I am a pediatric gastroenterologist at GI Care for Kids (previously called CCDHC) in Atlanta, Georgia. The goal of my blog is to share some of my reading in my field more broadly. In addition, I wanted to provide my voice to a wide range of topics that often have inaccurate or incomplete information.
Before starting this blog in 2011, I would tear out articles from journals and/or keep notes in a palm pilot. This blog helps provide an updated source of information that is easy to access and search, along with links to useful multimedia sources.
I was born and raised in Chattanooga. After graduating from the University of Virginia, I attended Baylor College of Medicine. I completed residency and fellowship training at the University of Cincinnati at the Children’s Hospital Medical Center. I received funding from the National Institutes of Health for molecular biology research of the gastrointestinal tract.
During my fellowship, I had the opportunity to work with some of the most amazing pediatric gastroenterologists and mentors. Some of these individuals included Mitchell Cohen, William Balistreri, James Heubi, Jorge Bezerra, Colin Rudolph, John Bucuvalas, and Michael Farrell. I am grateful for their teaching and their friendship. During my training with their help, I received a nationwide award for the best research by a GI fellow.
I have authored numerous publications/presentations including original research, case reports, review articles, and textbook chapters on various pediatric gastrointestinal problems. In addition, I have been recognized by Atlanta Magazine as a "Top Doctor" in my field multiple times.
Currently, I am the vice chair of the section of nutrition for the Georgia Chapter of the American Academy of Pediatrics. In addition, I am an adjunct Associate Clinical Professor of Pediatrics at Emory University School of Medicine. Other society memberships have included the North American Society for Pediatric Gastroenterology Hepatology and Nutrition (NASPGHAN), American Academy of Pediatrics, the Food Allergy Network, the American Gastroenterology Association, the American Association for the Study of Liver Diseases, and the Crohn’s and Colitis Foundation.
As part of a national pediatric GI organization called NASPGHAN (and its affiliated website GIKids), I have helped develop educational materials on a wide-range of gastrointestinal and liver diseases which are used across the country. Also, I have been an invited speaker for national campaigns to improve the evaluation and treatment of gastroesophageal reflux disease, celiac disease, eosinophilic esophagitis, hepatitis C, and inflammatory bowel disease (IBD). Some information on these topics has been posted at my work website, www.gicareforkids.com, which has links to multiple other useful resources.
I am fortunate to work at GI Care For Kids. Our group has 17 terrific physicians with a wide range of subspecialization, including liver diseases, feeding disorders, eosinophilic diseases, inflammatory bowel disease, cystic fibrosis, DiGeorge/22q, celiac disease, and motility disorders. Many of our physicians are recognized nationally for their achievements. Our group of physicians have worked closely together for many years. None of the physicians in our group have ever left to join other groups. I have also worked with the same nurse (Bernadette) since I moved to Atlanta in 1997.
For many families, more practical matters about our office include the following:
– 14 office/satellite locations
– physicians who speak Spanish
– cutting edge research
– on-site nutritionists
– on-site psychology support for abdominal pain and feeding disorders
– participation in ImproveCareNow to better the outcomes for children with inflammatory bowel disease
– office endoscopy suite (lower costs and easier scheduling)
– office infusion center (lower costs and easier for families)
– easy access to nursing advice (each physician has at least one nurse)
I am married and have two sons (both adults). I like to read, walk/hike, bike, swim, and play tennis with my free time.
I do not have any financial relationships with pharmaceutical companies or other financial relationships to disclose. I have helped enroll patients in industry-sponsored research studies.
My take: While the prices are very good, I know some have had trouble working with the online pharmacy to get their prescriptions filled in a timely manner.
“Science suggests that chores make kids happy and that you should start assigning little jobs early, even when they are toddlers.”
“Seemingly insignificant chores like setting the table or folding laundry are valuable building blocks toward a child’s independence.”
NY Times (11/1/22): How Brains Send a Signal That It’s Time to Vomit (in mice) Reference article: Z Xie et al. Cell: The gut-to-brain axis for toxin-induced defensive responses “They traced the effect to certain neurons in the brain that released neurotransmitters when the drug [eg. chemotherapy] or the toxin [eg. bacterial] reached the gut. Following those messages back, they discovered cells in the small intestine that reacted to the presence of these noxious substances. A central player in the pathway to nausea and retching was an immune system molecule called interleukin 33, or IL33. Keeping mice from making IL33 significantly reduced their symptoms.”
S Sen. NEJM 2022; 387: 1629-1630. Is It Burnout or Depression? Expanding Efforts to Improve Physician Well-Being
Key points:
“This growing attention has helped to reduce the stigma associated with burnout, highlighting the health care system, rather than the individual, as the primary driver of the problem.”
What is burnout? “One review identified 142 different definitions of physician burnout in 182 studies.3 …the most commonly used is the Maslach Burnout Inventory, which assesses continuous scores for three domains: emotional exhaustion, depersonalization, and reduced sense of personal accomplishment.”
There is a lot of overlap with depression especially with emotional exhaustion. However, depression is still stigmatized as due to individual weakness. “Work-related stress is the primary driver of depression among physicians. A stark illustration of this dynamic is the fact that the prevalence of depression among training physicians before they enter residency is similar to that among young adults in the general population, but depression rates quintuple immediately after residency begins.”
“Whether burnout is meaningfully distinguishable from depression, the argument that depression and burnout are caused by fundamentally different precipitants is unsupported by the evidence to date”
My take (borrowed from the author): “Crucially, identification and treatment of depression can help reduce the risk of suicide among physicians. Unfortunately, when we encourage clinicians to consider themselves burned out rather than depressed, they tend not to seek or receive the individual-level interventions that can improve well-being.”
Three most common causes of infectious esophagitis in children: Candida, HSV and CMV. Asperigillus (& other fungi) as well as bacterial esophagitis are rarely seen. Rare viral infections include human papilloma, varicella zoster and EBV
For Candida, this is typically a benign commensal organism but can become pathogenic due to changes in immunity (immunocompromised including corticosteroids), altered motility and sometimes after antibiotics (with or without PPI therapy). EoE can present with similar-appearing mucosa; thus, biopsy and/or brushing is needed.
With HSV, pediatric case series have reported higher rates in immunocompetent children
Typical treatments: fluconazole for Candida, and Acyclovir for HSV. For CMV, potential treatments include ganciclovir, valganciclovir, foscarnet or cidofovir.
My take: This is a short, good review of the infections that can cause esophagitis in children.
Compared with WD1 (typical Western Diet), PB2 (Plant-based diet 2) was associated with lower odds of active symptoms for CD (odds ratio [OR], 0.32
PB1 (Plant-based diet 1) was associated with lower odds of active symptoms for participants with UC (OR, 0.45; 95% CI, 0.23-0.90) but not for participants with CD (OR, 0.95
Diet PB1 (“Plant-based Diet 1”) was characterized by much higher intake of fruits, vegetables, plant-based proteins, and cooked grains than most other dietary clusters. There was low water intake in favor of juices and other beverages. There was otherwise average intake of added fats and oils, sugars, seafood, and dairy products, and modest intake of meats, eggs, mixed grains, and breads.
Diet PB2 (“Plant-based Diet 2”) was characterized by high intake of fruits, vegetables, plant proteins, and cooked grains and low intake of animal proteins (especially red and cured meats), added fats, sweetened beverages, sweet bakery products, other desserts, eggs, and breads. There was also a reduction of other beverages in favor of water. There was otherwise an average intake of seafood and dairy products.
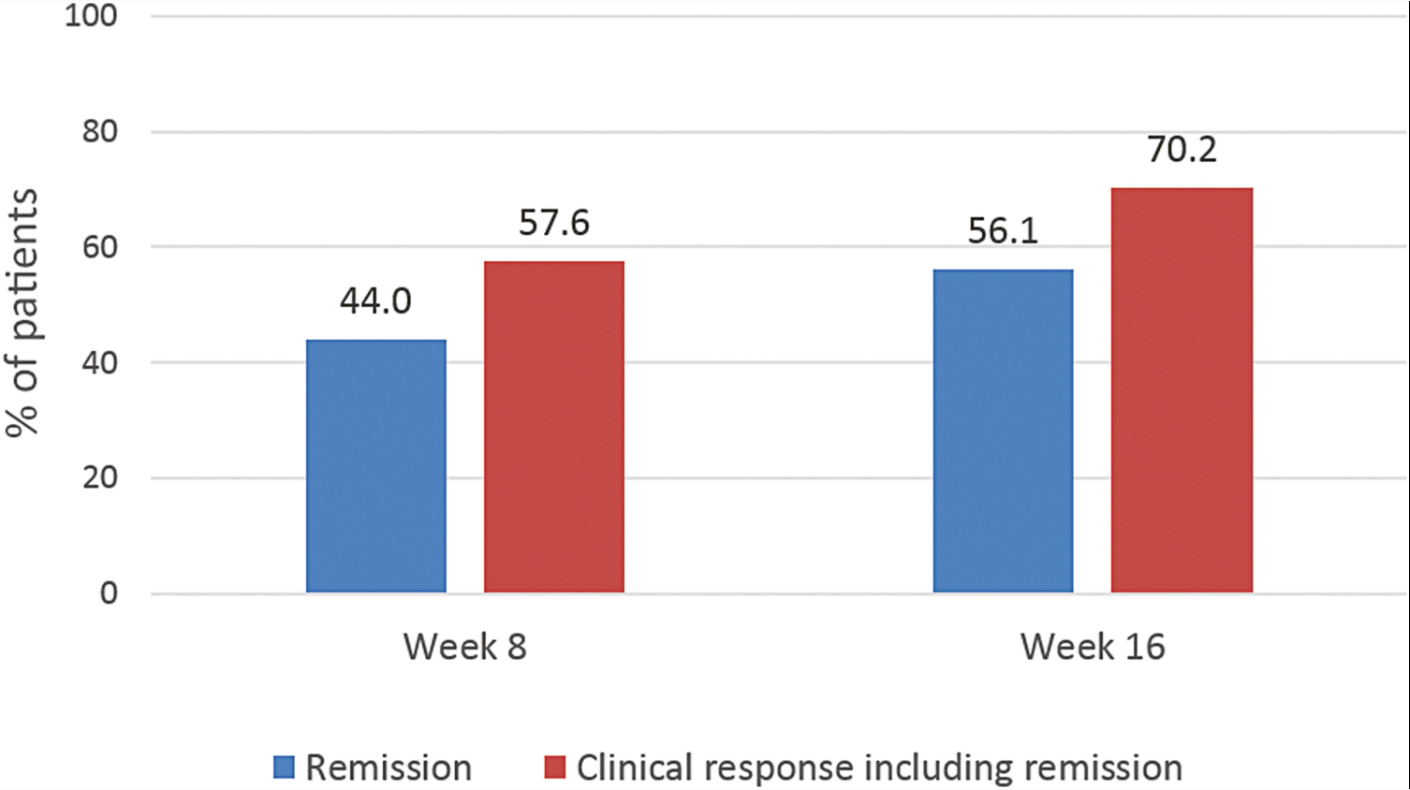
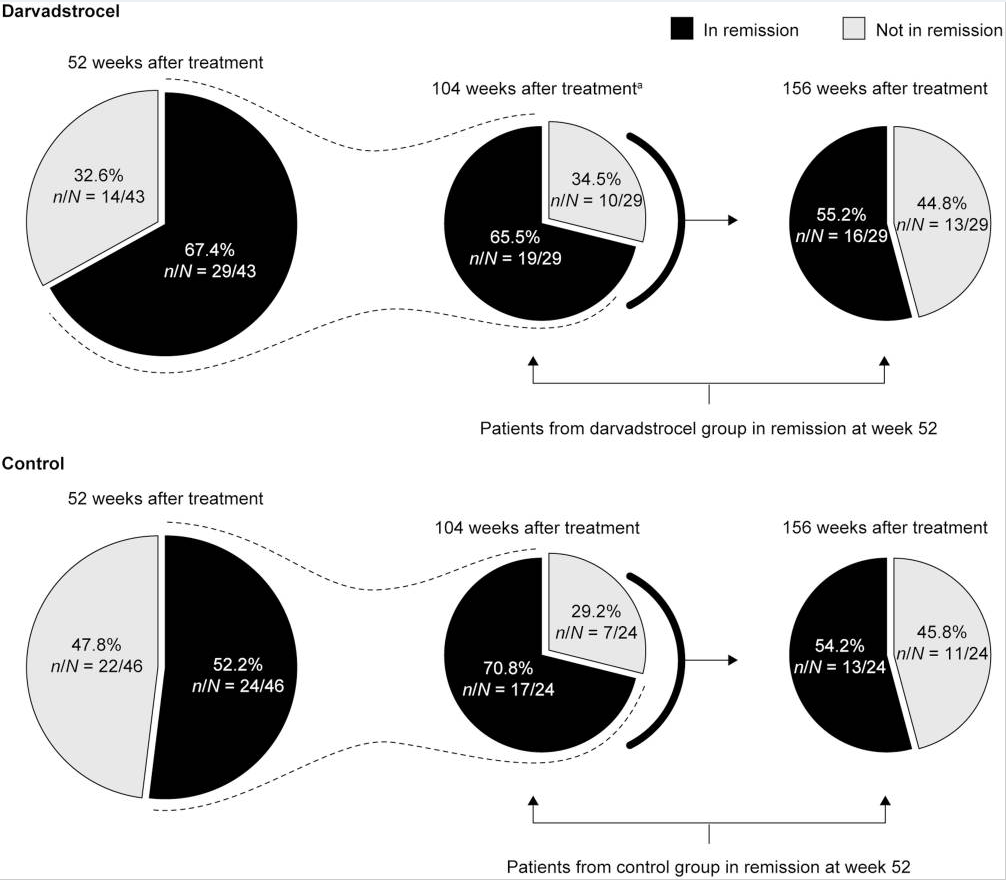
Background: The current chart review study evaluated the longer-term effectiveness and safety of darvadstrocel (expanded allogeneic adipose-derived mesenchymal stem cells).; n=43 treated patient and n=46 controls.
Key findings:
At 52, 104, and 156 weeks posttreatment, clinical remission was observed in 29 (67.4%) of 43, 23 (53.5%) of 43, and 23 (53.5%) of 43 darvadstrocel-treated patients, compared with 24 (52.2%) of 46, 20 (43.5%) of 46, and 21 (45.7%) of 46 control subjects, respectively.
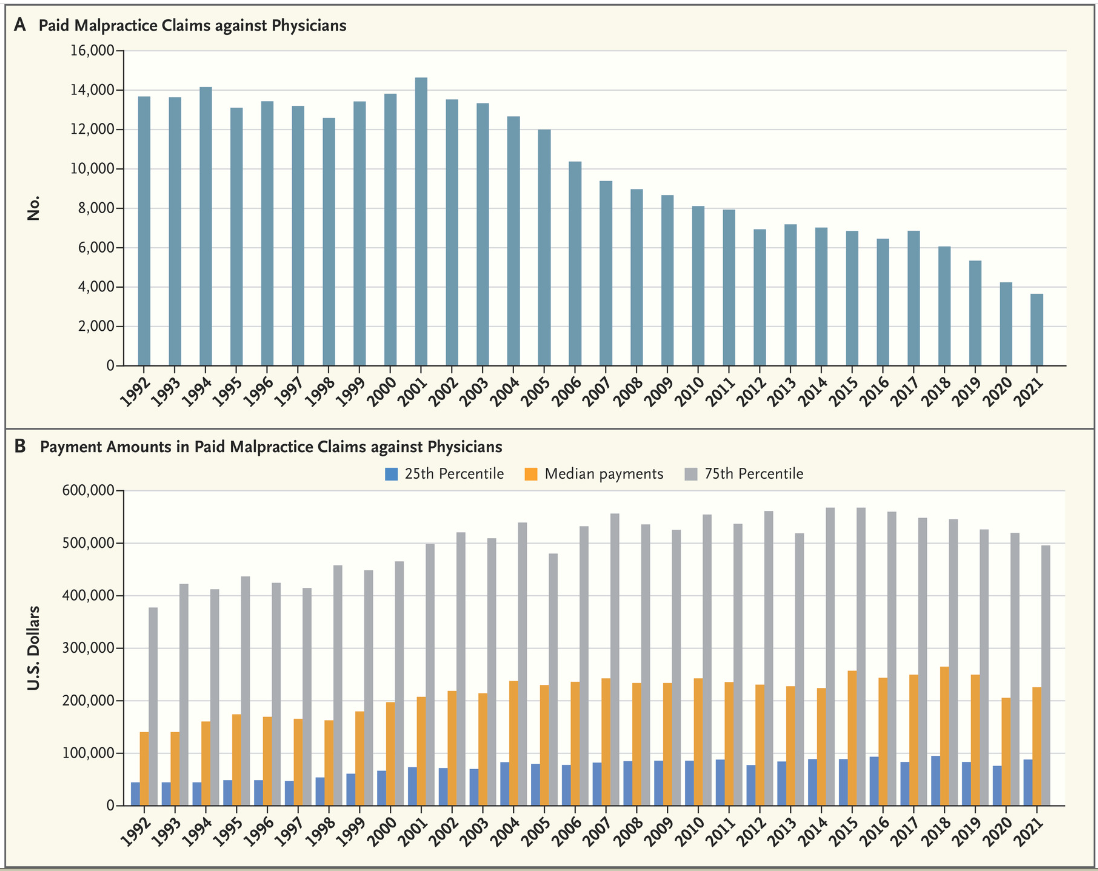
DM Studdert, MA Hall. NEJM 2022; 387: 1533-1537. Medical Malpractice Law — Doctrine and Dynamic
This article reviews the topic of malpractice and the hurdles for plaintiffs to establish liability. Some of the interesting points:
“Patients lose about 80% of medical malpractice trials.3 However, fewer than 1 in 20 claims end in courtroom verdicts; about one third are settled out of court with a payment to the patient, and the remainder are dropped or dismissed.3“
“NPDB data reveal a remarkable phenomenon: the number of paid claims against physicians has decreased by 75% in the past 20 years.” The potential reasons include tort reform, greater openness about medical errors may have reduced patients’ inclination to sue, better medical care (no evidence of this), and incomplete NPDB data. With regard to incomplete data, this can occur with “corporate shielding” in which institutions assume liability and payment responsibility in claims against physicians, thus averting reporting requirements).
A widely covered news story in October 2022 was the disappointing results/modest benefits of a colonoscopy screening study. This study actually supports the use of colonoscopy to reduce colorectal cancer deaths but shows that typical screening programs may not work well if patients don’t show up for the test.
Methods: This was “a pragmatic, randomized trial involving presumptively healthy men and women 55 to 64 years of age drawn from population registries in Poland, Norway, Sweden, and the Netherlands between 2009 and 2014. The participants were randomly assigned in a 1:2 ratio either to receive an invitation to undergo a single screening colonoscopy (the invited group) or to receive no invitation or screening (the usual-care group).”
There were 84,585 participants in Poland, Norway, and Sweden — 28,220 in the invited group,
Key findings:
Only 11,843 (42.0%) in the invited group underwent colonoscopy screening
During a median follow-up of 10 years, 259 cases of colorectal cancer were diagnosed in the invited group as compared with 622 cases in the usual-care group
The risk of colorectal cancer at 10 years was 0.98% in the invited group and 1.20% in the usual-care group, a risk reduction of 18%
The risk of death from colorectal cancer was 0.28% in the invited group and 0.31% in the usual-care group (risk ratio, 0.90; 95% CI, 0.64 to 1.16)
The risk of death from any cause was 11.03% in the invited group and 11.04% in the usual-care group
If all invited participants had received a colonoscopy, the authors estimate the risk of colorectal cancer would have decreased from 1.22% to 0.84% and the risk of colorectal cancer death would have been reduced from 0.3% to 0.15% (a 50% drop).
My take: Colonoscopy as a screening tool only works if it is performed. Given the low response rate for screening, other tools like an annual fecal immunochemical test (FIT) need to be considered as alternatives.
In this single-center retrospective study with 19 patients, MMP-7 and GGT values were compared in children who were diagnosed with Parenteral Nutrition-Associated Liver Disease (PNALD, n=15) and Biliary atresia (n=4). Key findings:
Median MMP-7 values for PNALD patients 37.8 ng/mL was much lower than MMP-7 values for biliary atresia 112.3 ng/mL.
GGT values were not statistically significantly different 116 for PNALD vs 248 for biliary atresia
In this cohort, a MMP-7 threshold of 52.8 ng/mL had a sensitivity of 100% and specificity of 93.5% for biliary atresia.
My take: MMP-7 values reduce diagnostic uncertainty between PNALD and biliary atresia. However, there are infrequent cases of biliary atresia with lower values of MMP-7.
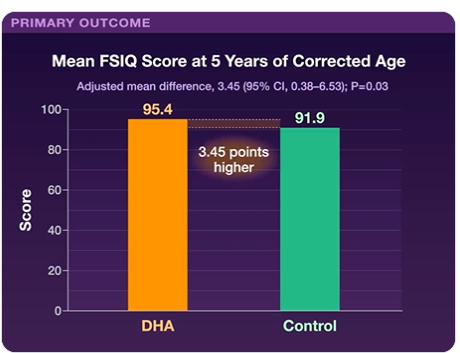
JF Gould et al. NEJM 2022; 387: 1579-1588. Neonatal Docosahexaenoic Acid in Preterm Infants and Intelligence at 5 Years
Background: “Because its accretion into the brain is greatest during the final trimester of pregnancy, infants born before 29 weeks’ gestation do not receive the normal supply of DHA.”
In this randomized placebo-controlled study of infants born prior to 29 weeks gestation, DHA supplementation 60 mg/kg/day was given to the study group and cognitive outcomes were measured at 5 yrs. 480 (73%) had an full-scale intelligence quotient (FSIQ) score available — 241 in the DHA group and 239 in the control group.
Key findings: FSIQ scores were 95.4±17.3 in the DHA group and 91.9±19.1 in the control group. Adverse events were similar in the two groups.