with regard to malignancy and infections).