HL Thel et al. Clin Gastroenterol Hepatol 2025; 23: 272-280. Open Access! Prevalence and Costs of Eosinophilic Esophagitis in the United States
Methods: Using two large administrative databases, MarketScan and Medicare, the authors estimated annual prevalence of EoE, as well as age- and sex-stratified estimates, standardized to the U.S. population. Health care utilization, including medications and endoscopic procedures, was quantified, and annual EoE-associated costs were calculated.
Key findings:
- There was a 5-fold increase in prevalence in both databases since 2009.
- Standardized to the U.S. population, the prevalence of EoE was 142.5/100,000, extrapolating to 472,380 cases. This equates to ~1 in 700 persons.
- Total EoE-associated annual health care costs were estimated to be $1.32 billion in 2024 dollars after accounting for inflation.
- PPIs were used more commonly than steroids for treatment. For Marketscan in 2022, PPIs were used in 41% and steroids in 26%.


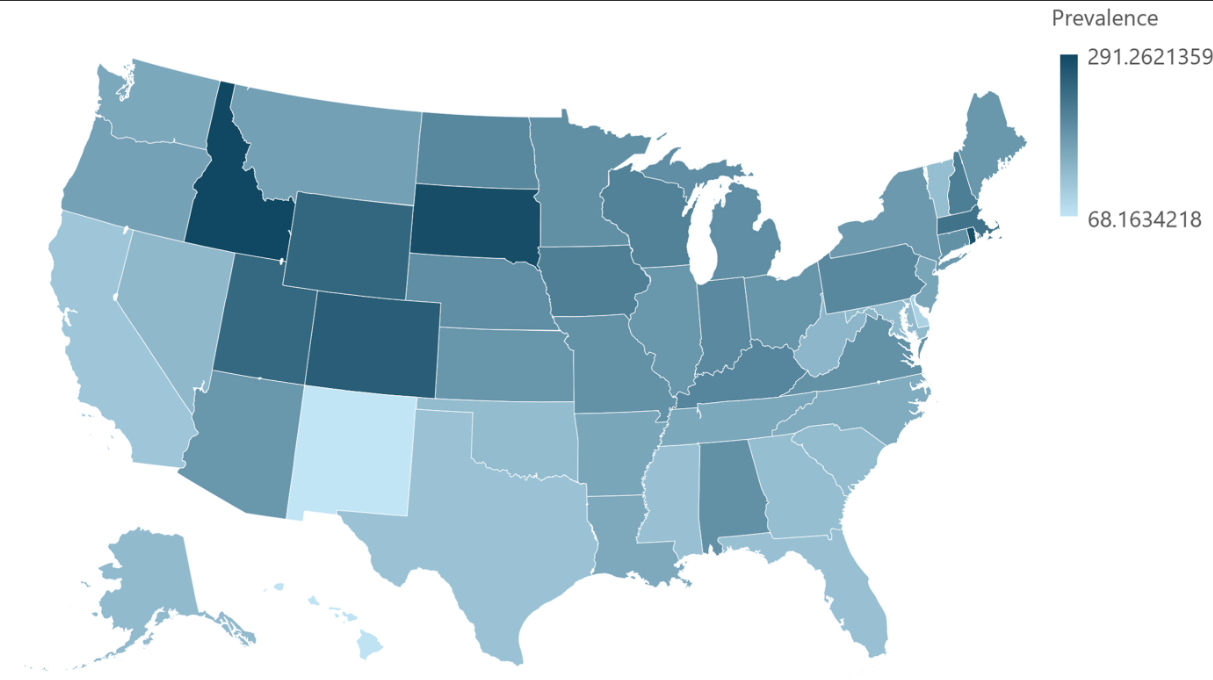
My take: There is likely a true increase in the number of affected individuals, though some changes in prevalence are due to an increased recognition/testing of eosinophilic esophagitis.
Related blog posts:
- Eosinophilic Esophagitis -Increasing Incidence and Emergence of Biologic Treatments (2024)
- ACG 2025 Guidelines for Eosinophilic Esophagitis
- Increasing Burden of Eosinophilic Esophagitis (2023)
- Highest Reported Prevalence Rates for Eosinophilic Esophagitis (2019)
- How Common is Eosinophilic Esophagitis? (2014)
- ESPGHAN Eosinophilic Esophagitis Guidelines (2024)
- NASPGHAN YouTube Video for Eosinophilic Esophagitis
- 1-Food vs 4-Food Elimination Diet for Eosinophilic Esophagitis
- When to Use Dupilumab for Eosinophilic Esophagitis: Multispecialty Guidelines
- Landmark Dupilumab Study for Eosinophilic Esophagitis
- Dupilumab: FDA Approval for Eosinophilic Esophagitis
- Practical Guide to Dietary Therapy for Eosinophilic Esophagitis
- But How Well Does It Work in Theory and Eosinophilic Esophagitis Treatments
- When To Take Fewer Biopsies With Eosinophilic Esophagitis