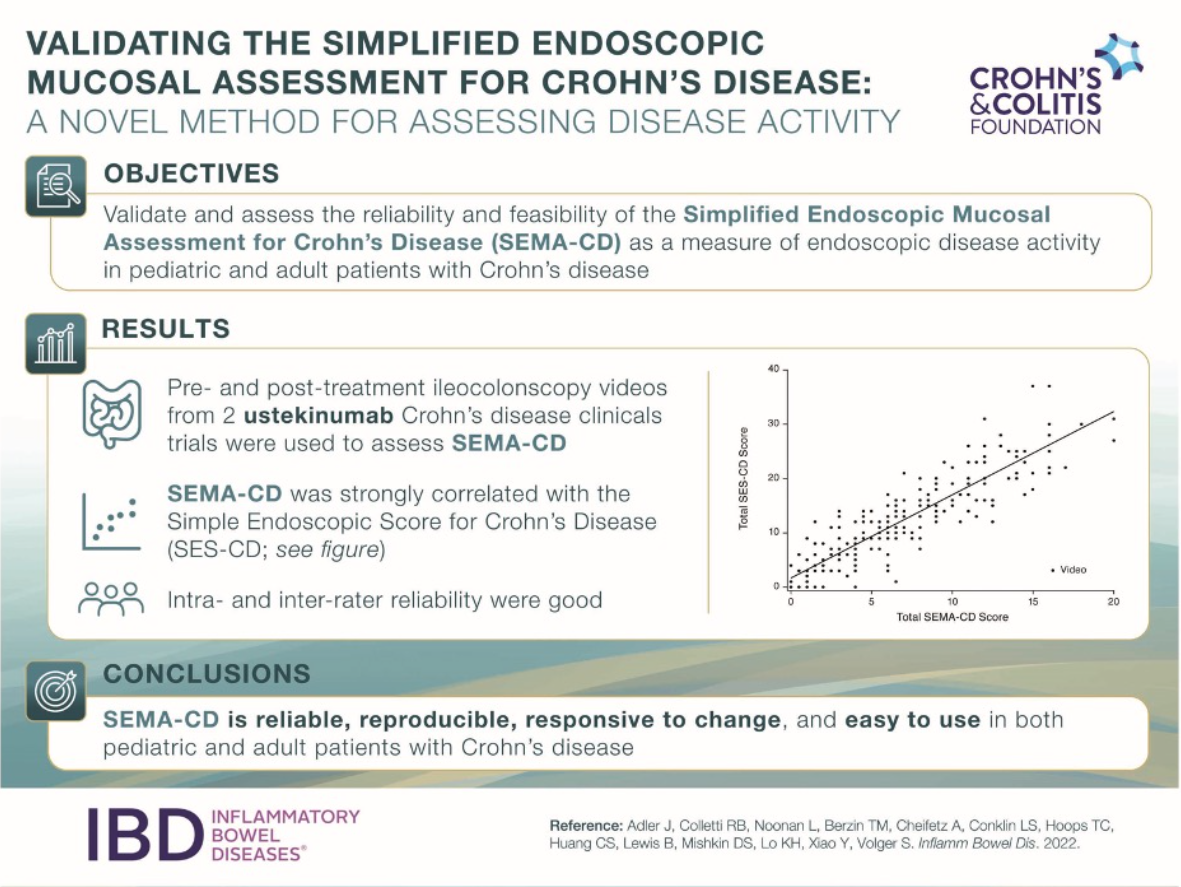
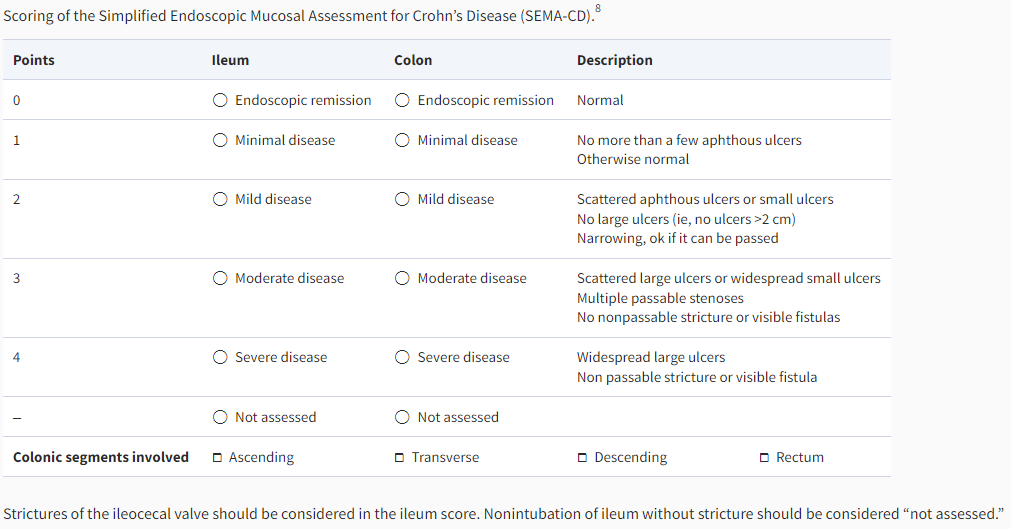
“The SEMA-CD is scored by assigning a numerical value ranging from 0 (endoscopic remission) to 4 (severe disease) for each bowel region (ileum and colon). The overall colon is scored as a whole based on the most severe colonic segment. The number of colonic segments with any degree of active disease is recorded, regardless of the severity of individual segments. The overall colon score is then multiplied by the number of involved colonic segments, and the result is added to the ileum score.”
4 patients with Crohn’s disease had loss of response.
9% of patients were switched back to IV vedolizumab due to adverse events or fear of needles.
Median clinical and biochemical disease activity remained stable after the switch. Median vedolizumab serum concentrations increased from 19 μg/ml at the time of the switch to 31 μg/ml 12 weeks after the switch (p < 0.005).
HC Kaplan et al. Am J Gastroenterol 2022 Jun 1;117(6):902-917. Open access: Personalized Research on Diet in Ulcerative Colitis and Crohn’s Disease: A Series of N-of-1 Diet Trials. In this study, 21 patients (completed trial) were randomized to 1 of 2 sequences of 4 alternating 8-week SCD (specific carbohydrate diet) and MSCD (modified specific carbohydrate diet) periods.
Key findings: “SCD and MSCD did not consistently improve symptoms or inflammation.” “Some individuals had improvement in symptoms and fecal calprotectin compared with their UD, whereas others did not.” The authors note that it took 18 months to recruit 54 patients for this study across 19 research sites.
Black adult patients were significantly less likely than White patients to have a diagnosis of CD (odds ratio [OR], 0.53) or UC (OR, 0.41). Pediatric Black patients were also less likely to have a diagnosis of CD (OR, 0.41) or UC (OR, 0.38)
Adult Hispanic patients were less likely to have a diagnosis of CD (OR, 0.33) or UC (OR, 0.45) compared with non-Hispanic patients. Similarly, pediatric Hispanic patients were less likely to have a diagnosis of CD (OR, 0.34) or UC (OR, 0.50).
Thus, these data suggest that CD and UC are modestly less prevalent among patients of non-White races and Hispanic ethnicity
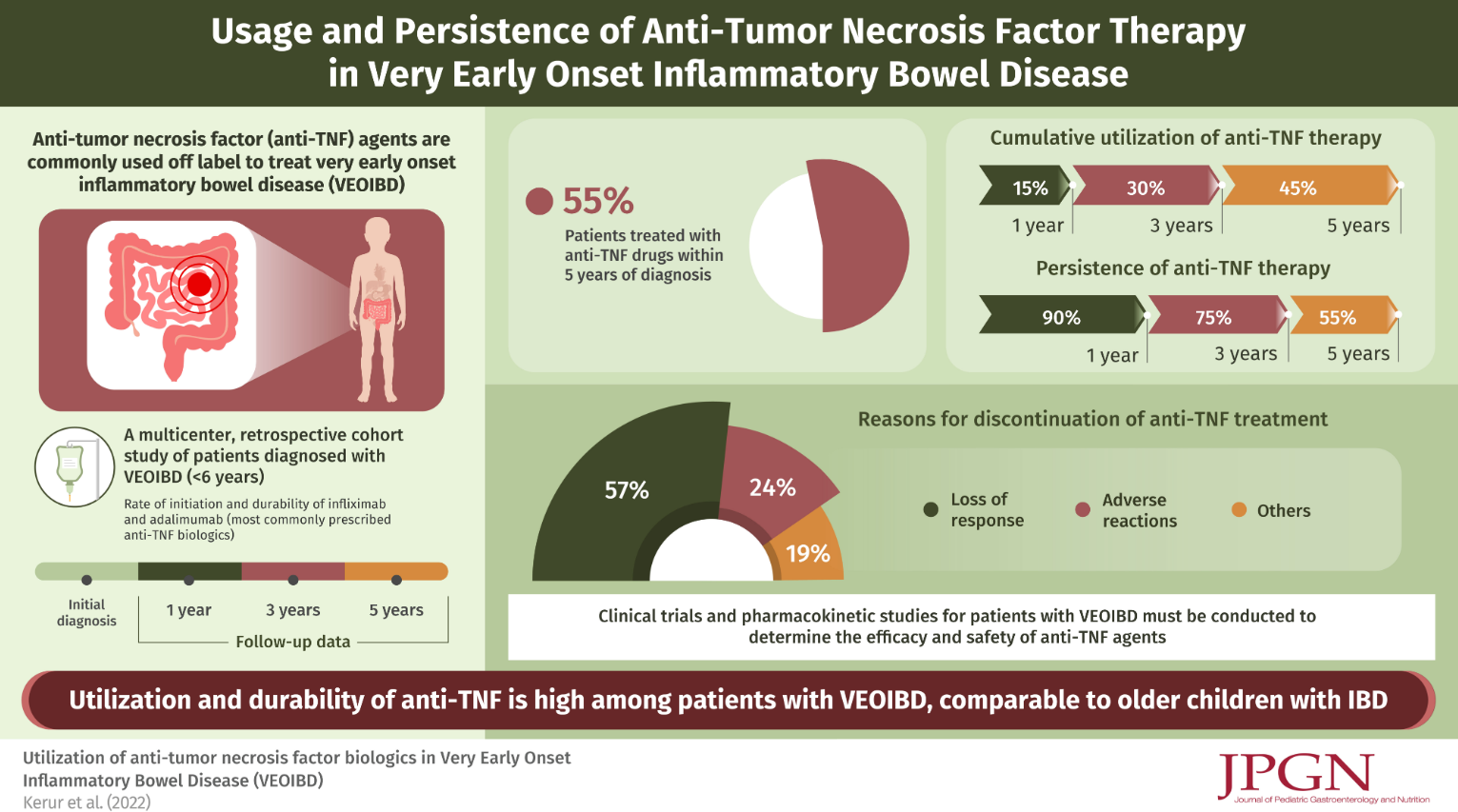
In this retrospective study, 120 of 294 children with VEO-IBD (diagnosed 2008 and 2013, PRO-KIDS network) received anti-TNF therapy (96% infliximab). 101 of these 120 had adequate data recorded. It is noted that additional data on this cohort has been previously published (IBD Updates: Outcomes of VEO-IBD, PIANO Study Update, and Insurance-Disparity Relationship). Key findings:
Anti-TNF durability was 90% at 1 year, 75% at 3 years, and 55% at 5 years
Patients with Crohn’s disease had better durability than those with UC/IBD-U (Hazard ratio 0.17)
The most common reason for discontinuation of anti-TNF were loss of response in 24 (57%) children
67 (66%) received combined therapy with an immunomodulator and this was associated with improved anti-TNF durability (Hazard ratio 0.30). However, authors note this was in era preceding widespread therapeutic drug monitoring.
The majority of children in the current study did not undergo testing for monogenic mutations
My take: Data for use of anti-TNF agents in this age group (< 6 yrs) has been limited. This study suggests similar effectiveness of anti-TNF agents in VEO-IBD compared to older groups. Given this groups increased risk for monogenic mutations, it is still a good idea, if feasible, to test for these disorders.
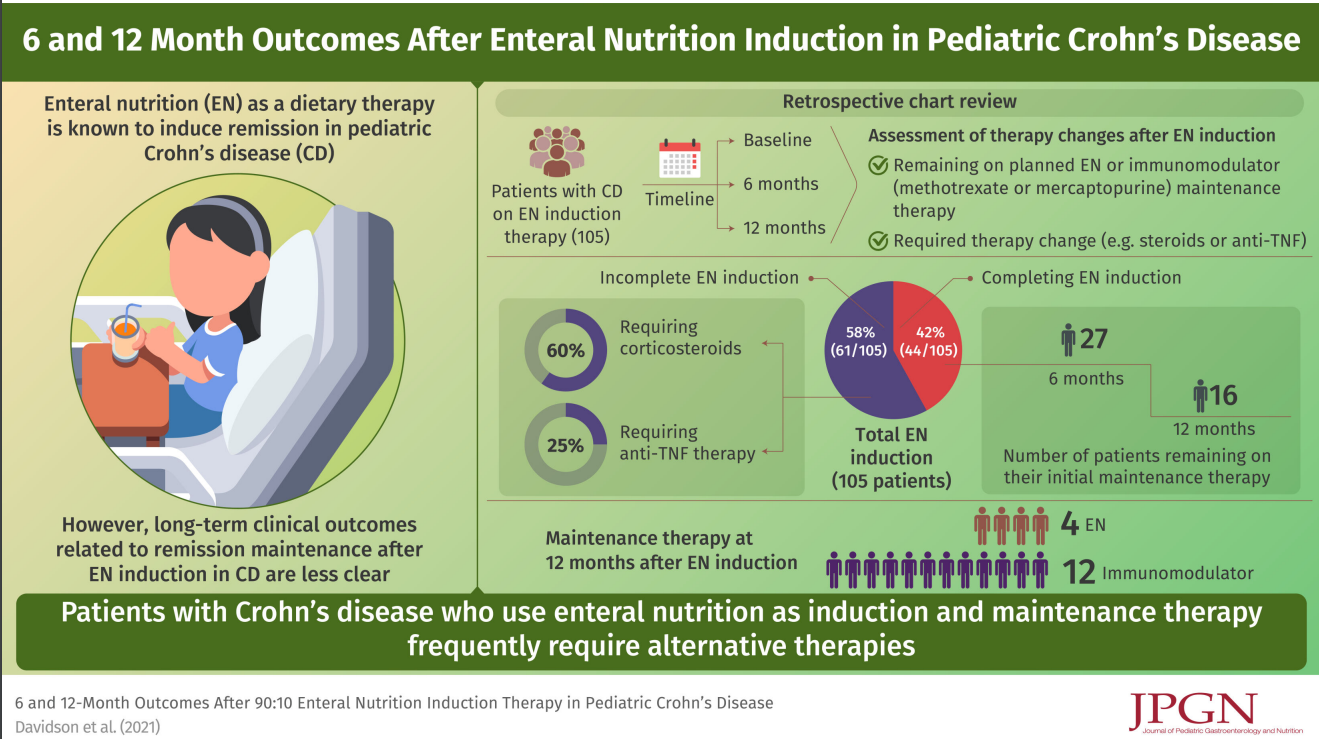
In this retrospective study (2013-2018), the authors examined outcomes in 105 children treated with a 90:10 enteral feeds (90% formula).
Key findings:
44/105 (42%) patients completed 8–12 weeks
After induction, 18 continued EN maintenance with a 80:20 then 70:30 protocol; however, only 10 remained on EN at 6 months and 4 remained on EN at 12 months
The associated editorial (pg: 1-2) make several points:
While EEN is effective and safe, this study and others have shown poor adherence
It is unclear how exclusive enteral nutrition needs to be in order to be effective. And, many patients instructed to receive 90% of their calories as formula are likely consuming higher amounts of table foods
We still are working out which foods need to be excluded
My take: This study shows that EEN is NOT a practical option for most patients beyond induction. Only 4 patients remained on EEN at 12 months.
The expression ‘90% of Success is Showing Up’ has been attributed to Woody Allen. With dietary and medical treatments, adherence is the equivalent of showing up.
In this study, the authors measured fecal gluten immunogenic peptides (GIP), a biomarker of gluten intake, in 45 children (3– 17 years) with Crohn’s disease to assess adherence to enteral nutrition. This, in turn, was correlated with fecal calprotectin (FC) levels.
Key findings:
FC decreased in patients with undetectable GIP at both 33 and 54 days of EEN (mean decrease, 33 days: −743 mg/kg, 54 days: –1043 mg/kg, P< 0.001) but not in patients who had detectable GIP levels
At EEN completion, patients with undetectable GIP had a lower FC by 717 mg/kg compared with patients with a positive GIP result (P = 0.042) and demonstrated a greater decline from baseline FC (–69% vs +5%, P = 0.011)
13% and 23% had detectable GIP levels at 33 days and 54 days respectively. It is noted that GIP levels are only indicative of short-term consumption (eg. prior 1-2 days) of gluten-containing foods
My take: Dietary therapies are really difficult for most people. This study shows that those with poor compliance are unlikely to benefit.
Many times, treatment decisions are like on “Let’s Make a Deal.” That is, should I stick with what I’ve got or should I try for something better & sometimes wind up with a goat. In this referenced article, patients were under maintenance therapy with adalimumab (ADA) monotherapy (40 mg every 14 days) and had experienced a secondary loss of response (LOR) despite trough levels > 4.9 μg/mL. In this nonrandomized prospective study, patients were either swapped to vedolizumab (VDZ) or optimized on adalimumab (ADA) treatment.
Key findings:
At 24 months, 11 out of 70 patients (16%) in the swap group discontinued treatment compared with 36 out of 61 (59%) patients in the optimization group (P < 0.001)
In the optimization group, treatment discontinuation was positively associated with baseline fecal calprotectin >500 μg/g (HR, 3.5)
In patients selected for optimization, 56% (34/61) remained on ADA at 1 year and 41% (25/61) at 2 years
In their discussion, the authors state “current guidelines recommend switching to another class of biologics in case of LOR to ADA with therapeutic drug levels.” However, the authors note that their therapeutic level cut-off of >4.9 mcg/mL is lower than the latest recommendations. In addition, in their conclusion, they note that due to limited biologic options, “ADA optimization strategy might be considered” in a subgroup.
My take: Despite better results in the patients that swapped to VDZ in this study, I think it is important to assure adequate drug levels before choosing a new drug class. For ADA, expert recommendations have suggested a level of 8-12 as therapeutic and to avoid discontinuation if ADA level is less than 10. In this study, more than 40% remained on ADA two years after LOR in those with dosing optimization.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
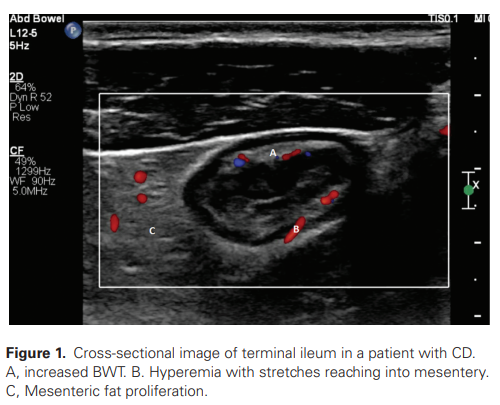
Research has shown that IUS has the potential to be a valuable additional point-of-care tool to guide treatment choice and to monitor and predict treatment response, although evidence of its accuracy and value in clinical practice is still limited
The utility may be operator-dependent as well
My take: Due to low upfront costs, IUS would be appealing adjunct to current monitoring. However, one could envision IUS leading to more downstream studies (& costs), especially if its sensitivity and specificity are not very high.
In this internet-based cohort of 9-17 yr olds (n=159, 96% white), the authors found no association between baseline PROMIS Pediatric anxiety score and subsequent sCDAI (change in sCDAI for 3-point change in PROMIS Pediatric −0.89; 95% CI −4.81 to 3.03). This study is in contrast to studies in adults which have shown a bidirectional relationship between anxiety/depression and IBD activity.
My take: It is difficult to know with certainty whether anxiety/depression may trigger IBD activity; more studies are needed. Treatment of mental health is important regardless of its effects on IBD activity.
An excerpt: “The Crohn’s & Colitis Foundation…launched the We Can’t Wait app, which provides an interactive map that allows users to find a restroom near them across the U.S. Driven by crowd-sourced submissions and major retail and restaurant partners that contributed their restroom location data, the app empowers IBD patients – and all users – with a tool to find restrooms more easily, both in emergency and everyday situations. The app is free and available for download now.
This is a case series of six pediatric patients and young adults who developed hypersensitivity reactions during intravenous infusion with ustekinumab (UST).
Key findings:
Hypersensitivity reactions during intravenous (IV) induction dose of UST, ranging from mild allergic reactions to anaphylaxis, with no antibodies detected in the two who had testing
Reactions occurred 0-30 minutes after start of infusion
Management was with methylprednisolone in 5 of 6 patients, diphendyramine in 3 of 6, and epinephrine in 1. One patient was managed with IV diphenhydramine alone.
Four of six continued with UST subcutaneously without reactions. ***Change of formulation of UST from IV to subcutaneous was done in a controlled hospital-based setting. The other two 33% were switched to another biologic due to physician preference and were never exposed to the subcutaneous formulation
Although the exact pathogenesis of this infusion reaction remains unknown, it has been attributed to EDTA
My take: It appears that patients with UST hypersensitivity reactions can be changed to SC formulation. The authors recommend to trial a subcutaneous dose of UST in a controlled setting; in addition, they suggest testing with skin prick testing or specific IgE levels to EDTA done by allergy and immunology.
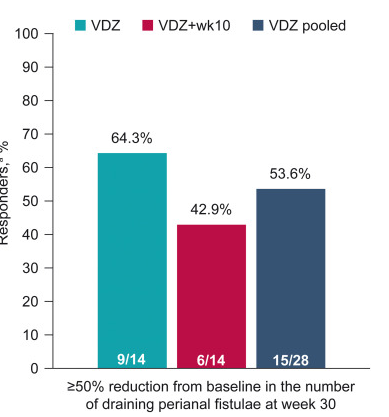
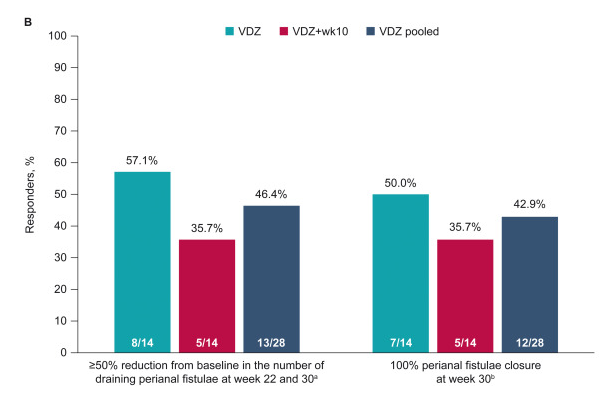
Methods: “Patients with moderately to severely active CD and 1–3 active perianal fistulae (identified on magnetic resonance imaging [MRI]) received vedolizumab 300 mg intravenously at weeks 0, 2, 6, 14, and 22 (VDZ) or the same regimen plus an additional vedolizumab dose at week 10 (VDZ + wk10)… Enrollment was stopped prematurely because of recruitment challenges”
Key findings:
“Rapid and sustained fistula closure was observed; 53.6% (VDZ, 64.3%; VDZ + wk10, 42.9%) and 42.9% (VDZ, 50.0%; VDZ + wk10, 35.7%) of patients achieved ≥50% decrease in draining fistulae and 100% fistulae closure, respectively, at week 30”
“MRI healing, defined as the disappearance of T2 hyperintensity signal and absence of gadolinium contrast enhancement,3 was not reached in this study…gadolinium contrast enhancement showed improvement at week 30…MRI studies have shown that internal fistulae healing lags behind clinical remission by a median of 12 months”
Figure 1Figure 2 B
The study findings are limited by relatively small size and lack of control group (eg. placebo or seton/antibiotic group). However, the rate of response in this study is significantly higher than placebo studies which have shown “~1 in 6” who experienced fistula closure.
My take: Vedolizumab is another option for treating Crohn’s disease with perianal fistula. Both regimens in this study were associated with response, though the additional 10-week dose (in one group) did not improve outcomes.