Online Webinar –Annual Aspen Conference —July 14, 2000
Below I’ve included a few slides and some notes; my notes may have errors of omission or transcription.
Biliary Atresia -Prompt Diagnosis and Screening Ronald Sokol
Key Points:
- We have NOT improved age of diagnosis in biliary atresia in the past 30 years
- Uniform screening of fractionated bilirubin has been effective in Texas: Diagnostic Yield of Newborn Screening for Biliary Atresia Using Direct or Conjugated Bilirubin Measurements S Harpavat et al. JAMA 2020; 323: 1141-50
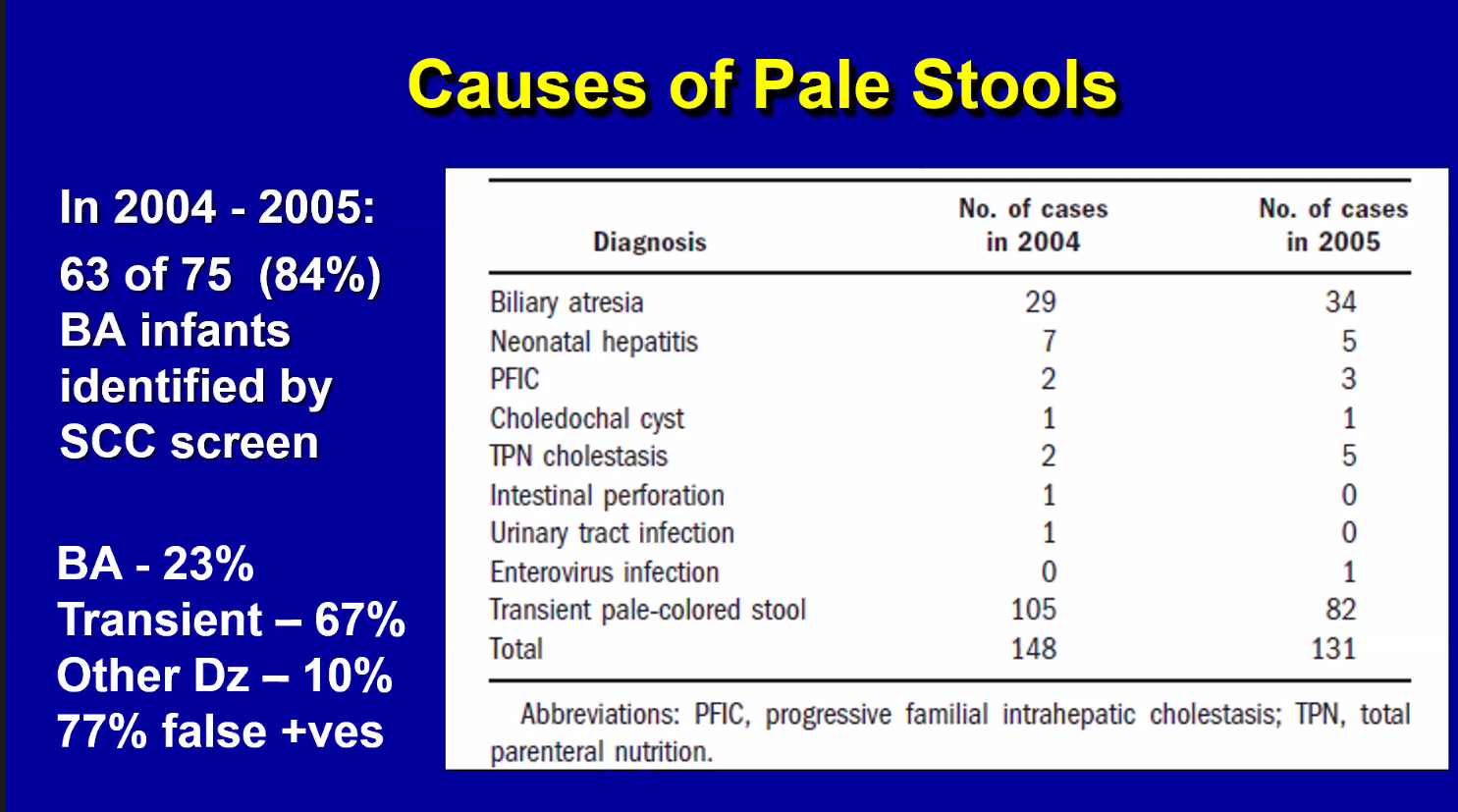
- Pale stools are usually NOT due to biliary atresia but should prompt investigation (eg. fractionated bilirubin)
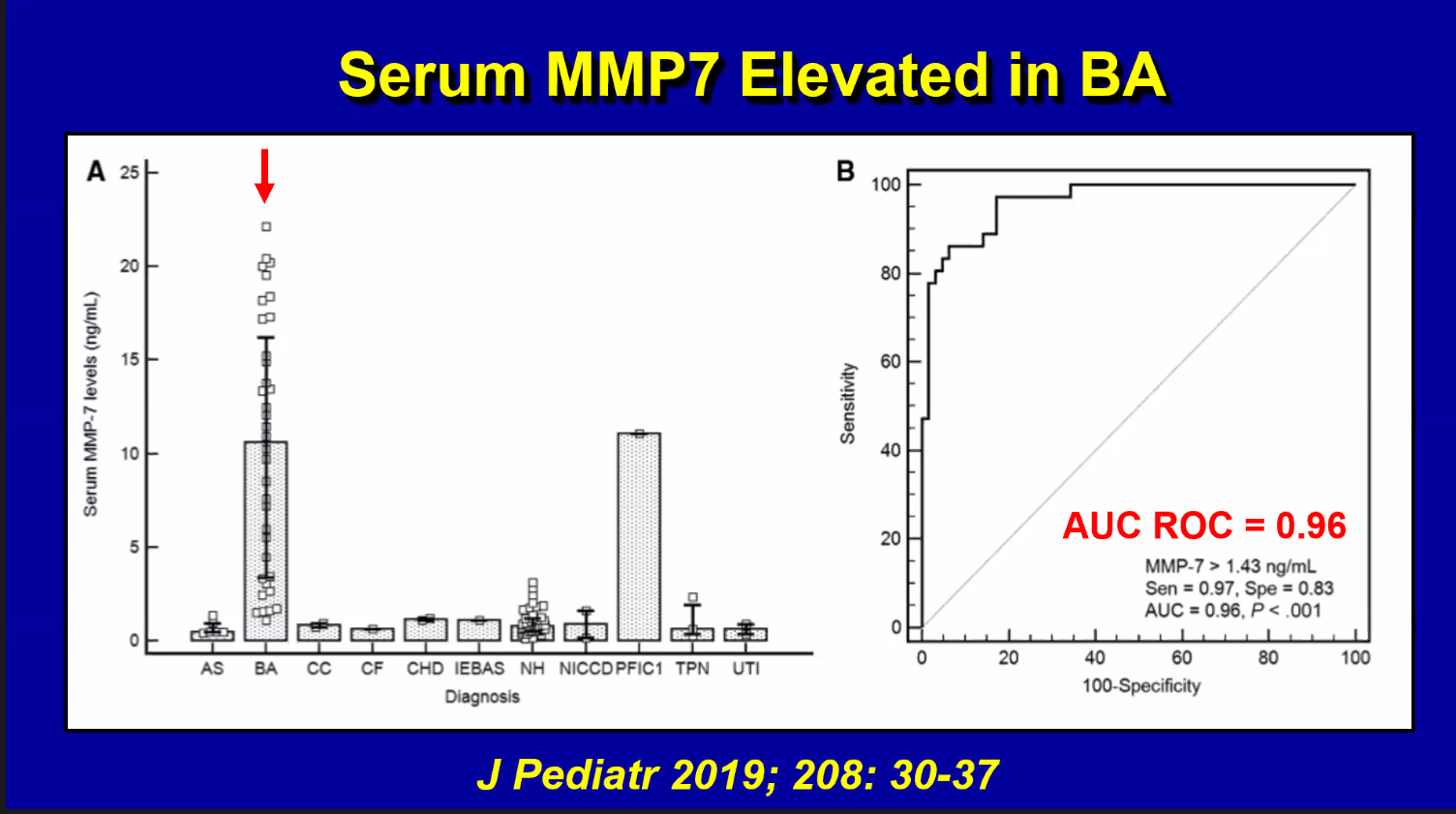
- MMP-7 may improve diagnostic approach; unclear if MMP-7 performs well in all populations (eg. prematurity)
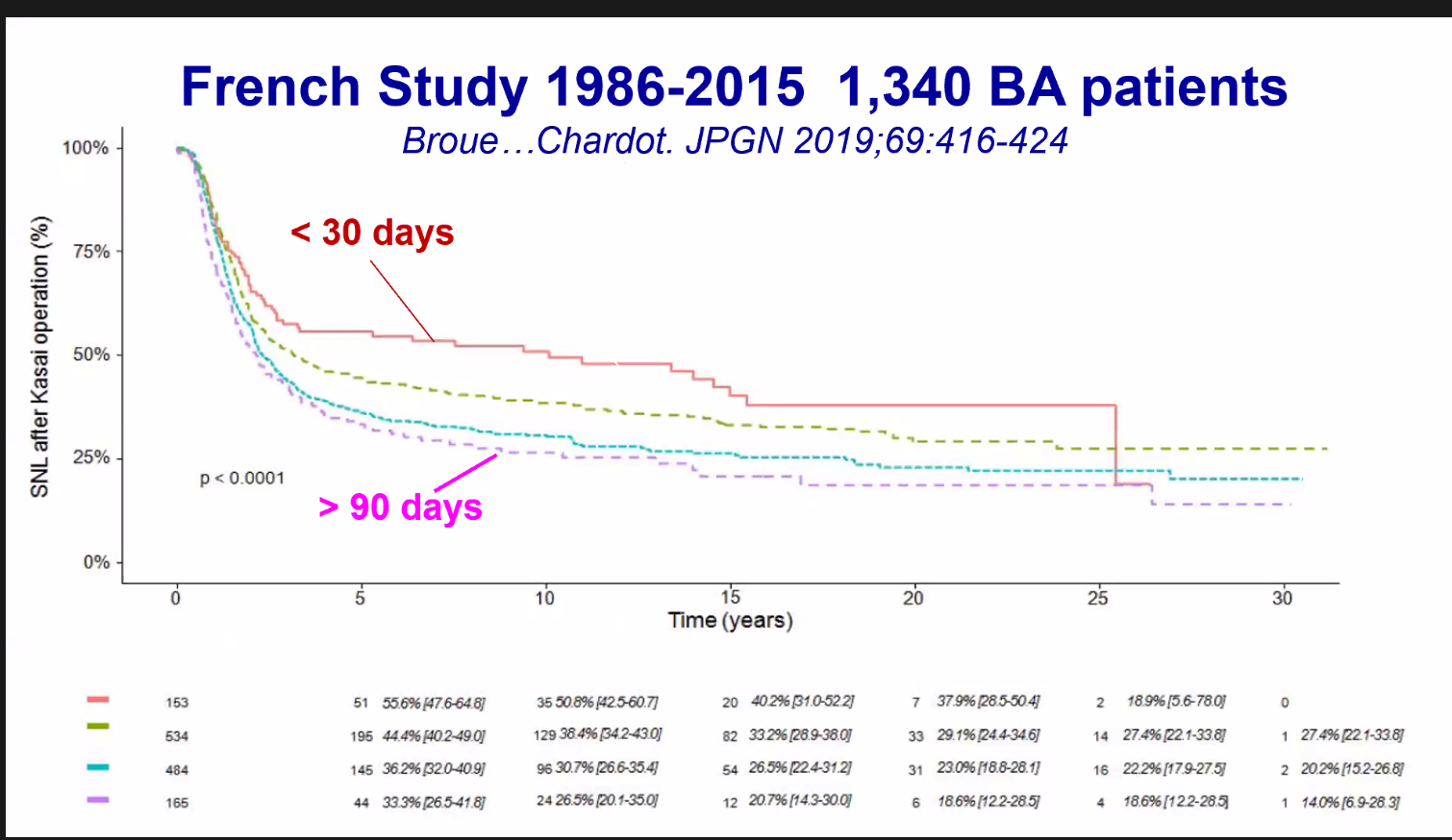
- Outcome key factors: age at diagnosis (goal less than 30-45 days) and surgeon/center











Related blog posts:
- Newborn Bilirubin Measurements To Identify Biliary Atresia | gutsandgrowth
- One More Problem with HIDA Scans
- Biliary Atresia Biomarkers 2020
- More data, More Nuance with MMP-7
- Will We Still Need Liver Biopsies to Diagnose Biliary Atresia in a Few Years?
- Diagnosing biliary atresia earlier | gutsandgrowth
- Helpful Review on Biliary Atresia | gutsandgrowth
- Biliary Atresia More Common in Preterm Infants | gutsandgrowth
- High Survival Rates for Biliary Atresia Patients Needing Liver Transplantation
- What to Expect After Pediatric Liver Transplantation: Cognitive Function and Quality of Life
- 30 -Year Outcomes with Biliary Atresia
- Outcomes of Liver Transplantation in Small Infants
- “Big Improvements for Smallest Recipients” with Bad Liver Disease