Yesterday’s post reviewed the landmark study leading to dupilumab’s FDA approval. Today’s case report shows that we have a lot we need to learn about its use.
The authors present a case report of a patient with eosinophilic esophagitis (EoE) who had ongoing active EoE while receiving topical steroids (TS) and PPI (and previously dietary elimination therapy). He achieved remission after the addition of dupilumab. “When his TS were weaned after achieving remission, his disease relapsed with worsening of his dysphagia and a peak eosinophilic count (PEC) of 55 eosinophils per high power field (eos/hpf). Upon restarting TS to his ongoing dupilumab, symptoms fully resolved, and he achieved histologic remission (PEC 10 eos/hpf).”
My take: This study indicates that there are some patients need dupilumab and topical steroids in combination, rather than monotherapy. Reliable biomarkers to more easily determine response and/or to predict optimal therapy are clearly needed.
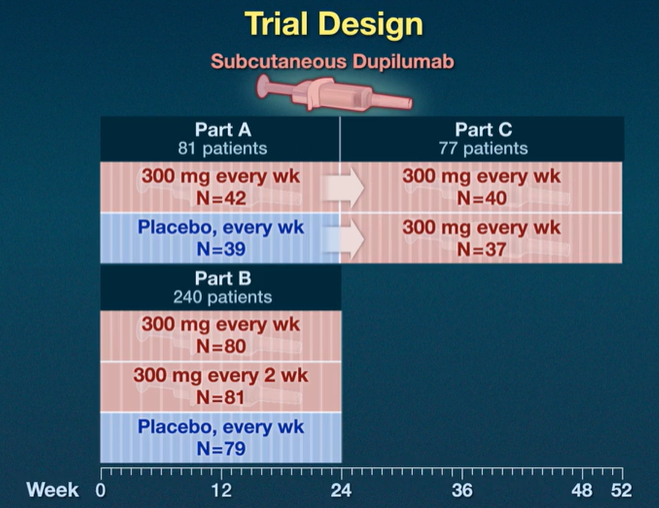
This study was pivotal for receiving FDA approval of dupilumab (dupixent) for the treatment of EoE (the only FDA approved therapy). Background: “Dupilumab, a fully human monoclonal antibody, blocks interleukin-4 and interleukin-13 signaling, which have key roles in eosinophilic esophagitis..Standard-of-care treatments for eosinophilic esophagitis include food elimination diets, proton-pump inhibitors (PPIs), swallowed topical glucocorticoids (applied to the esophagus by swallowing), and, in the case of strictures, esophageal dilation.11,12 However, the rates of response are variable (30 to 40% of patients may not have a response to first-line treatments).”
Key findings from three-part study (see images below):
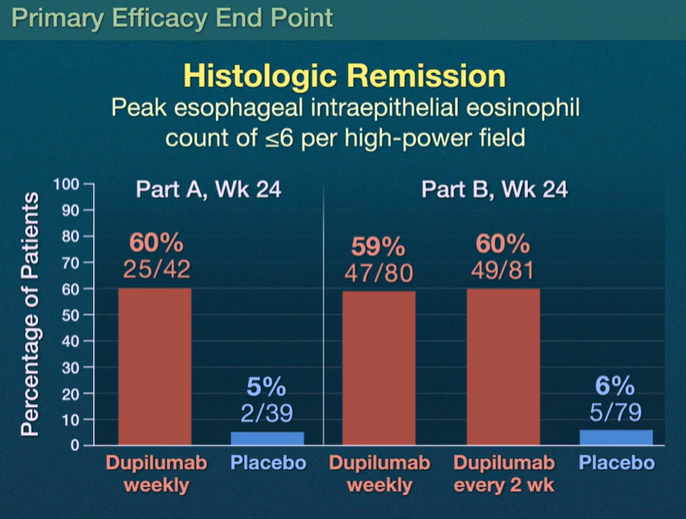
Part A: Histologic remission occurred in 25 of 42 patients (60%) who received weekly dupilumab and in 2 of 39 patients (5%) who received placebo
Part B: Histologic remission occurred in 47 of 80 patients (59%) with weekly dupilumab, in 49 of 81 patients (60%) with dupilumab every 2 weeks, and in 5 of 79 patients (6%) with placebo
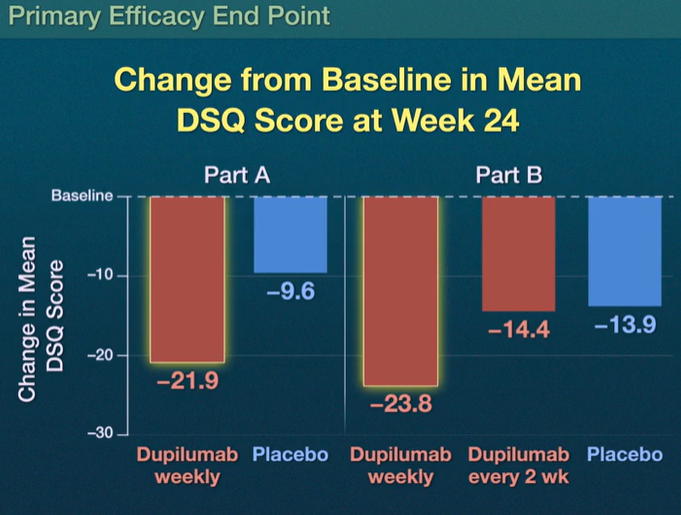
Dysphagia Symptom Questionnaire (DSQ) scores: the scores improved with weekly dupilumab as compared with placebo, with differences of –12.32 (95% CI, –19.11 to –5.54) in Part A and –9.92 (95% CI, –14.81 to –5.02) in Part B (both P<0.001) but not with dupilumab every 2 weeks (difference in Part B, –0.51; 95% CI, –5.42 to 4.41)
The most common adverse effect was injection site reactions. There were 10 serious adverse events; none of these “were considered by the trial investigators to be related to the trial regimen.”
In the associated commentary, (pg 2379-2380), Dr. Alex Straumann notes that since EoE is localized to the esophagus, whether a patients should be treated with a systemically acting medication, “particularly in light of the fact that topical glucocorticoids have been shown to be as efficacious as systemically acting prednisone.”
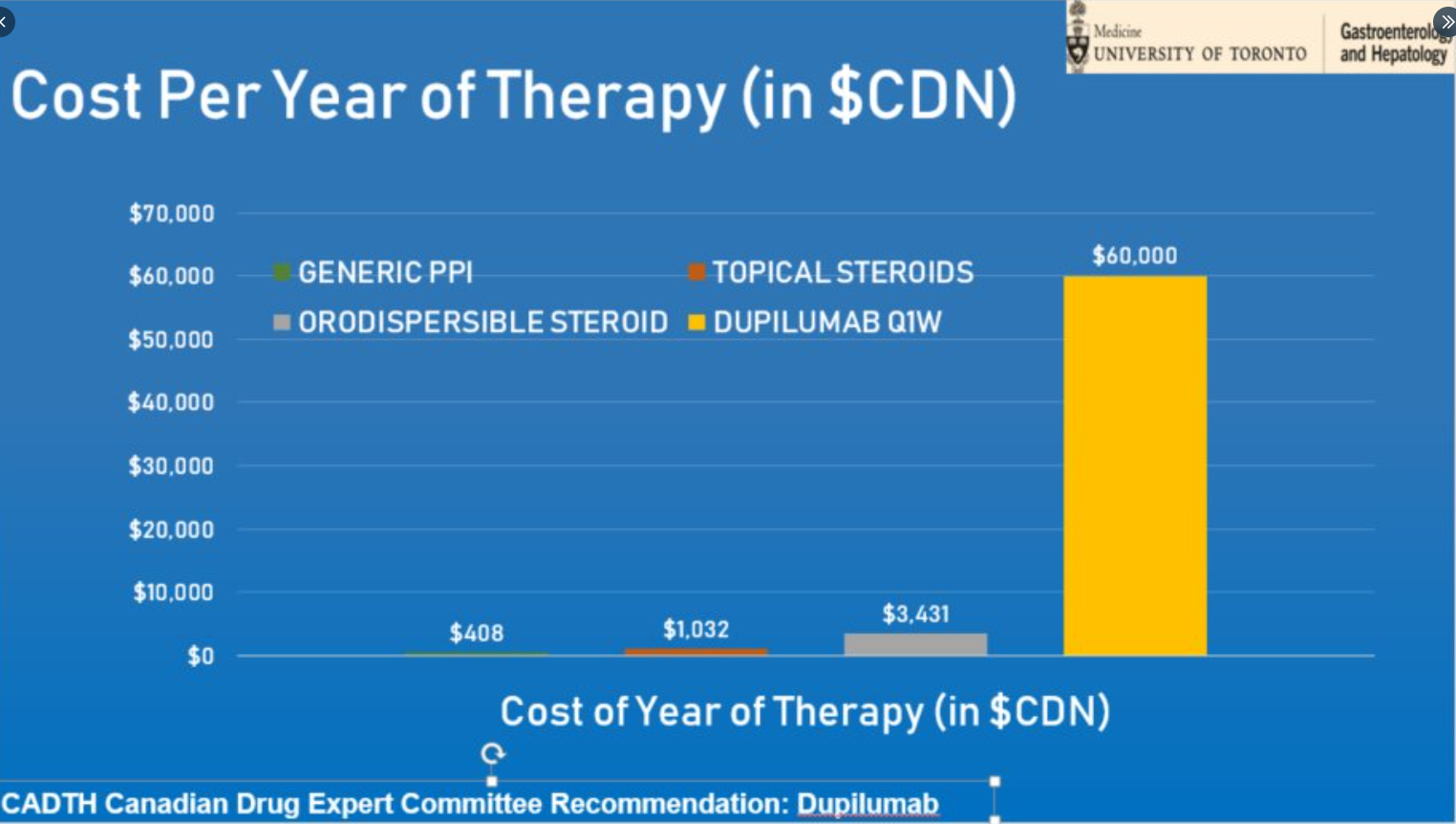
My take (borrowed in part from editorial): It remains unclear whether dupilumab “is better than the good old topical glucocorticoids in improving disease outcomes, particularly in light of considerable costs associated with this treatment.” Due to its cost (see below), dupillumab is likely best situated as a 2nd line treatment at this time for most patients.
Food recipes -type ingredients you have at home, and ask it for a recipe
Explain complicated topics at age-appropriate levels
Travel itinerary (can specify if active vacation, with kids, specific goals)
Recommendation letters
Resumes
Lesson plans
Solve complex math problems in step-by-step fashion
Provide scientific/journal references
Write music in almost any genre
Write essays and develop ideas for novels
Provide personal advice
Create content in multiple languages
Medication appeal letters
Write or fix computer coding/software
Develop questions for speaker question and answers
Prep for interview
My take: Only George Santos can claim more accomplishments than ChatGPT (AI). It is important to verify the information that ChatGPT provides –it is sometimes wrong.
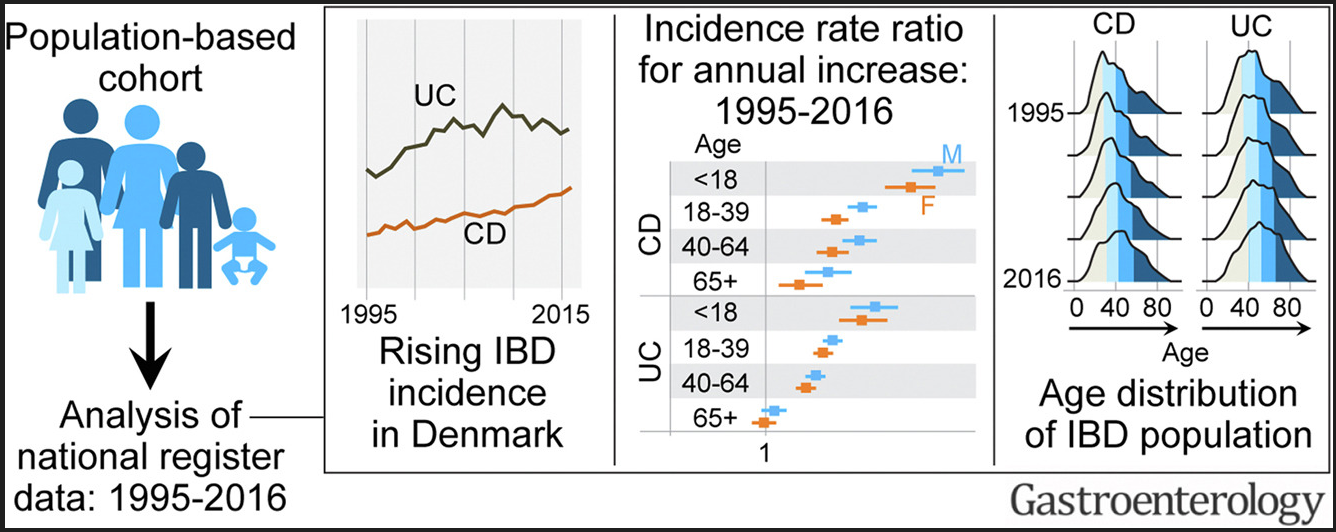
Between 1995 and 2016, the incidence rate (95% confidence interval) per 100,000 person-years rose from 9.1 (8.3–10.0) to 17.8 (16.8–19.0) for CD, and from 21.0 (19.8–22.3) to 28.4 (27.0–29.8) for UC.
The highest increase in CD and UC incidence rates occurred in children and young adults, respectively.
The prevalence of IBD doubled from 1995 to 2016; the greatest increase (2.5-fold) was in UC prevalence among individuals aged >40 years. During this period, the median age of the IBD population increased by 6 to 7 years.
In this retrospective study (n=130), therapeutic drug levels in the postoperative period were associated with improved outcomes for anti-TNF agents (infliximab (IFX) or adalimumab (ADA) but NOT for ustekinumab (UST):
In patients with IFX ≥3 µg/mL, higher rates of deep remission (39% vs 0%; P = .02) existed compared with those with IFX less than 3 µg/mL. This was true for clinical remission (44% vs 9%; P = .04) and objective (83% vs 62%; P = .1) remission.
In patients with ADA ≥7.5 µg/mL, rates of deep (42% vs 0%; P = .02), clinical (42% vs 0%; P = .02), and objective (88% vs 40%; P = .007) remission were higher than patients with lower concentrations.
For UST, rates of deep (28% vs 17%; P = 1.0), clinical (33% vs 33%; P = 1.0), and objective (70% vs 67%; P = 1.0) remission were similar between patients regardless of drug concentration.
In this retrospective study (n=147), a fecal calprotectin >800 mcg/g independently predicted the need for inpatient medical rescue therapy (odds ratio, 2.61; 95% CI, 1.12-6.12). An admission calprotectin >800 mcg/g independently predicted surgery within 3 months (odds ratio, 2.88; 95% CI, 1.01-8.17). My take: This is the least surprising study I’ve read this past month —those with more severe colitis, based on calprotectin values, were more likely to need more intensive treatments.
In this retrospective pediatric study (n=171), the authors found that a generic oral supplement (Fortsip) was as effective as a specialized formula (Modulen IBD) for enteral nutrition. “No difference was demonstrated in remission rate (Fortisip n = 67 of 106 [63%] vs Modulen IBD n = 41 of 64 [64%], P = .89), nonadherence rate (Fortisip n = 7 of 106 [7%] vs Modulen IBD 3 of 64 [5%], P = .57) or method of administration.” The main difference in outcome was a lower expense in the group receiving the generic formula. My take: This study is in agreement with previous studies.
In total, 6723 patients completed new patient gastroenterology visits for a primary diagnosis of constipation between 2013 and 2019. Of these, 993 (14.8%) patients had abdominal radiographs taken within 24 hours of their initial visit. Over the 7 years of this project, a mean frequency of abdominal radiograph use decreased from 24% to less than 11%.
No increases in subsequent emergency department visits or hospitalization for constipation within 30 days of patients’ initial visits were seen.
One of the keys to improvement was providing data to individual providers
The authors note that routine radiographs are NOT recommended by expert guidelines in patients presenting with functional constipation.
My take: The trend of using radiographs less frequently shows that a QI project can help avoid low value testing though more than 10% is still too high.
In this retrospective study from Israel with nearly 600,000 children, key findings:
The incidence rate of acid-suppressant medication use increased by 2.8-fold from 18.2 per 1000 in 2005 to 51.0 per 1000 in 2020
Primary care providers accounted for 74.8% of prescribing physicians in 2005 vs 96.1% in 2020, whereas the prevalence of prescribing gastroenterologists decreased from 18.8% to 2.8%
Other factors associated with increased use: first born child, male sex, multiple births and greater socioeconomic status; this latter group is more likely driven by health-seeking tendency rather than financial disparity due to national health insurance
Comments: This high use of acid suppression medications in infancy has been reported in multiple other studies despite the lack of efficacy in prior studies. Pediatricians, more than pediatric gastroenterologists, may be less familiar with the GERD guidelines and potential adverse effects of acid suppression (including association with an increase food allergies).
My take: This Israeli study shows that pediatric gastroenterologists are using acid blockers less in infants while pediatricians are using them more often. It is interesting that after the first child, parents are less likely to seek medical attention & are more tolerant of reflux symptoms.
Methods: VEDOKIDS was a paediatric, multicentre, prospective cohort study done in 17 centres in six countries. We report the 14-week outcomes as the first analyses of the planned 3-year follow-up of the VEDOKIDS cohort
Key findings:
32 (42%) of 77 children with ulcerative colitis and 21 (32%) of 65 children with Crohn’s disease were in steroid-free and exclusive enteral nutrition-free remission at 14 weeks.
In children who weighed less than 30 kg, the optimal drug concentration associated with steroid-free and exclusive enteral nutrition-free clinical remission was 7 μg/mL at week 14, corresponding to a dose of 200 mg/m2 body surface area or 10 mg/kg
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
“Rebyota is approved for the prevention of recurrence of Clostridioides difficile infection (CDI) in individuals 18 years of age and older. It is for use after an individual has completed antibiotic treatment for recurrent CDI.”
“Rebyota is administered rectally as a single dose [150 mL]. Rebyota is prepared from stool donated by qualified individuals….The effectiveness of Rebyota was evaluated in an analysis of data from a randomized, double-blind, placebo-controlled, multicenter study….the overall estimated rate of success in preventing recurrent CDI through 8 weeks was significantly higher in the Rebyota group (70.6%) than in the placebo group (57.5%).”
My take: As pharmaceutical companies gain approval for fecal transplant products, I would anticipate a significant increase in costs. This product seemed to have a fairly low success rate compared to placebo.
Methods: This was a double-blind, randomized, sham-controlled trial in patients (n=100) with nocturnal symptoms of gastroesophageal reflux. Patients were advised to sleep in the left lateral decubitus position and were assigned randomly (1:1) to an electronic sleep positional therapy wearable device (applied with an adhesive sticker), programmed to either produce a vibration when in the right lateral position (intervention) or only during the first 20 minutes (sham).
Key findings:
In the intention-to-treat analysis, the rate of treatment success (defined as a 50% or more reduction in the nocturnal reflux score) was 44% in the intervention group (22 of 50) vs 24% in the sham group (12 of 50)
There was increased time sleeping in the left lateral decubitus position (intervention 60.9% vs sham 38.5%)
My take: In those with nocturnal heartburn, this appears to be a helpful nonpharmacological tool.
Website for the company (side sleep technologies) that makes the device: The Left ” Your body will be conditioned to sleep at least 80% on your left within a week.” (I do not have any financial relationship with this company).
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
This was a cross-sectional study of caregivers of children (n=34) with intestinal failure receiving long-term parenteral nutrition. 97% of caregivers were the child’s mother and median duration of providing care among respondents was 3.4 years.
Key findings:
Caregivers reported a median of 29.2 hours per week (IQR, 20.8-45.7 hours per week) of direct medical care. 6.1 hours was spent on providing PN and care of the central venous catheter. 6.3 hours was spent on enteral nutrition and enteral tube care.
In the associated editorial (pgs 10-12 by S Mauskar, JG Berry. Open Access! “Failing to Support Families’ Burden of Care for Children with Intestinal Failure“), the authors note that in the U.S. there has been a growing population of children at home with greater medical complexity and reliance on medical technology and that the need for home nursing support “greatly exceeds the supply, leaving many families on their own to care for their children.”
They also note that the medical literature (over the last 25 years) on caregiver burden for children notes it is associated with “marital discord, loss of employment, and financial struggle…In the U.S. a substantial portion of children with medical complexity assisted with technology live in single-parent households, in poverty, and are exposed to adverse childhood events…very vulnerable to the effects of high caregiving burden.”
My take: This study shows that while we have an effective treatment for intestinal failure, the burden of this treatment is very high even with care coordination and social worker help. Understanding this burden could help medical providers be more empathetic for the family who is struggling with home medical care (eg. child with recurrent admissions for central line infections).