Last fall, the FDA approved a liquid version of omeprazole.
9/3/22Drugs.com: “FDA Approves Konvomep. FDA Approves Konvomep (omeprazole and sodium bicarbonate for oral suspension) for Gastric Ulcer and Reduction of Risk of Gastrointestinal Bleeding in Critically Ill Patients
WOBURN, Mass. (September 2, 2022) – Azurity Pharmaceuticals, Inc., a pharmaceutical company focused on developing innovative dose-forms and formulations of products to serve the needs of overlooked patients, announced today that the U.S. Food and Drug Administration (FDA) has approved Konvomep (omeprazole and sodium bicarbonate for oral suspension).“
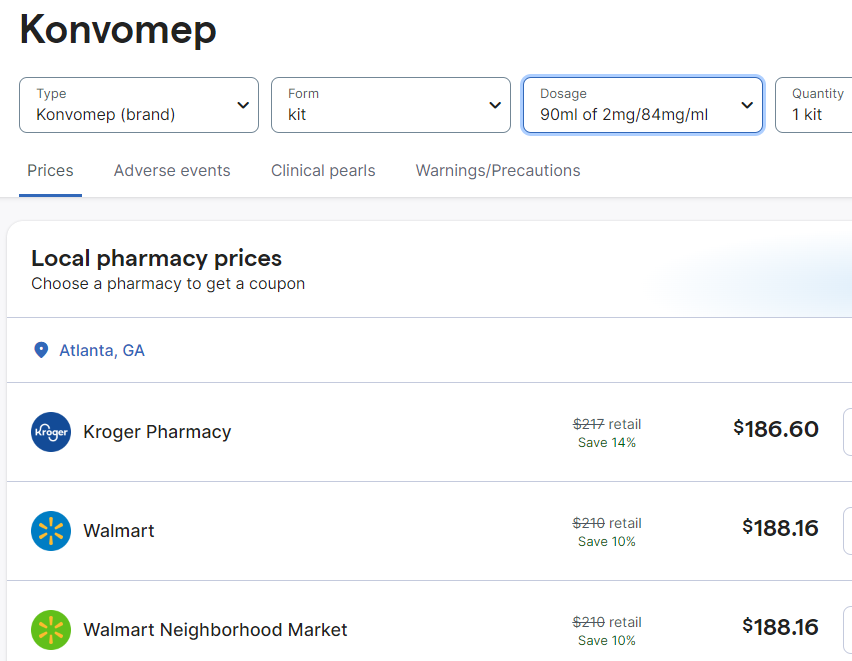
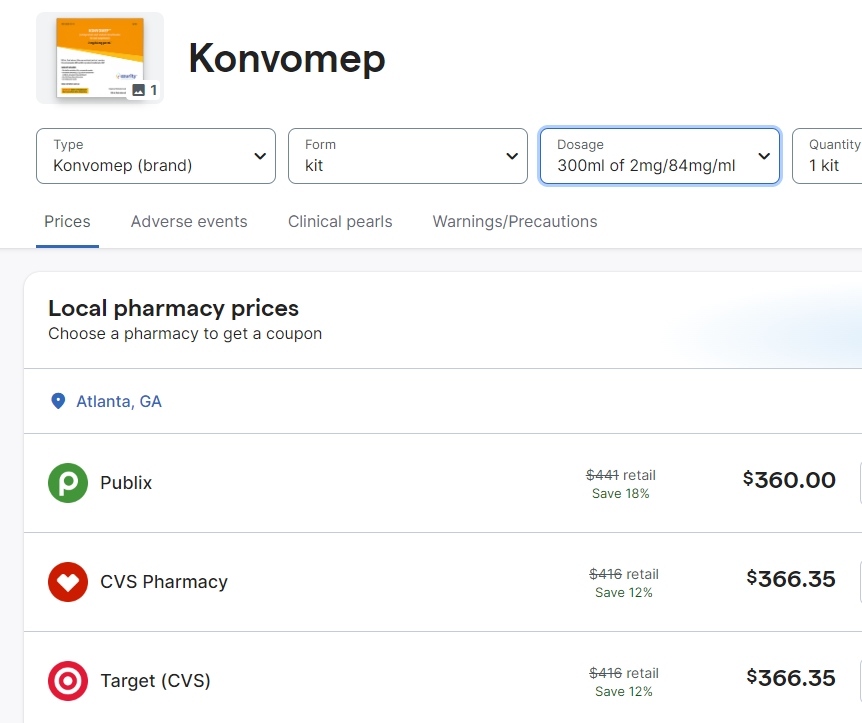
Now that this FDA approved product is available, it may be that it will be more difficult to receive a compound version. The cost of this new formulation is much higher. Here are some of the costs from GoodRx.com.
My take: The high cost of this liquid preparation is another good reason to avoid using a PPI in patients with low likelihood of benefit.
This retrospective study analyzed data from 11,965 infants who had fractionated bilirubin obtained in the nursery (2016-2019). Key findings:
DB of 0.6 mg/dL was chosen as the cut-off based on a high sensitivity (100%) and specificity (99%) for screening newborns for CLD
Out of 60 infants who met criteria for DB ≥0.6 mg/dL, only 15 (25%) had a repeat level drawn after nursery discharge; 3 (5%) were eventually diagnosed with CLD (2 with BA and 1 with Alagille syndrome)
It is fairly easy to get fractionated bilirubins on infants. Many need to get a bilirubin check and in many centers, a fractionated bilirubin is automatically generated at no additional costs. The hard part is making sure that those with abnormal values receive timely followup.
My take: It is a mistake to get fractionated bilirubins in newborns unless one has developed a plan/infrastructure to make sure those with abnormal values receive appropriate followup.
L D’Antiga et al. NEJM; 2023; 389: 620-631. Gene Therapy in Patients with the Crigler–Najjar Syndrome
Methods: Five patients received a single infusion of the gene construct (GNT0003): two received 2×1012 vector genomes (vg) per kilogram of body weight, and three received 5×1012 vg per kilogram. The primary end points were measures of safety and efficacy; efficacy was defined as a serum bilirubin level of 300 μmol per liter or lower measured at 17 weeks, 1 week after discontinuation of phototherapy. The infusion protocol included administration of sirolimus adjusted for a trough of 4-12 mcg/L (starting 1 week prior to infusion) and steroids (IV day prior then oral for 8 weeks). .
Key findings
By week 16, serum bilirubin levels in patients who received the lower dose of GNT0003 exceeded 300 μmol per liter.
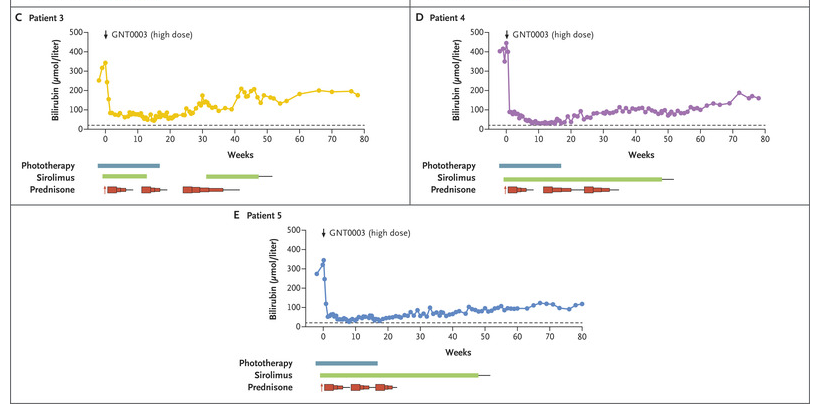
The patients who received the higher dose had bilirubin levels below 300 μmol per liter in the absence of phototherapy at the end of follow-up; mean level at the final follow-up visit [week 78 in two patients and week 80 in the other], was149±33 μmol per liter.
No serious adverse events were reported. Mild increase in ALT levels were seen in 4 of 5 patients; this was “potentially related to an immune response against the infused vector; these patients were treated with a course of glucocorticoids.”
This figure shows the response of the serum bilirubin in patients receiving the higher dose of the infusion.
My take: This study shows that the GNT0003 increased UGT1A1 activity to levels that permitted cessation of phototherapy; this persisted for 18 months after treatment. Further studies are needed.
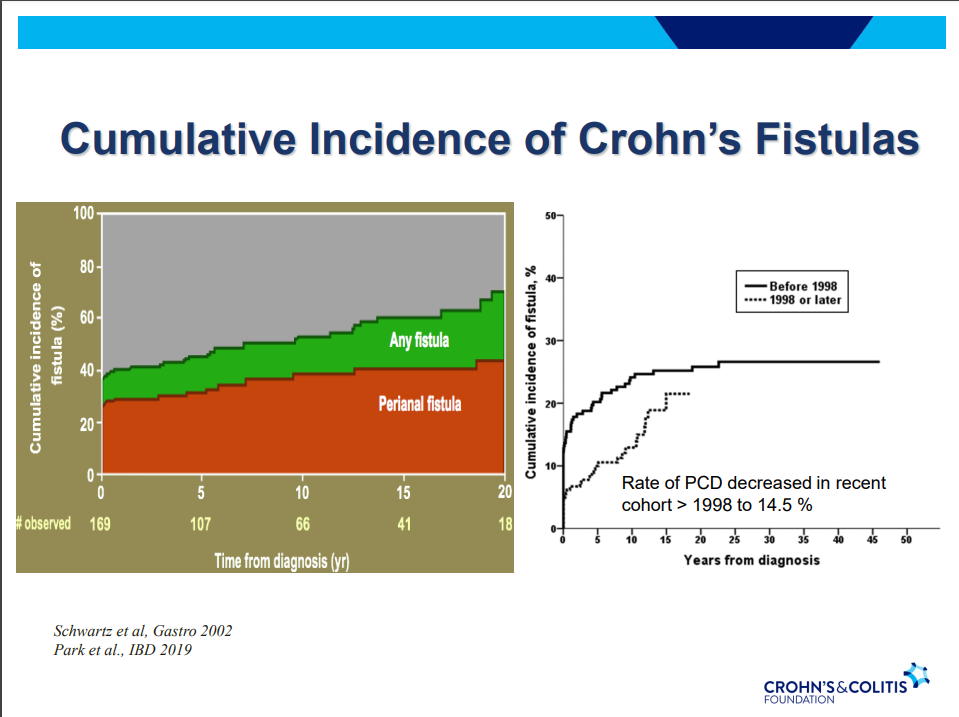
Another very good review by David Schwartz on The Daunting Duo: Management of Stictures and Fistula. Below are some of my notes and some slides; my notes may contain errors in transcription or omission. Can get access to all 49 slides here: IBD Pro CCFA 2023 Atlanta
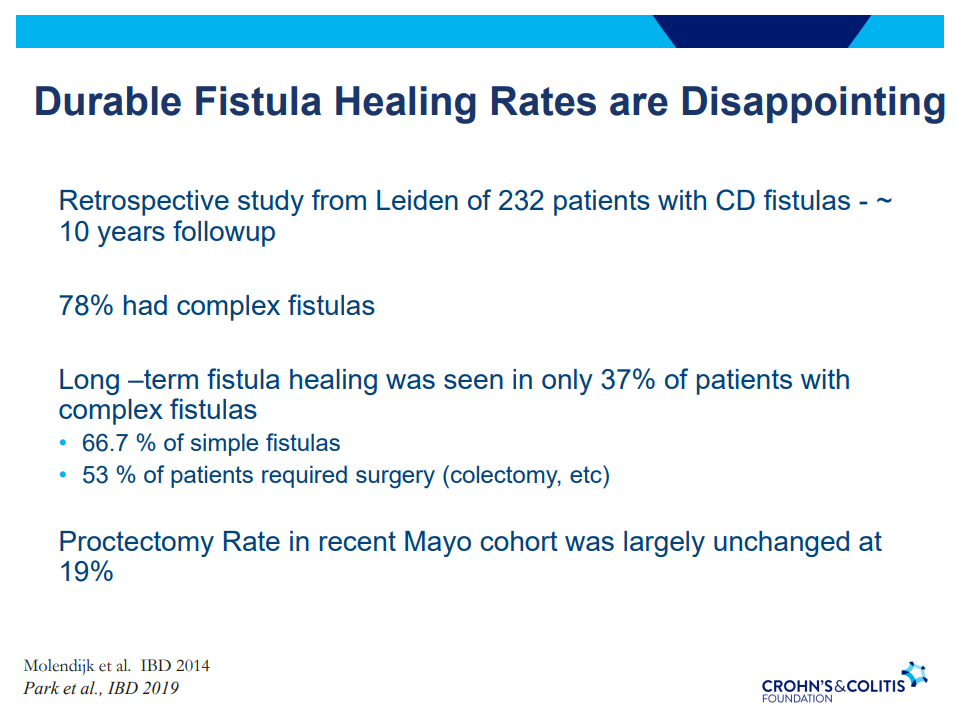
Fistula healing rates are poor
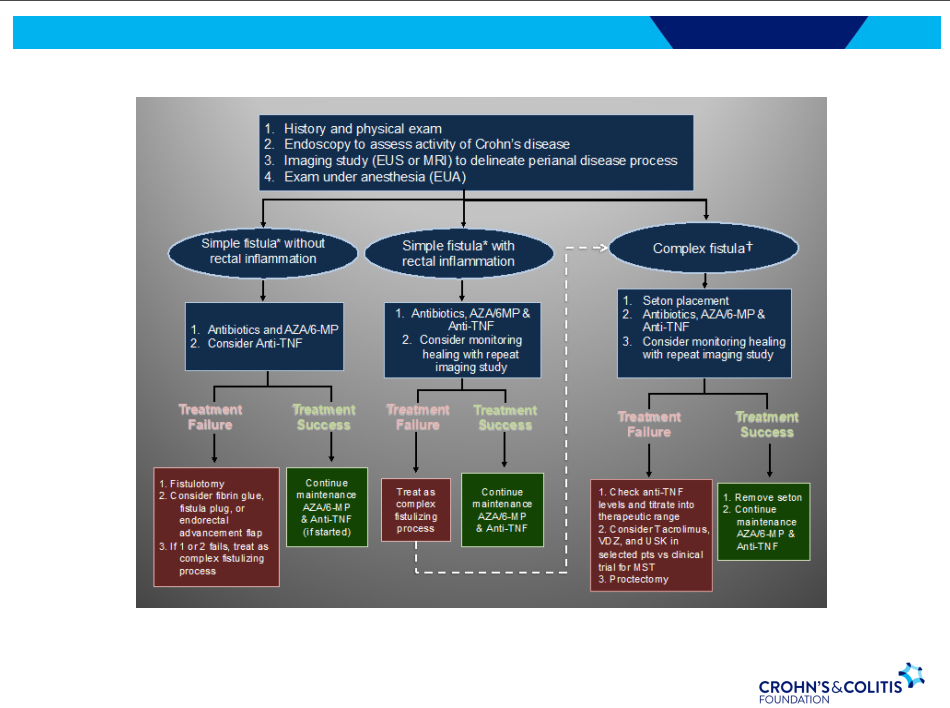
78% have complex fistulas
Long-term healing: 67% with simple fistulas but only 37% with complex fistulas
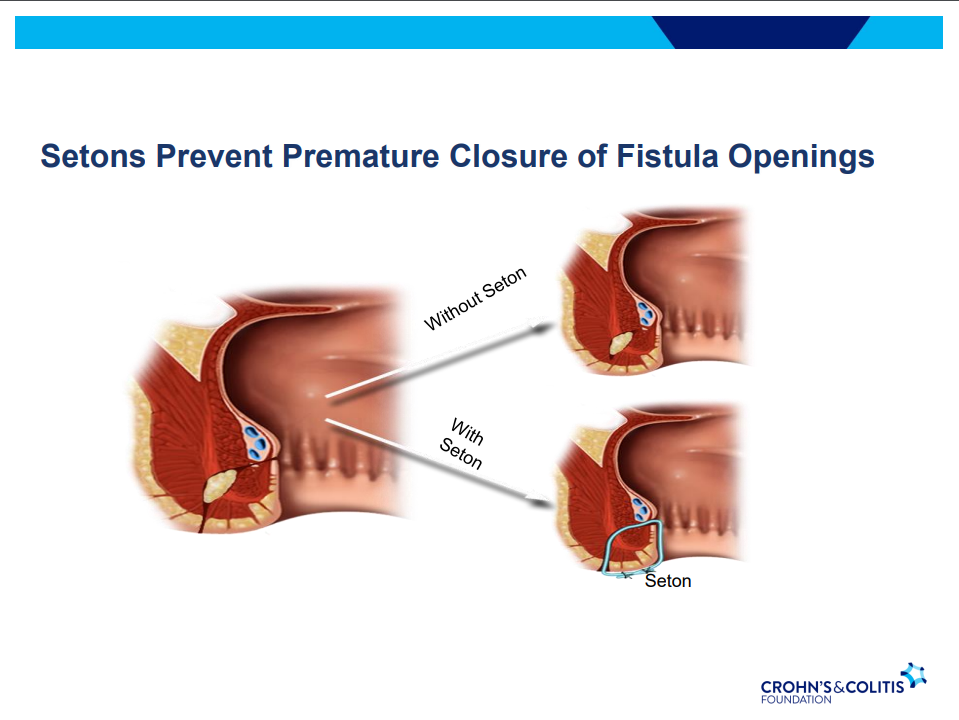
Seton placement prior to biologic therapy increases likelihood of better outcomes
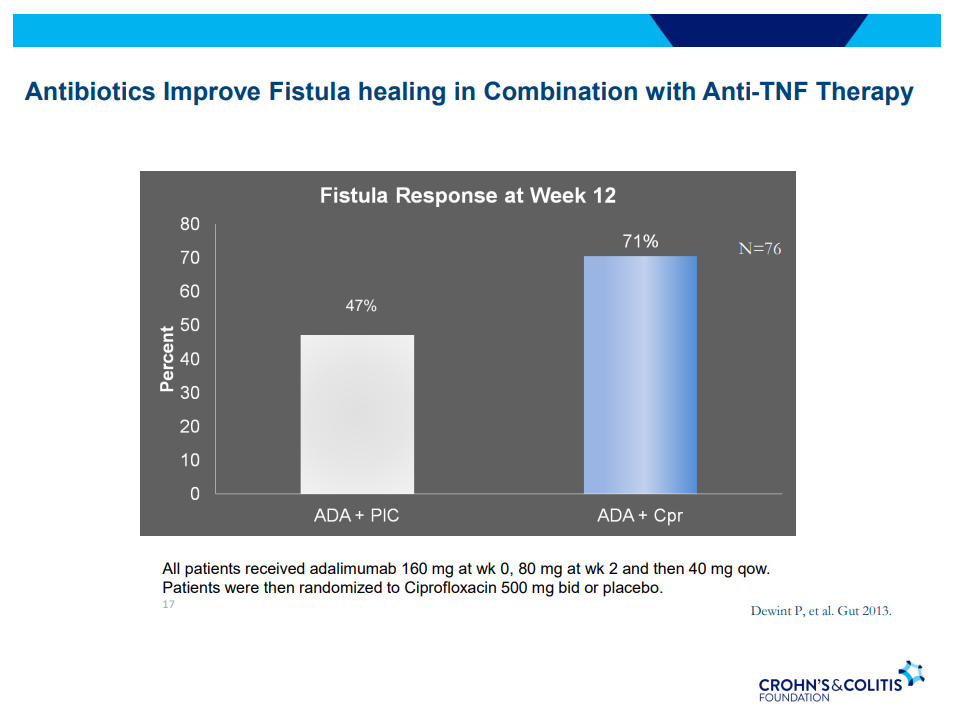
Antibiotic therapy recommended until Seton removed (not short-term treatment) –improved healing rates along with medical therapy
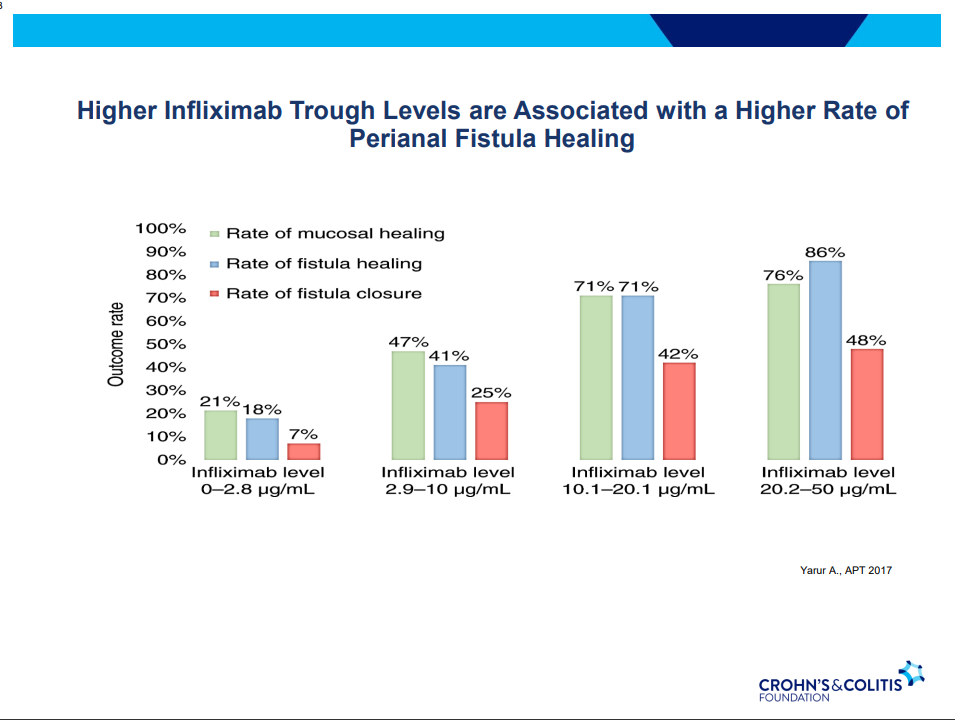
Anti-TNF therapy effective in ~40% long-term; higher rates of healing with higher anti-TNF levels
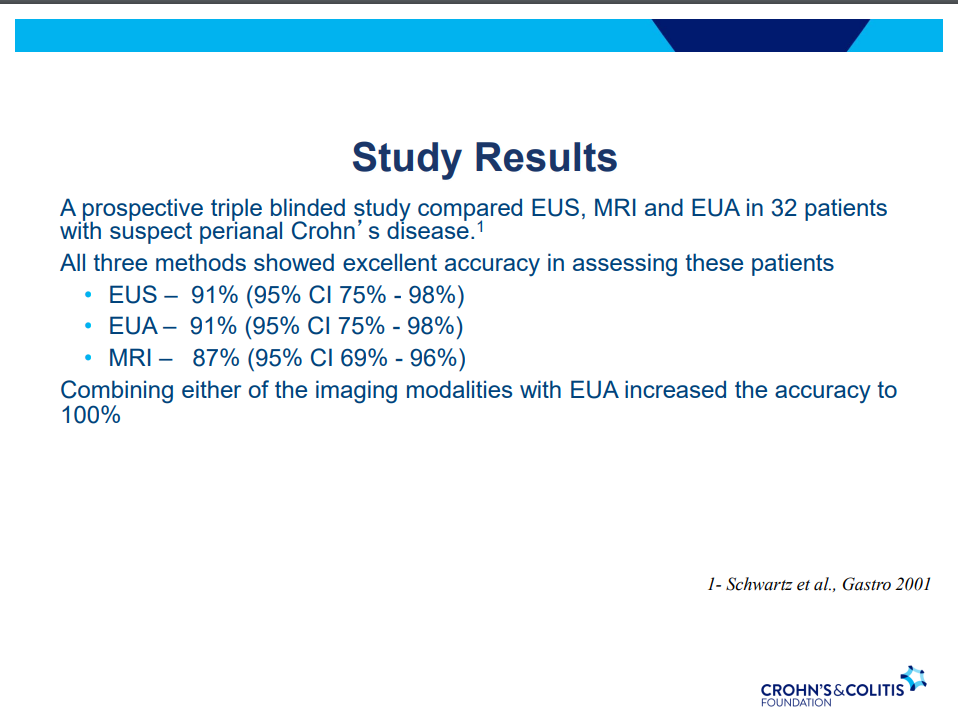
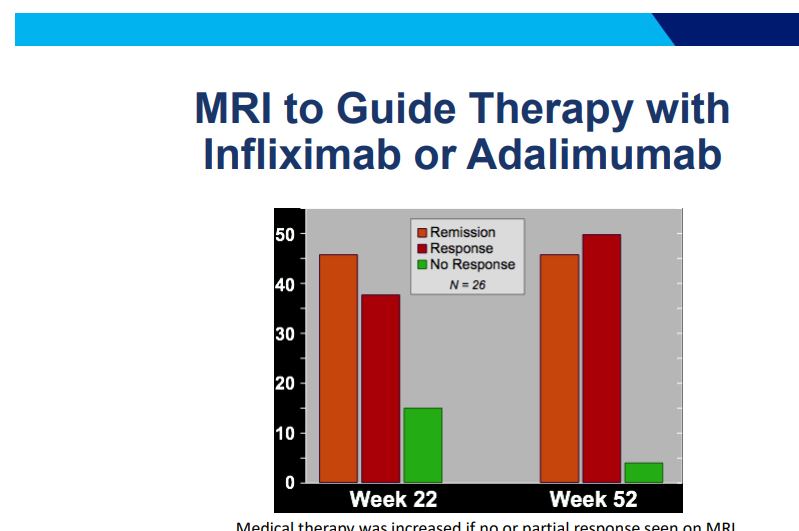
MRI and/or EUS helpful in improving fistula healing rates
Ustekinumab and Vedolizumab both had fistula healing rates ~40%
Adipose derived stem cells with ~50% healing rates (study with high placebo healing rate too ~37%); changes local cytokine profile, cells gone in about 2 weeks but goal for changing trajectory
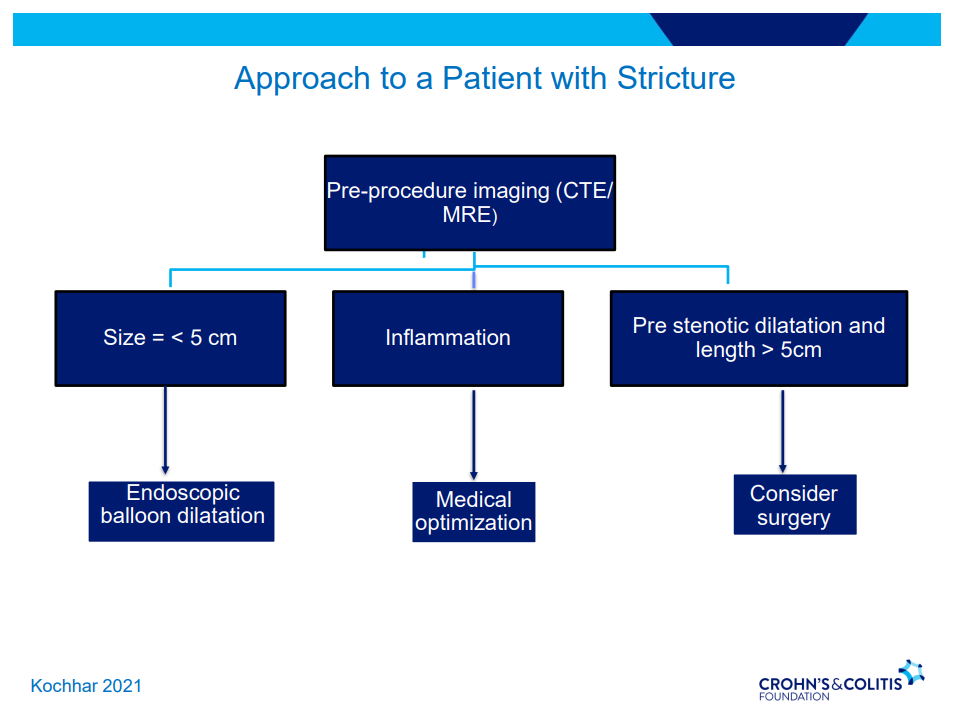
Strictures
5-24% with stricturing phenotype
No effective medical treatments
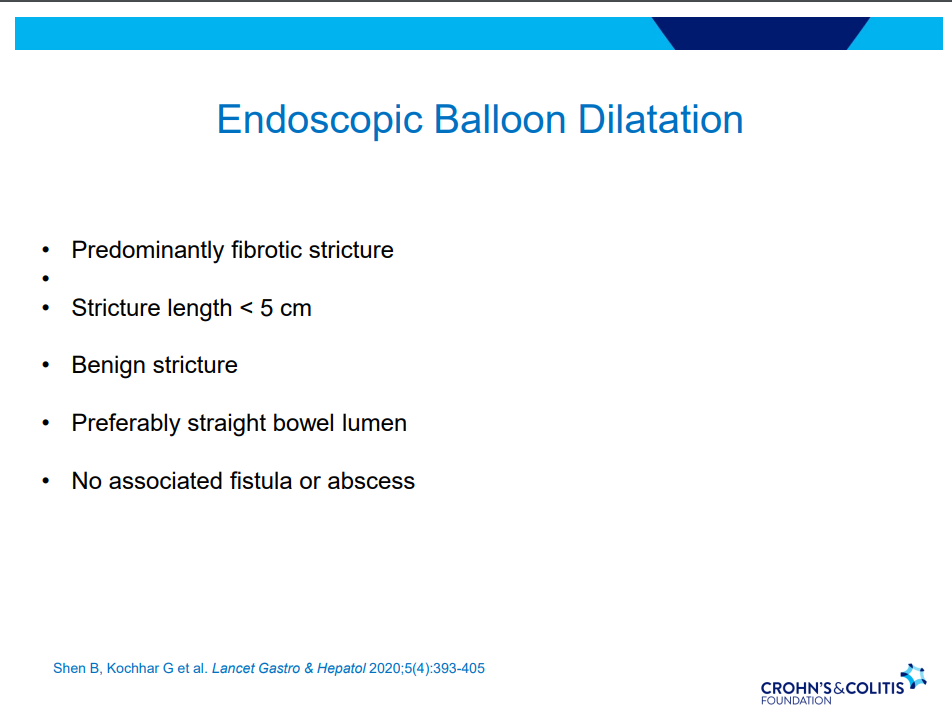
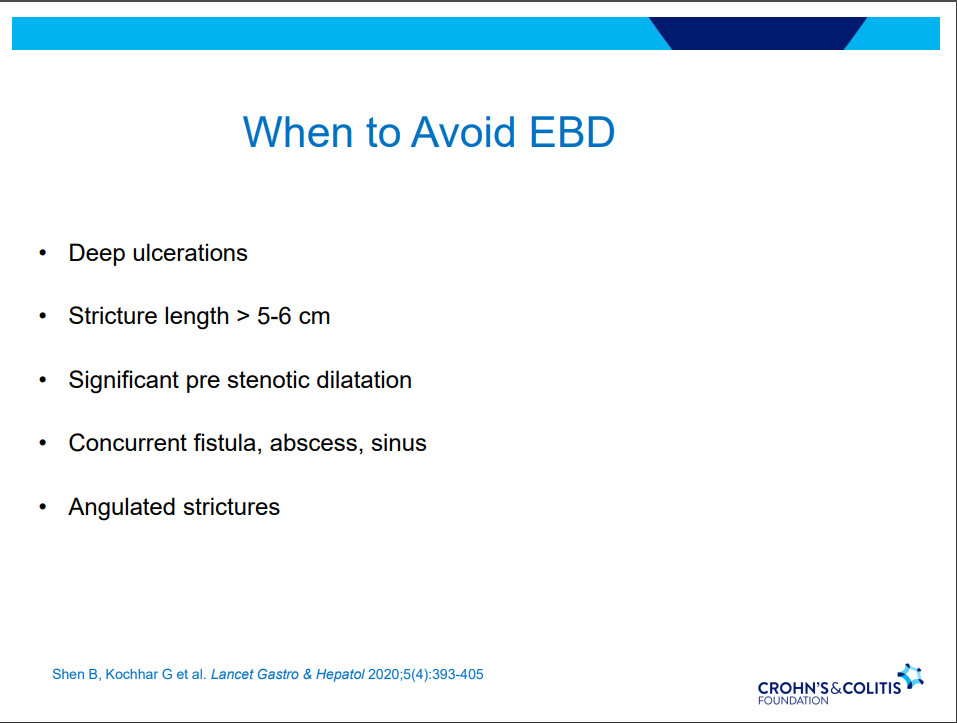
Endoscopic balloon dilatation in shorter strictures (<5 cm) without associated abscess or fistula (needs imaging prior)
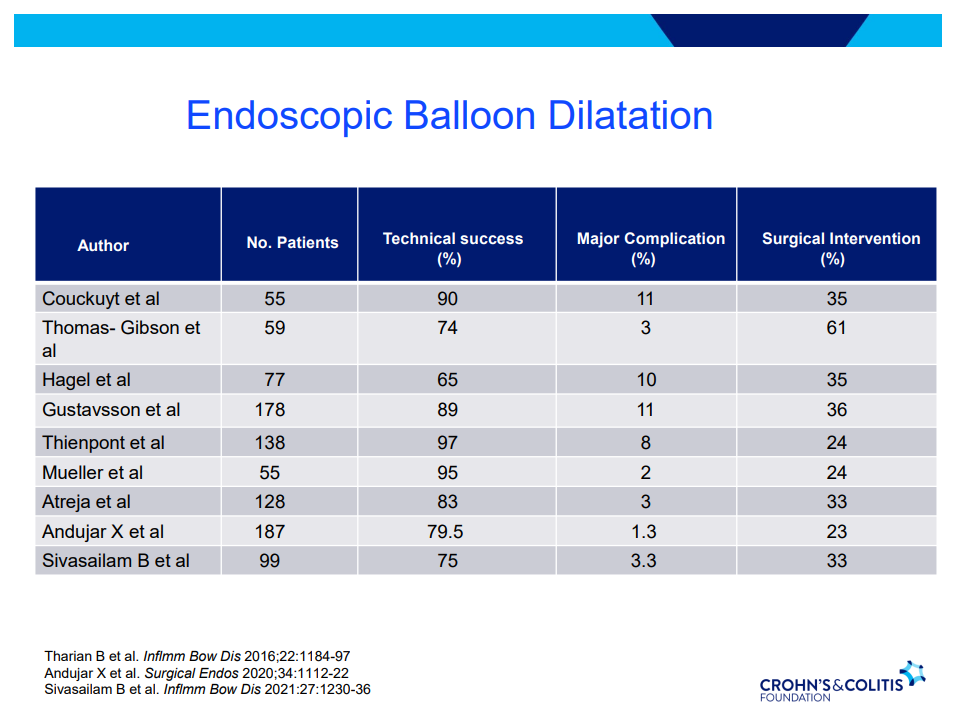
One-third of balloon dilated strictures will still wind up needing surgery despite dilatation. 5-10% risk of complication. Goal is 15 mm or more (Dr. Schwartz typically does not increase by more than 3 sizes from baseline in one session)
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
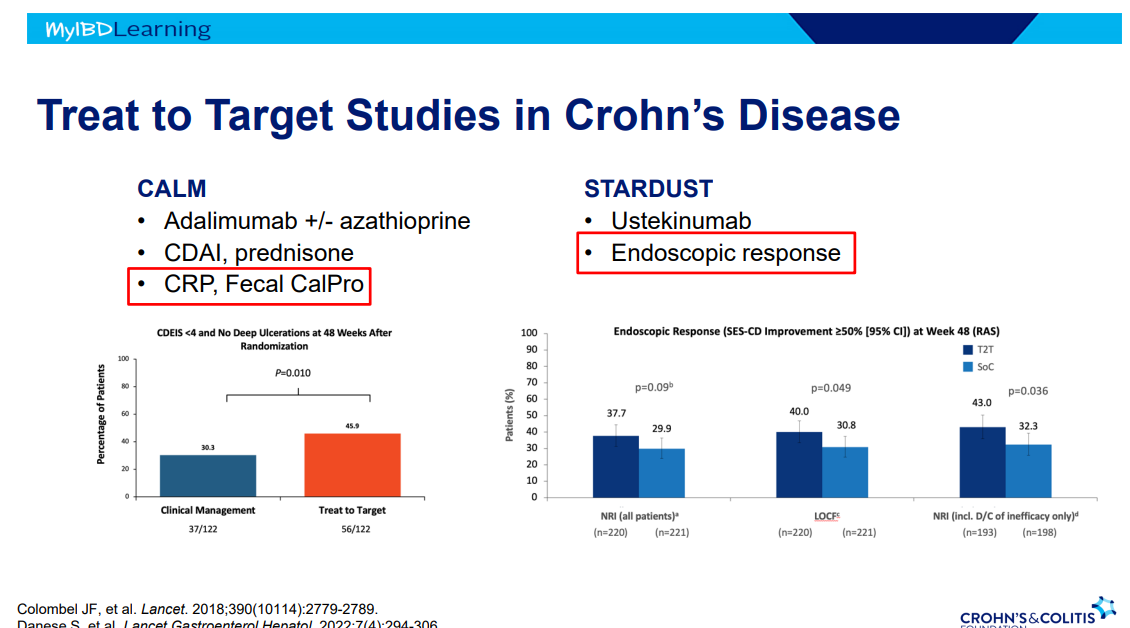
Another terrific lecture from David Rubin: Positioning of Advanced IBD Therapy. Here are my notes and some slides which could include errors in transcription and omission. Can get access to all 46 slides here: IBD Pro CCFA 2023 Atlanta
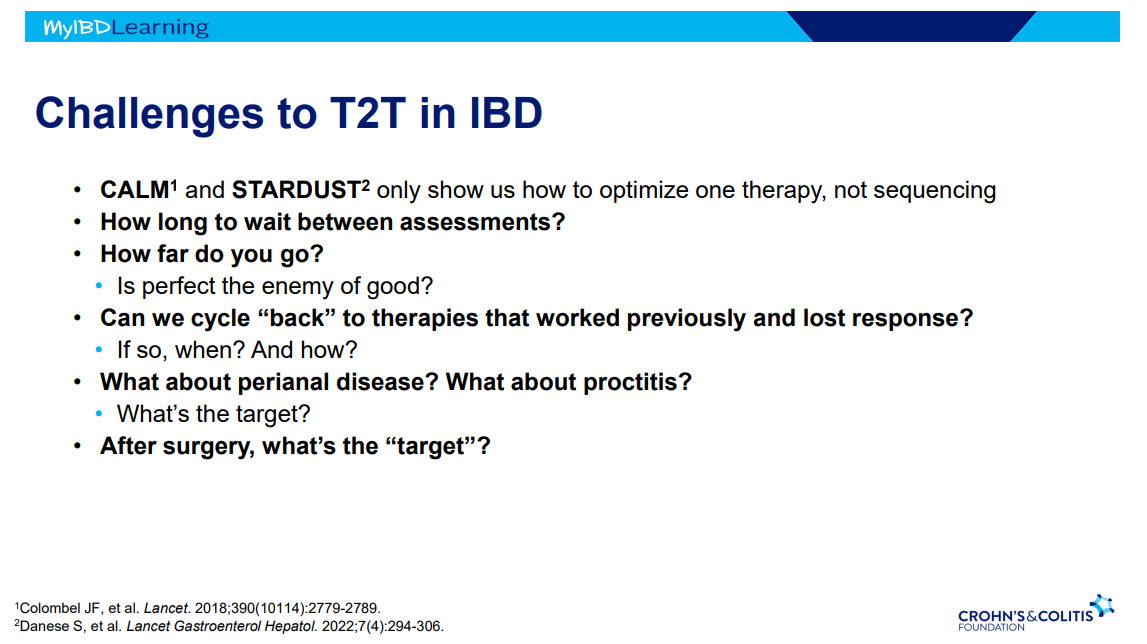
Many challenges in sequencing treatment -heterogeneity of diseases, loss of response, challenges in interpreting data, understudied issues (perianal disease, extra-intestinal manifestations, psychological health).
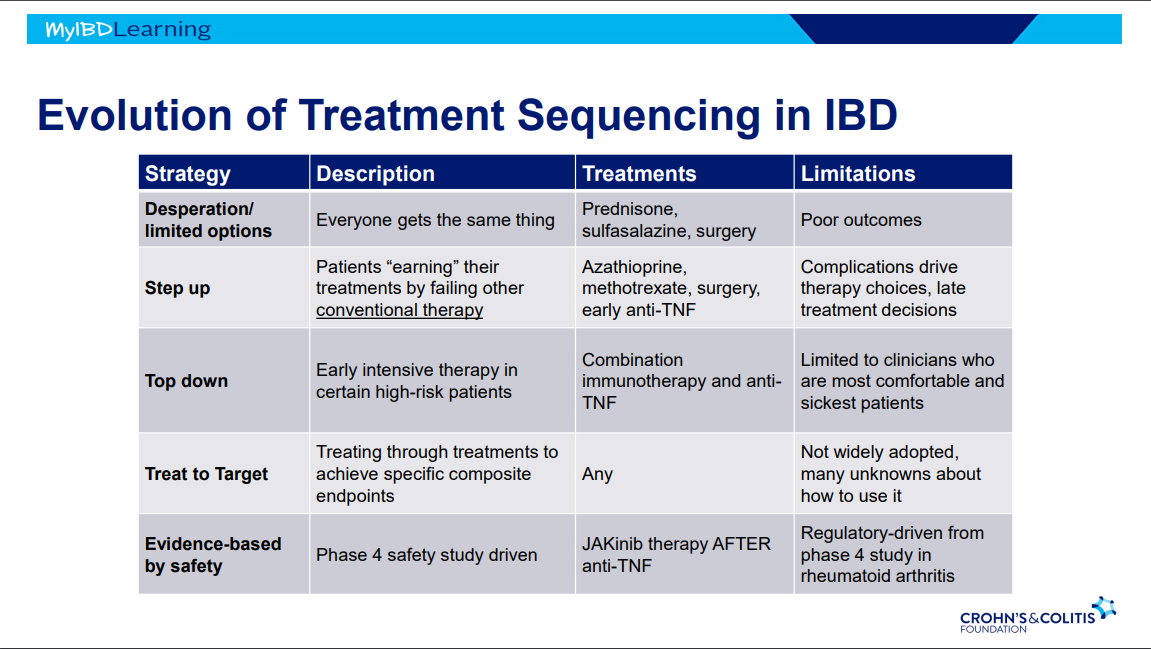
Evolution of therapies: desperation era -limited options, step up era, top down era with anti-TNFs, treat to target era and currently evidence-based by safety era.
It is possible to avoid steroids in many patients with upcoming plans to use an advanced therapy -this is probably beneficial. This may result in patients remaining symptomatic until these therapies can be started.
JAK inhibitors cannot be given as first-line agent in U.S. (but is done in other countries).
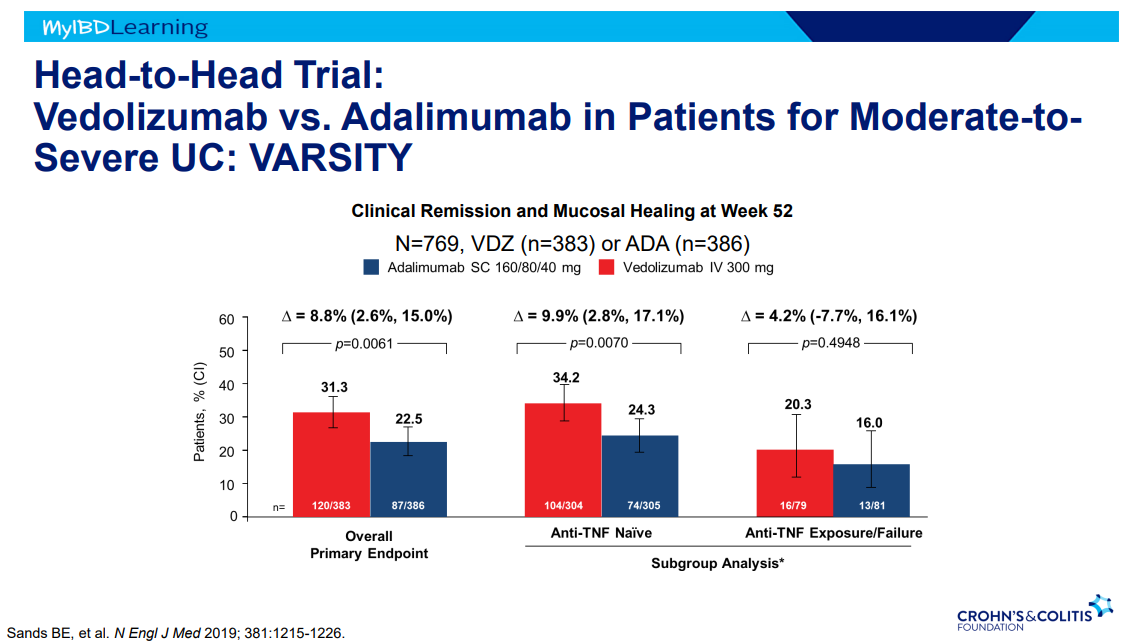
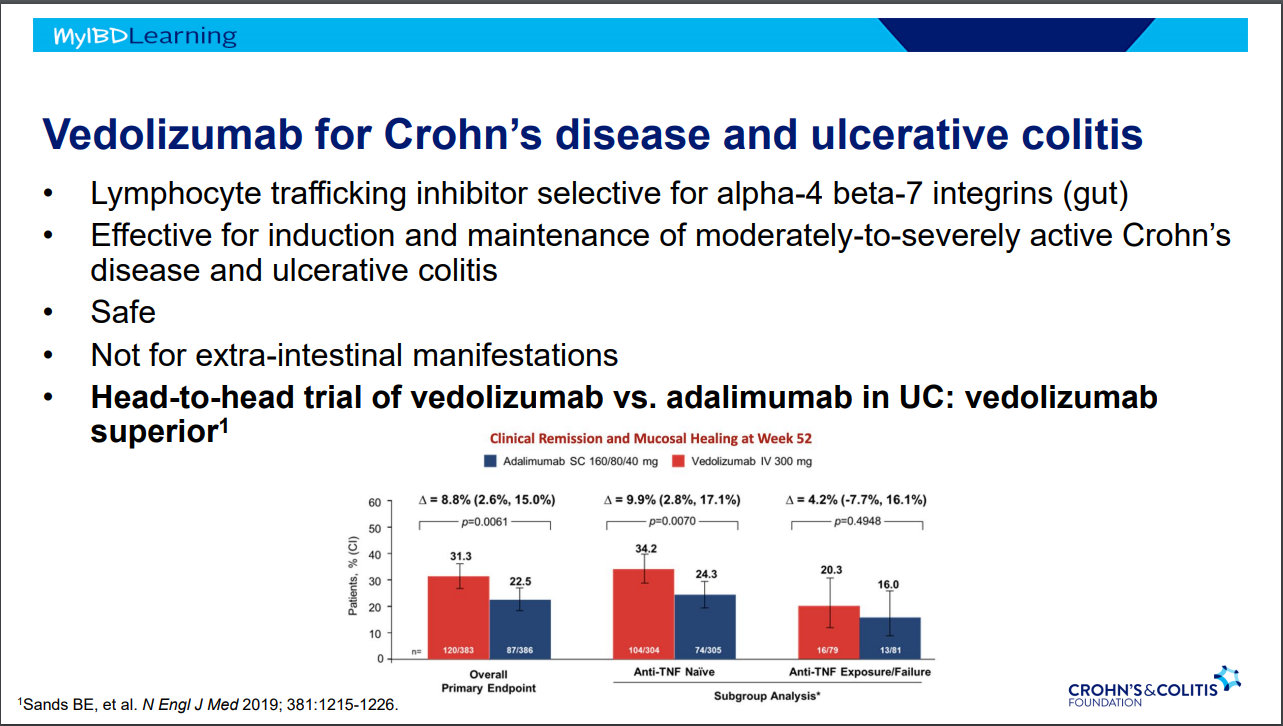
VARSITY trial enrolled patients with prior anti-TNF exposure (but not adalimumab) which biased the study against adalimumab vs vedolizumab
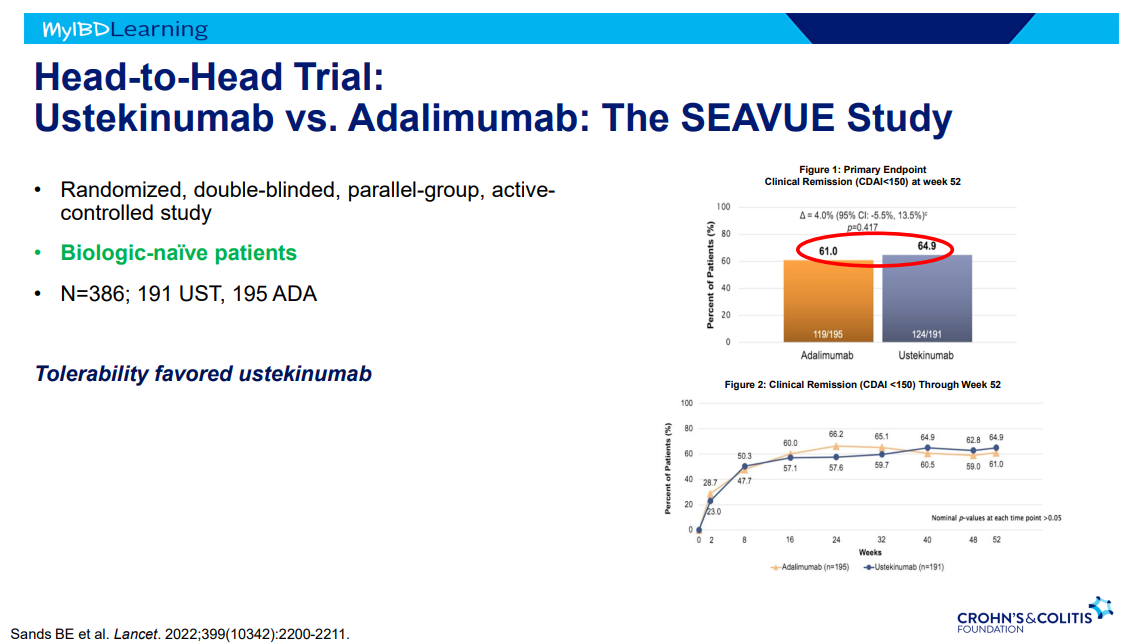
SEAVUE study ~65% in clinical remission at 1 yr with both adalimumab and ustekinumab; though, ustekinumab had better tolerability
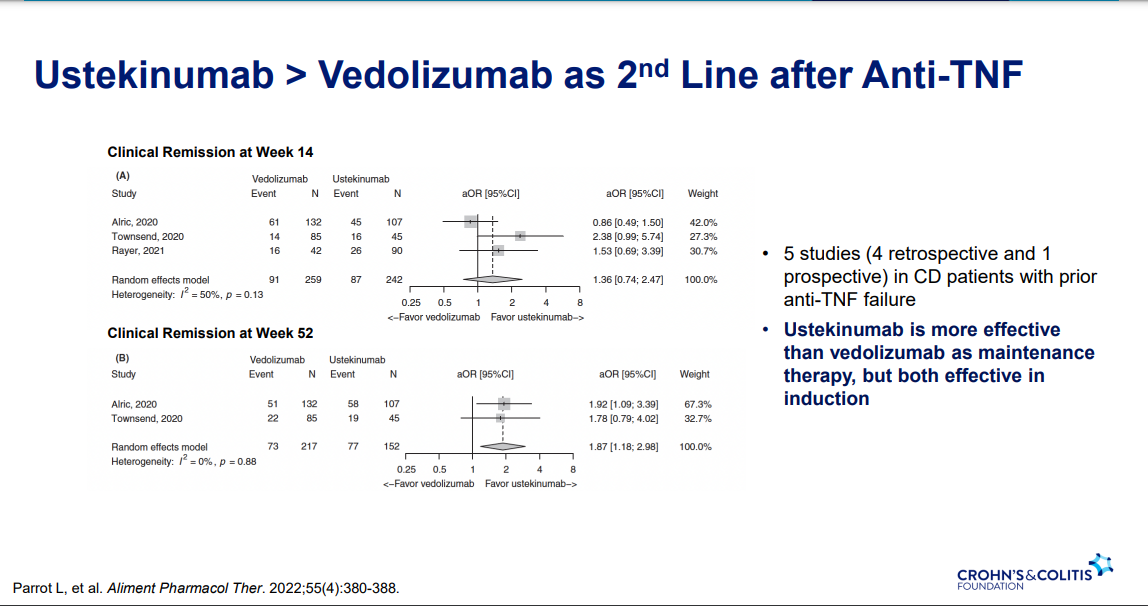
Ustekinumab better 2nd line treatment for CD after anti-TNF (Parrot et al. AP&T 2022; 55: 380-388
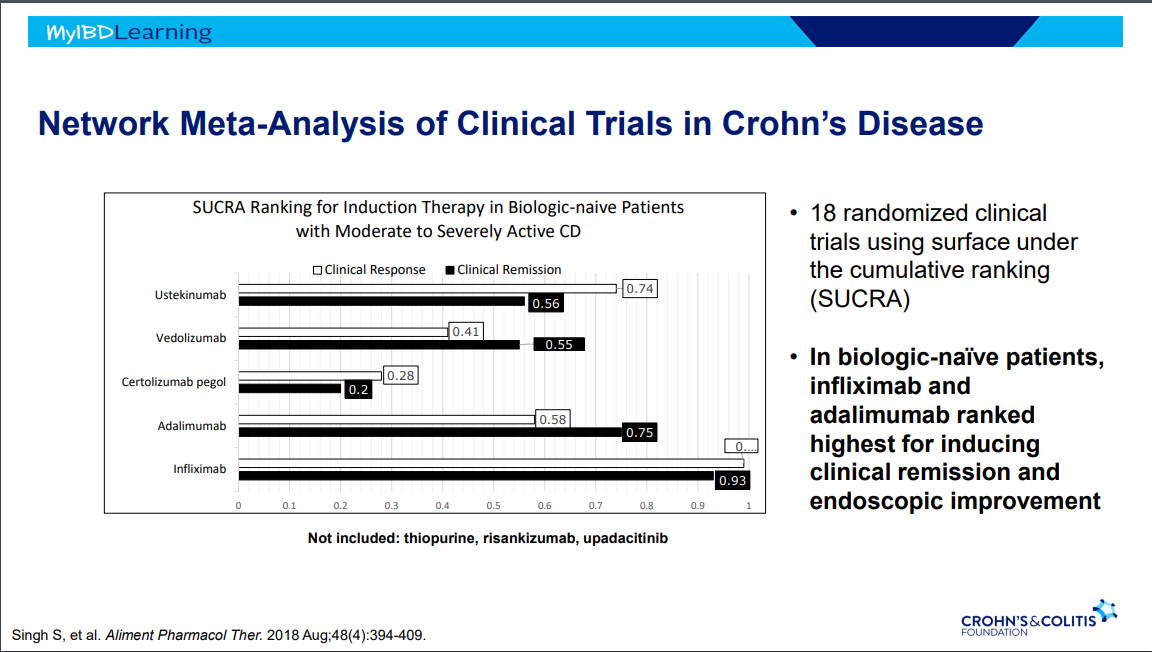
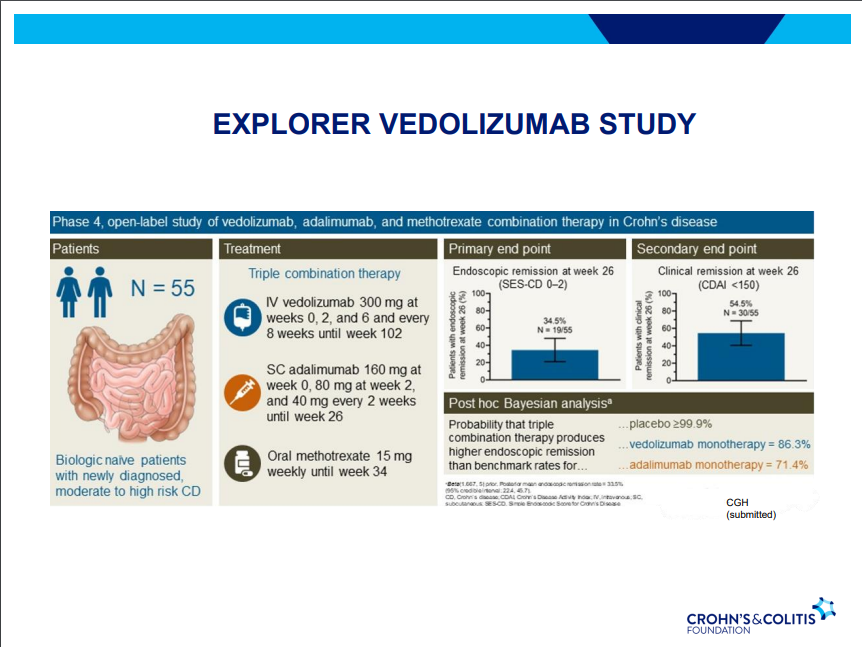
Vedolizumab is a good therapy for CD, especially in biologically-naïve
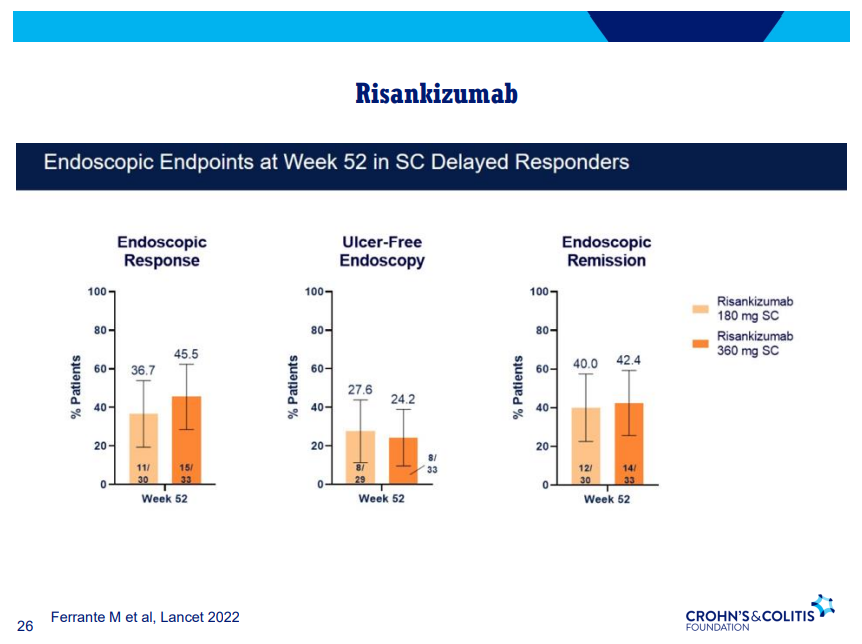
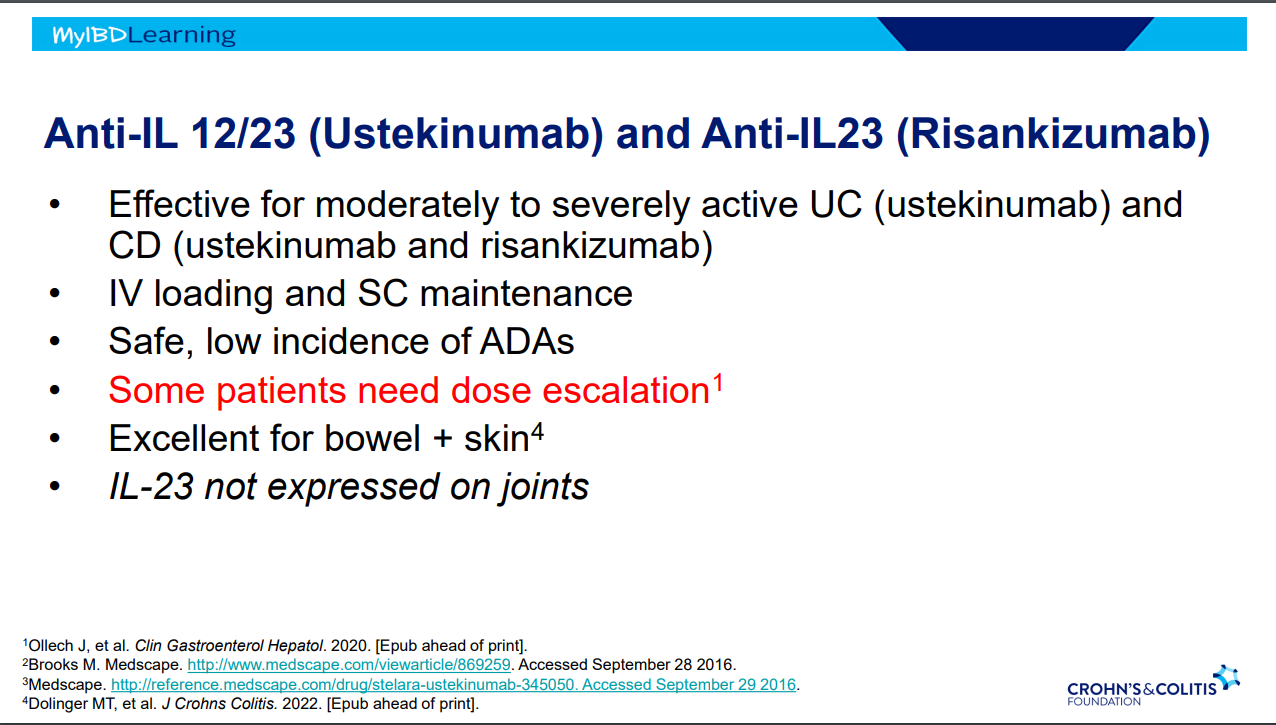
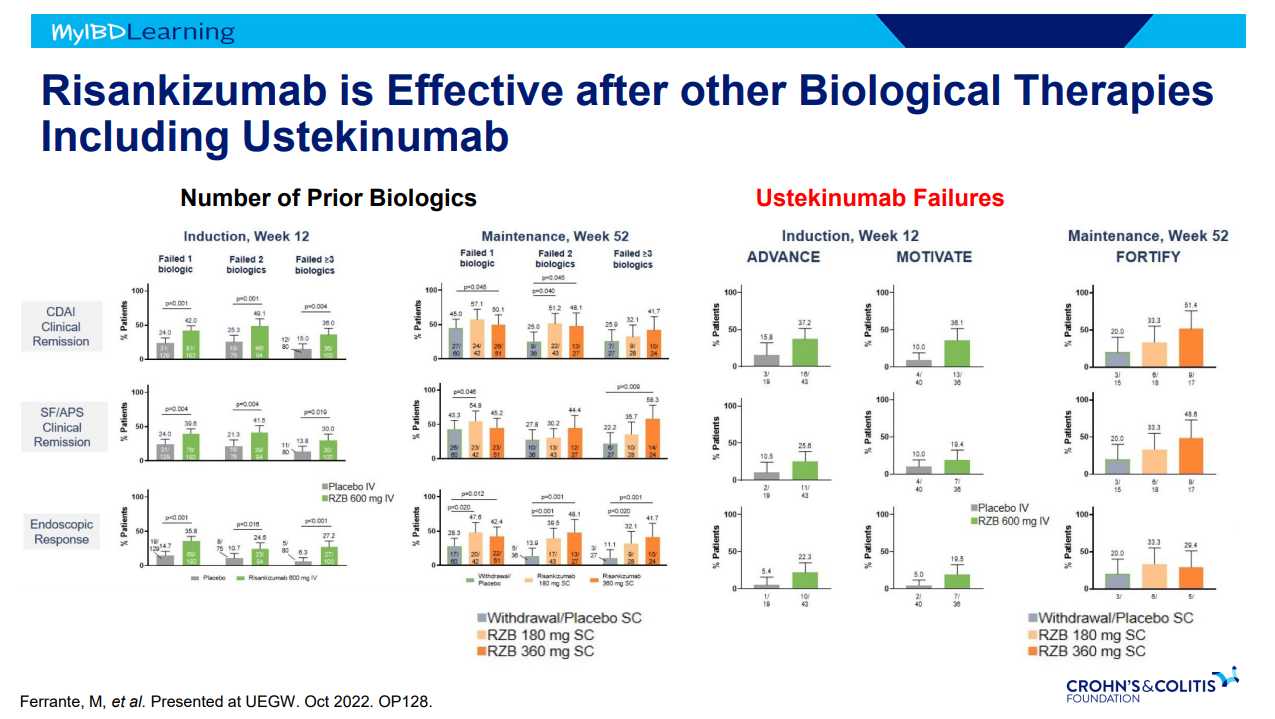
Risankizumab good for moderate-severe CD both in biologically-naïve and biologically-experienced
Dose reduction in maintenance of Jak inhibitors can result in LOR and 50-75% can achieve response after resumption of higher dosing
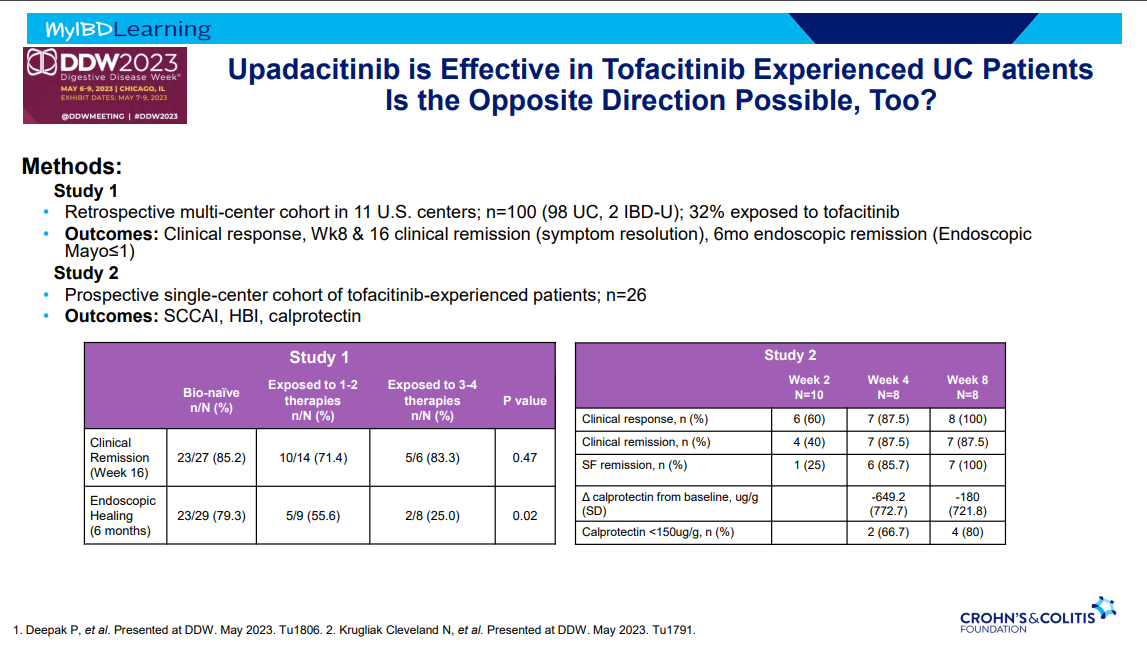
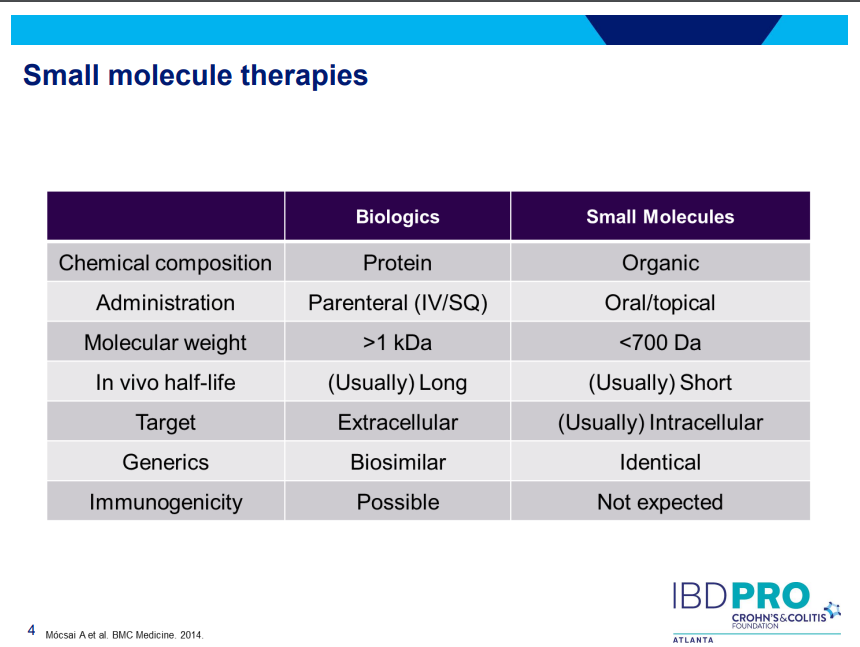
This is third day summarizing some of the talks at the regional CCFA conference. Erin Forster presented on Treatment with Oral Advanced Therapy. Below are my notes and some of the slides; my notes may have errors of omission or transcription. Can get access to full slide set: (n=22) here: Treatment with Oral Advanced Therapy
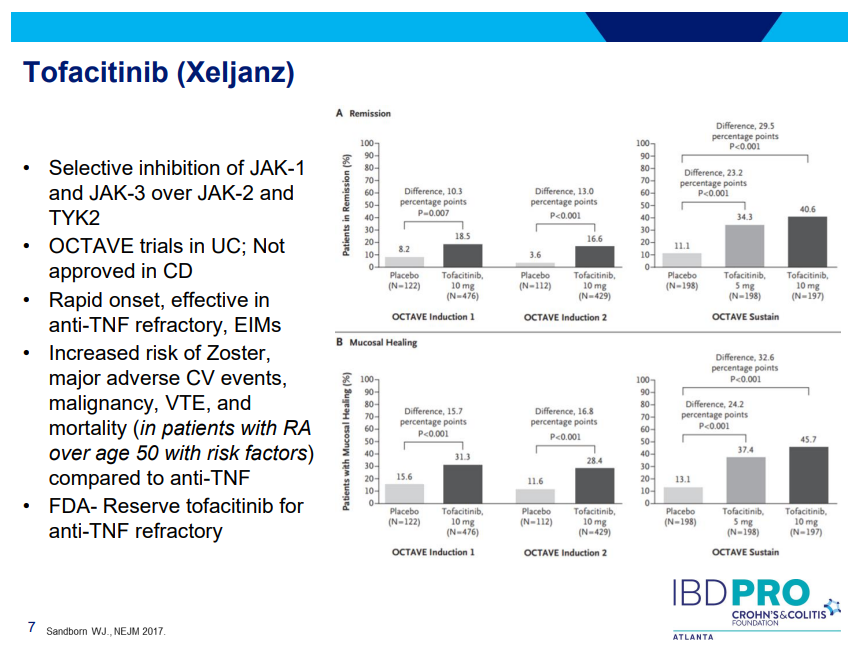
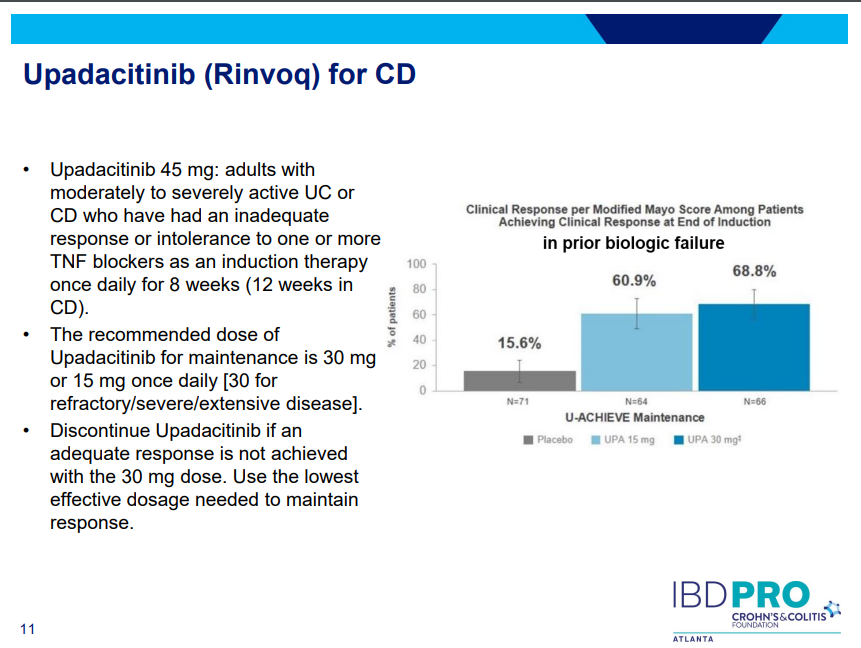
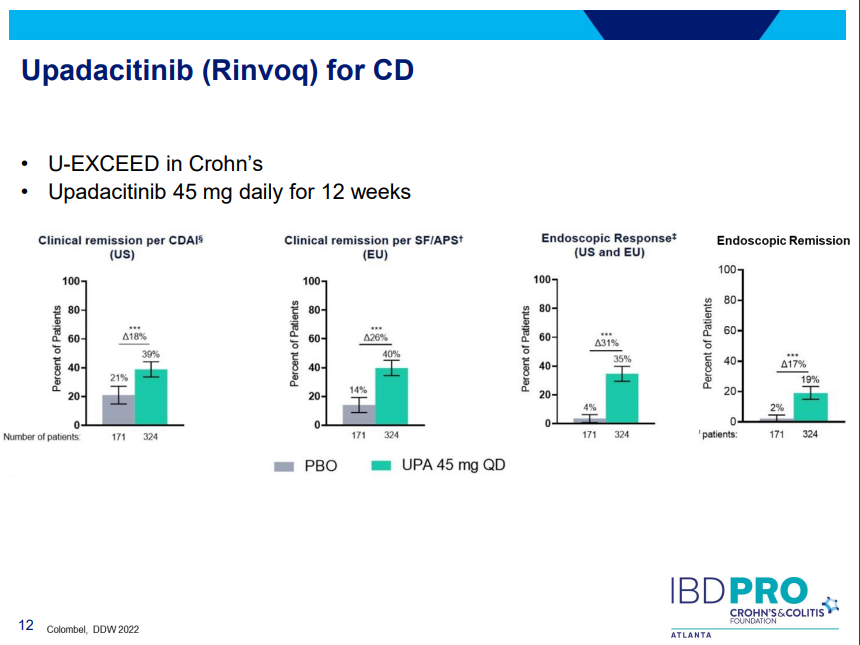
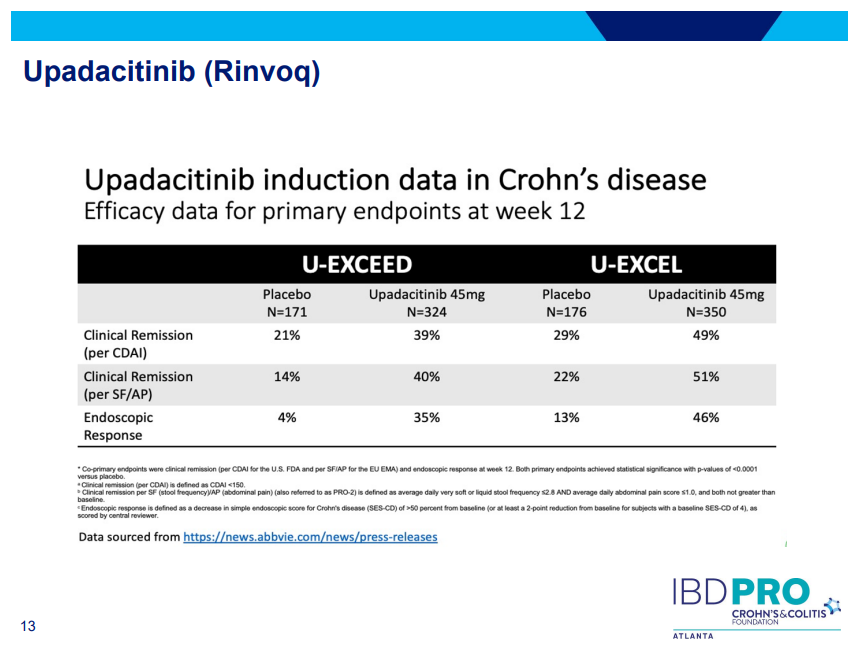
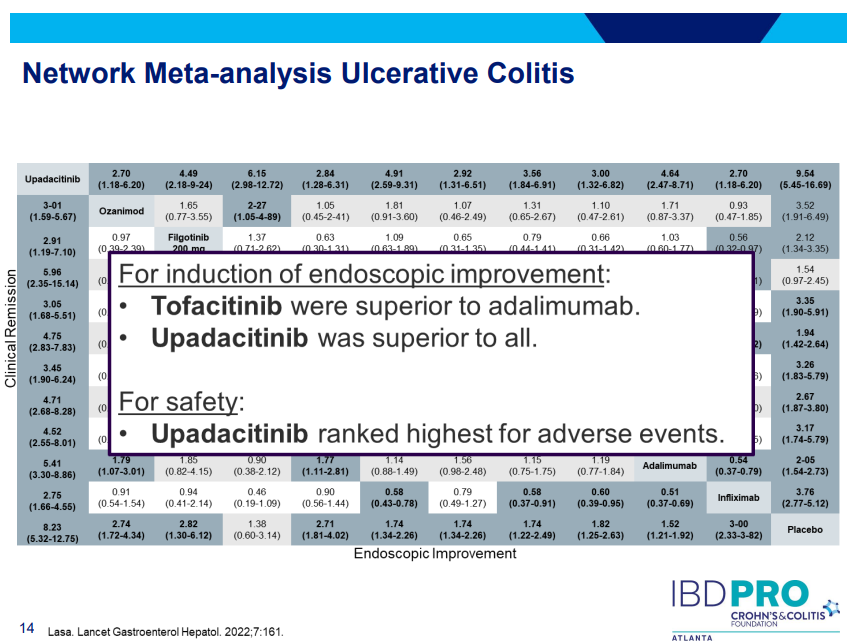
JAK inhibitors (Tofacitinib, Upadacitinib) have rapid onset of action and are taken orally
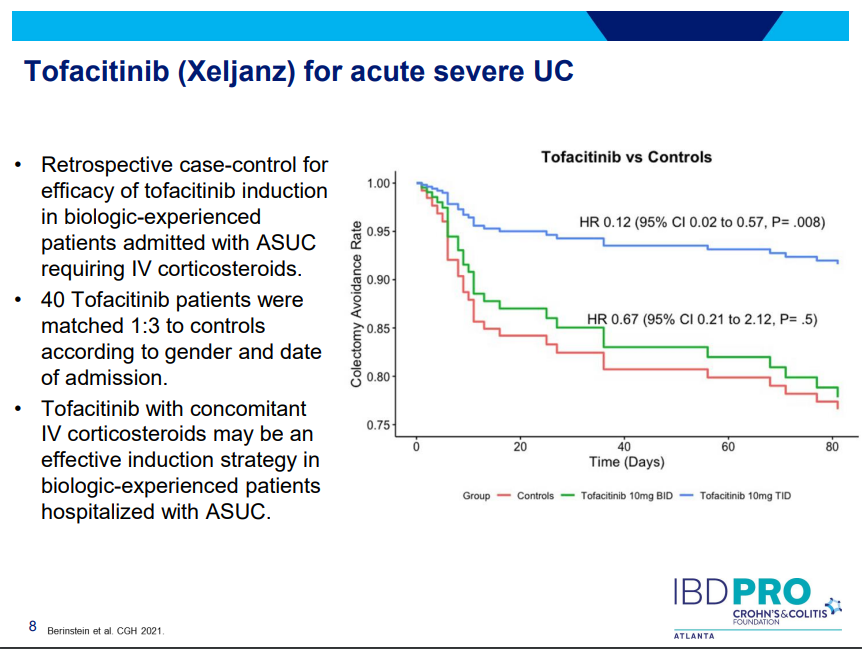
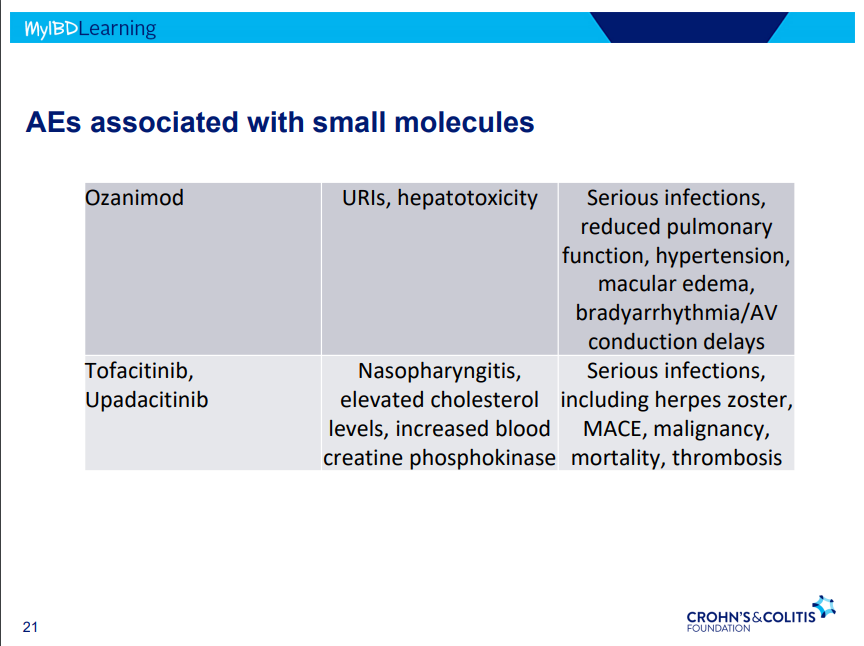
Tofacitinib (Xeljanz) -concern about cardiovascular events was derived from elderly rheumatologic patients. Cardiovascular events are rare. Higher dose (TID) (in the hospital) associated with lower colectomy rates in acute severe ulcerative colitis.
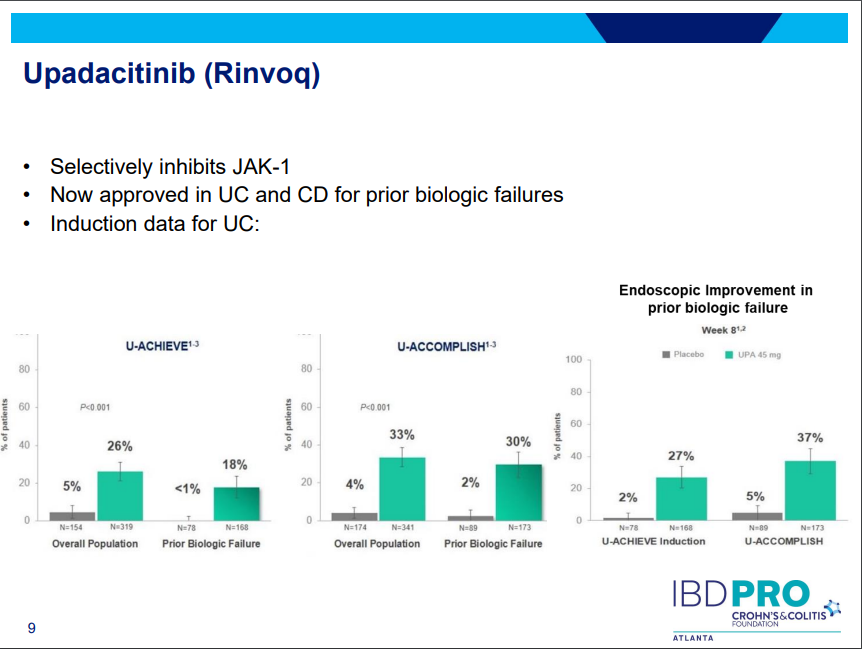
Upadacitinib (Rinvoq) -now approved for CD and UC. Higher dosing could affect liver function (especially if underlying liver disease). Also, JAK inhibitors as a class have similar safety concerns: increased herpes zoster and concerns for cardiovascular concerns (esp if >50 years)..
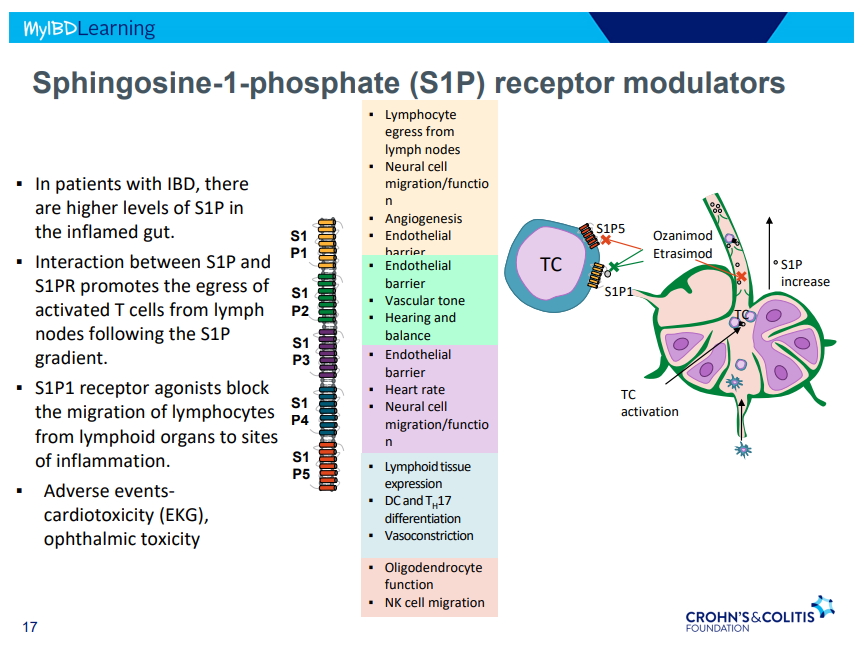
S!P receptor modulators: Oznaimod, Etrasimod & Amiselimod. Can cause bradycardia -have to check EKG prior.
There were a bunch useful lectures at CCFA 2023 regional conference in Atlanta. Here are some of my notes and slides from Doug Wolf‘s lecture; my notes may have errors of omission or transcription. Can get access to full slide set (n=37) here: Dose Escalation of Biologic Therapy and Dual Biologic Therapy
If loss of response to anti-TNF, consider dose escalation by either re-induction or increasing (doubling) dose. Re-induction is less costly
Dose escalation generally not effective for vedolizumab
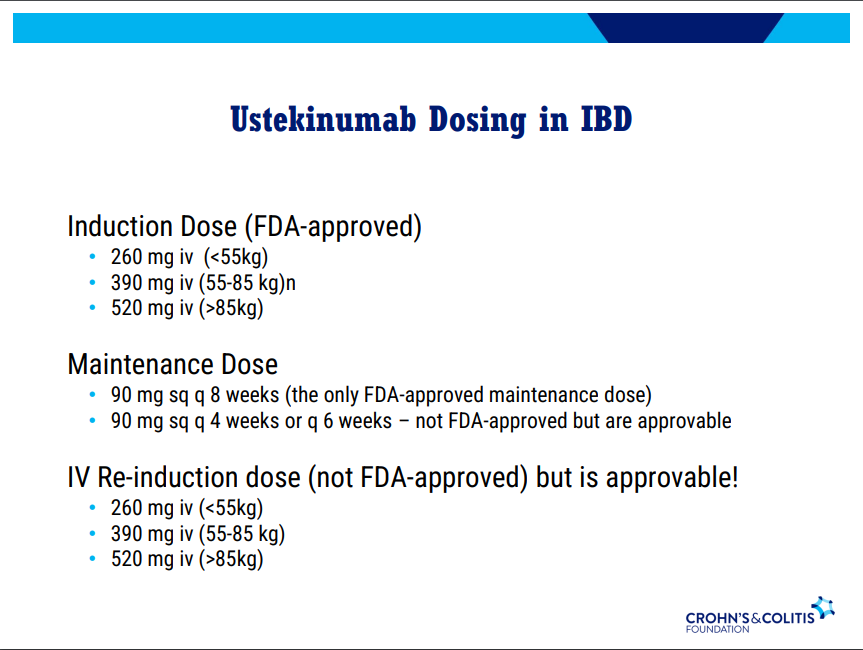
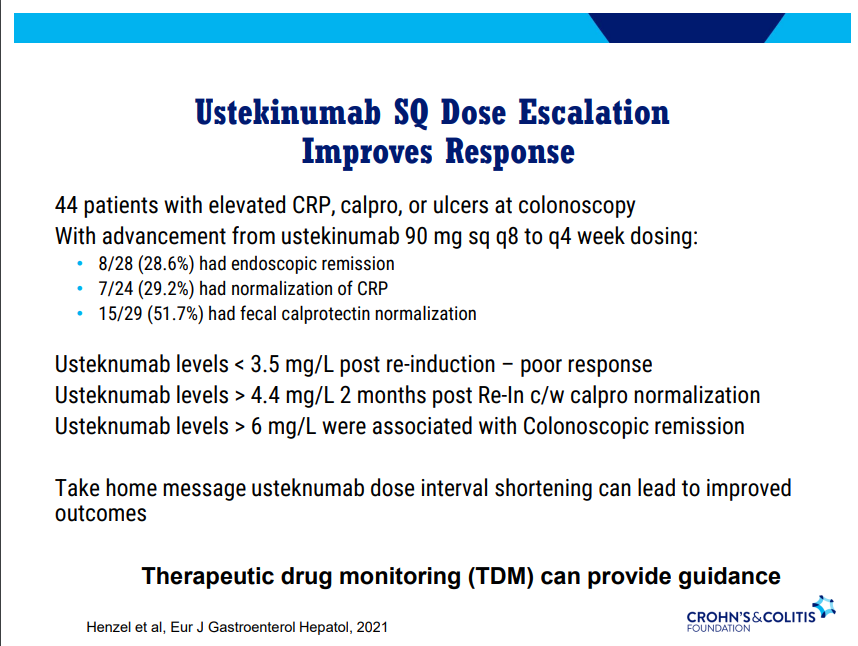
Dose escalation (increased frequency) with ustekinumab can be effective. Therapeutic drug monitoring can provide guidance. Re-induction can also be effective in half of patients (especially in patients with either no prior biologics or one prior biologic)
Risankizumab can still work in patients who had not responded by 12 weeks (delayed responders)
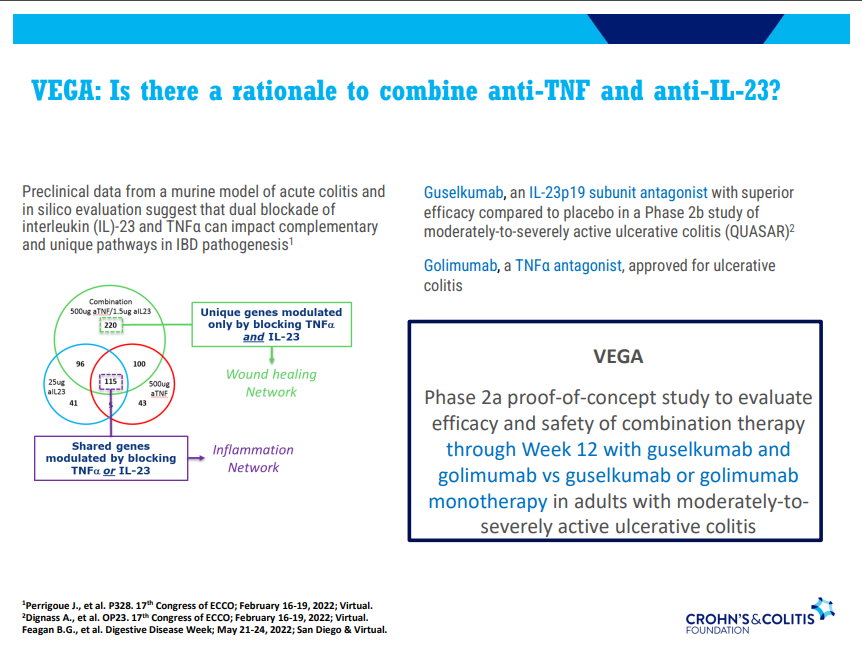
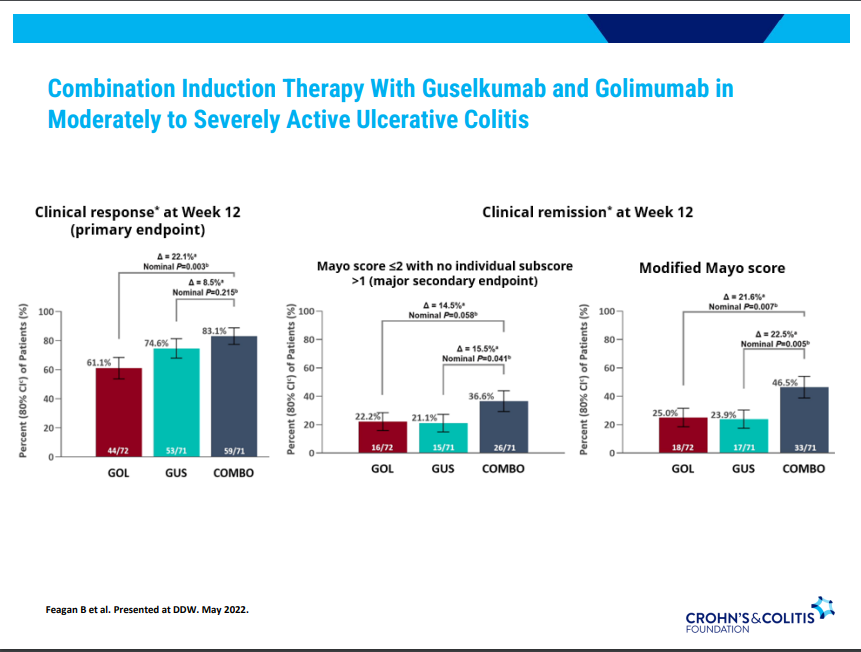
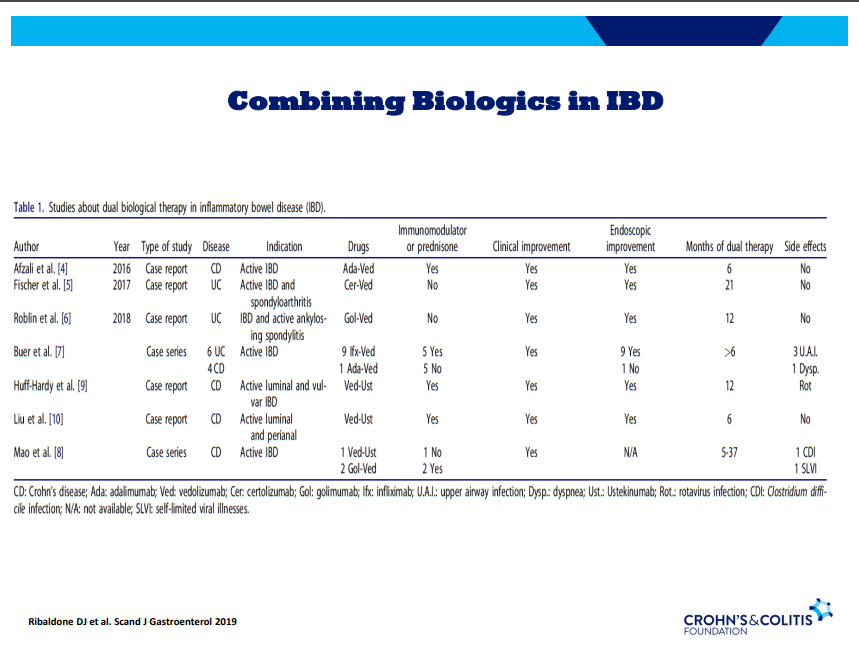
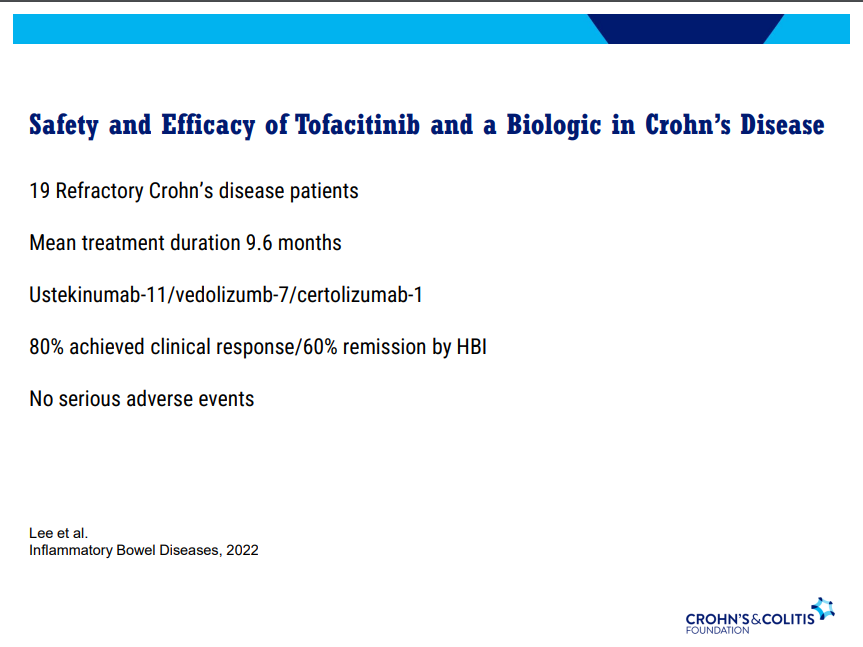
Discussed several combination treatments -no large studies thus far
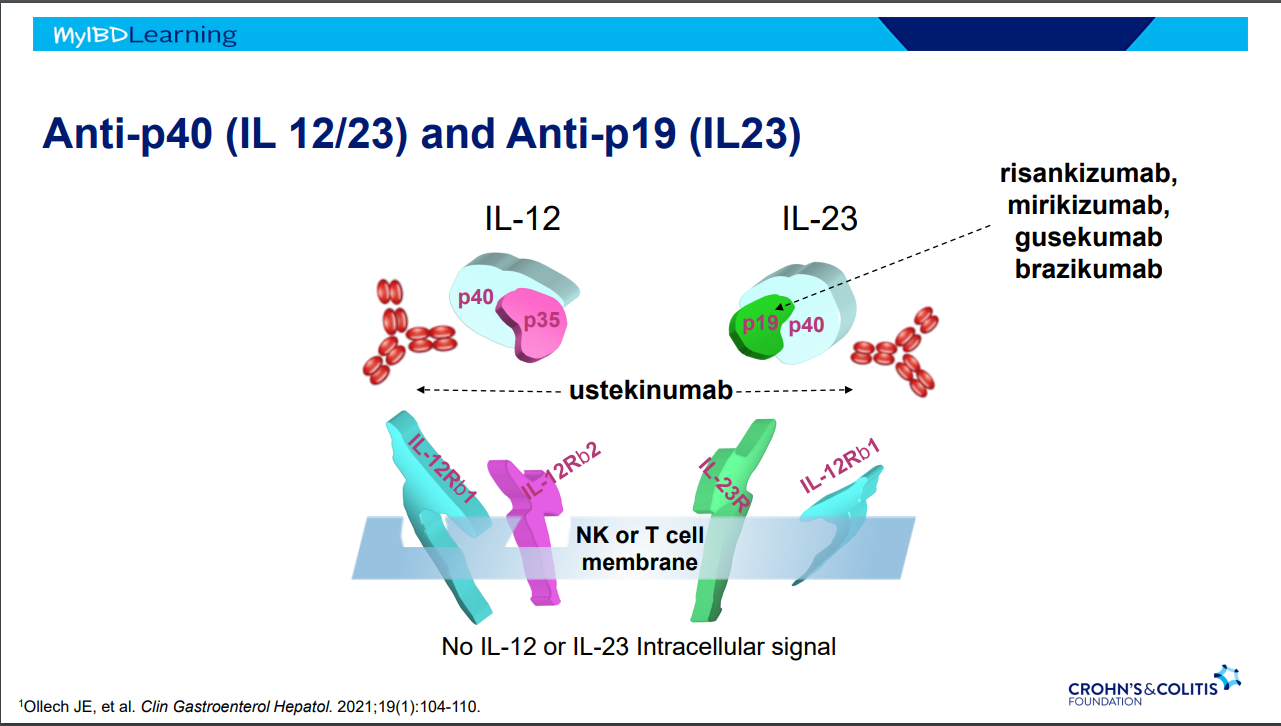
I recently attended a regional CCFA conference. David Rubin gave several terrific lectures. Here are some of my notes and some slides from this lecture. My notes may contain transcription errors as well as important omissions. Can get access to full set of slides here: Biologics and Their Biosimilars
“Biologics and Their Biosimilars“
What is a Biologic Therapy?
Dr. Rubin makes a point of explaining the term to patients. It is a protein made in a living cell that targets another protein. Term “biologic” can sound scary to patients. Usually given IV because they cannot be absorbed through the small bowel.
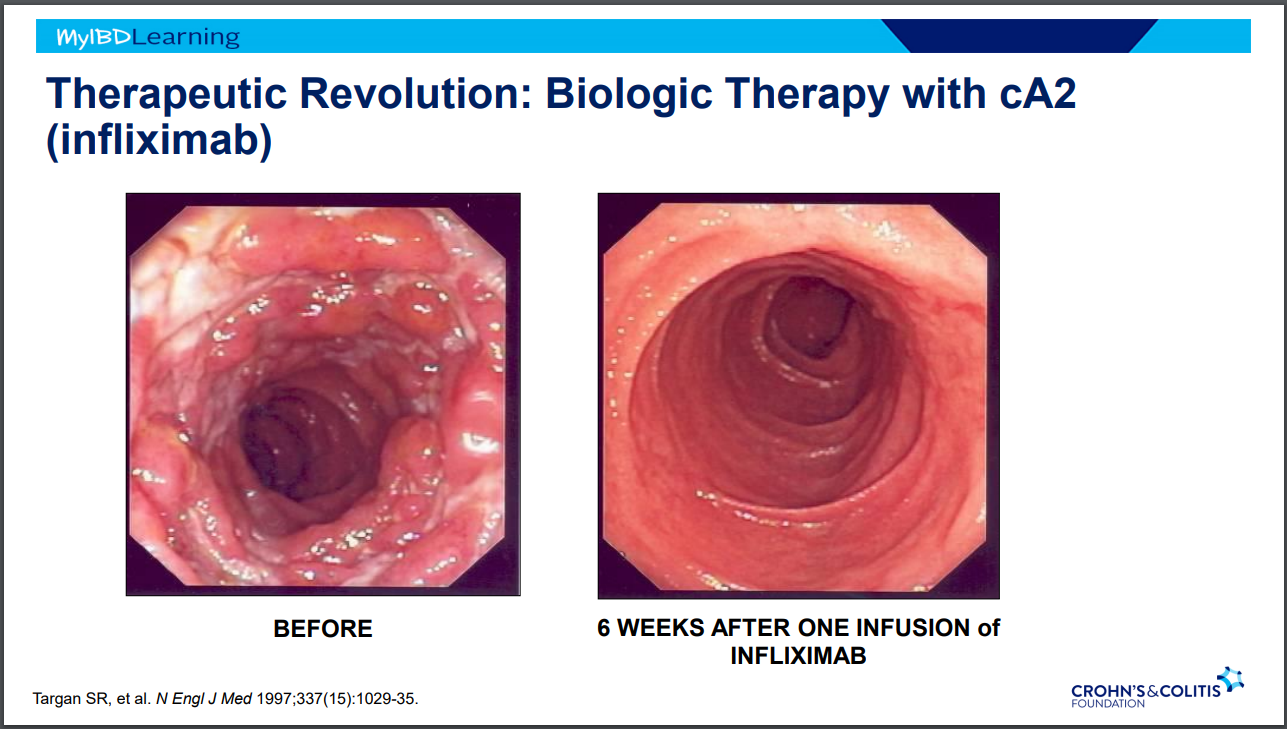
IBD Treatment Revolutions
Steroids -overnight changed mortality in IBD
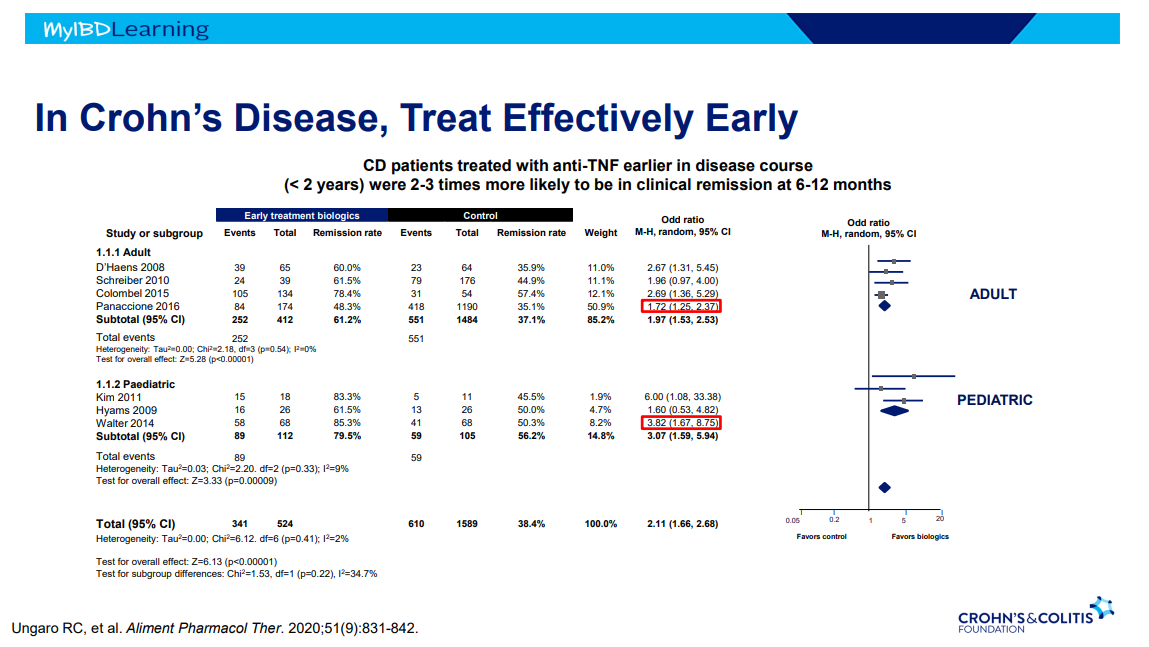
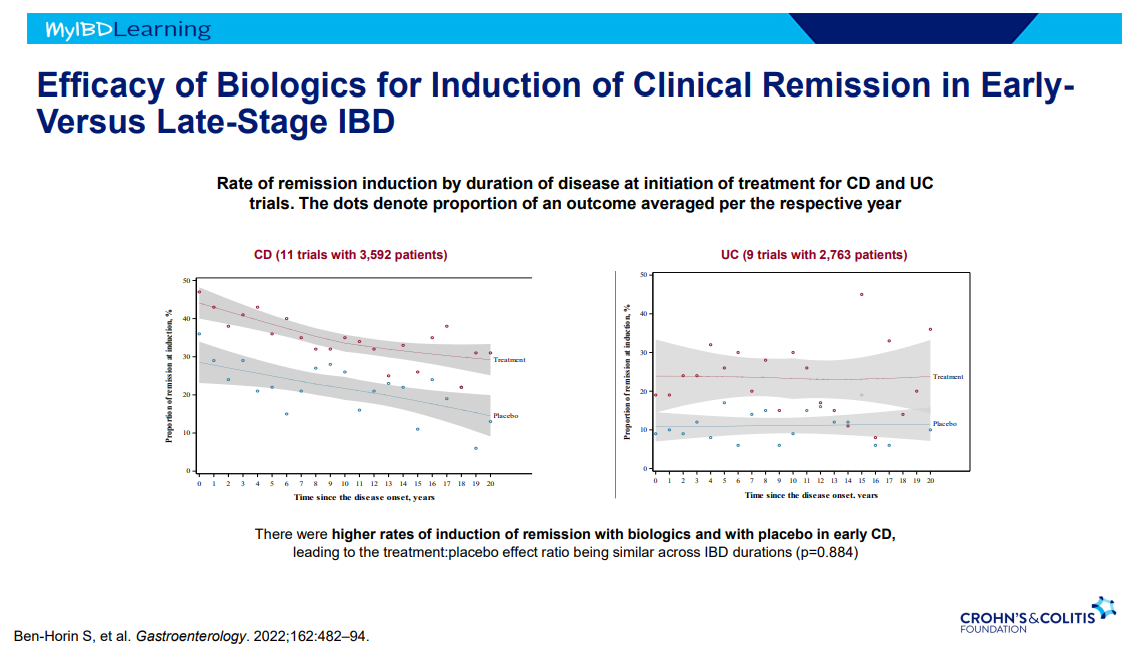
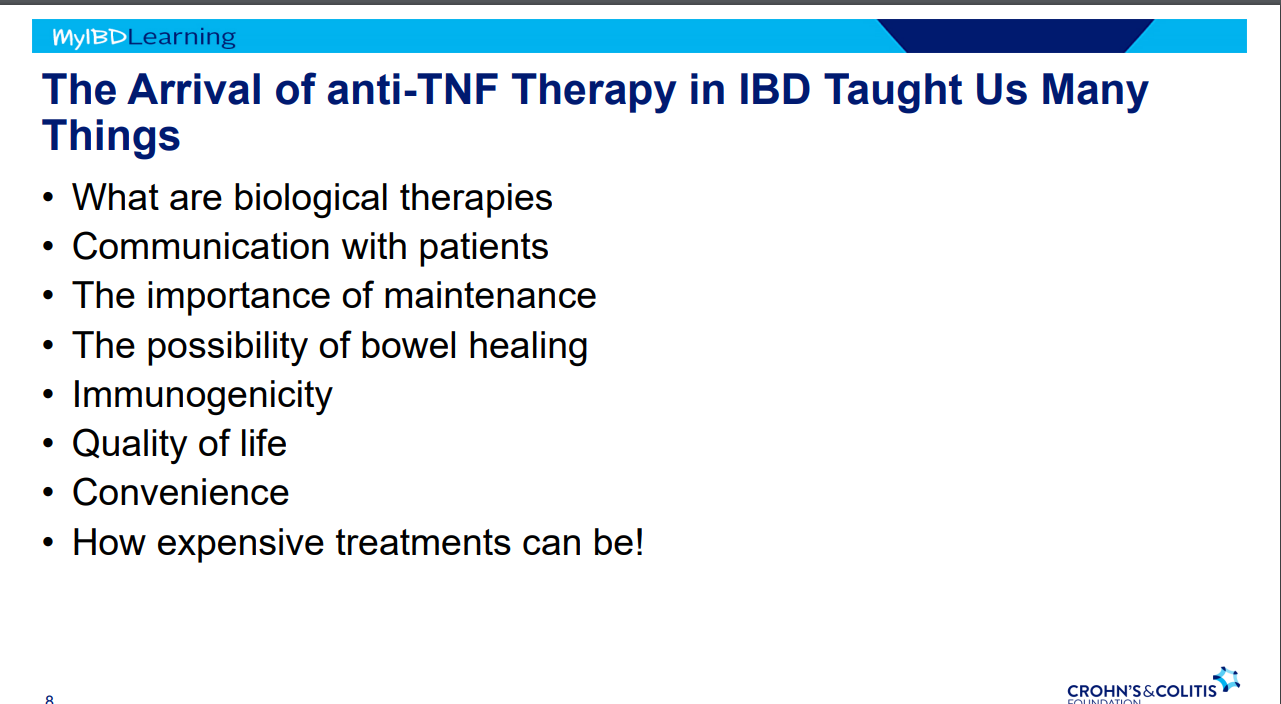
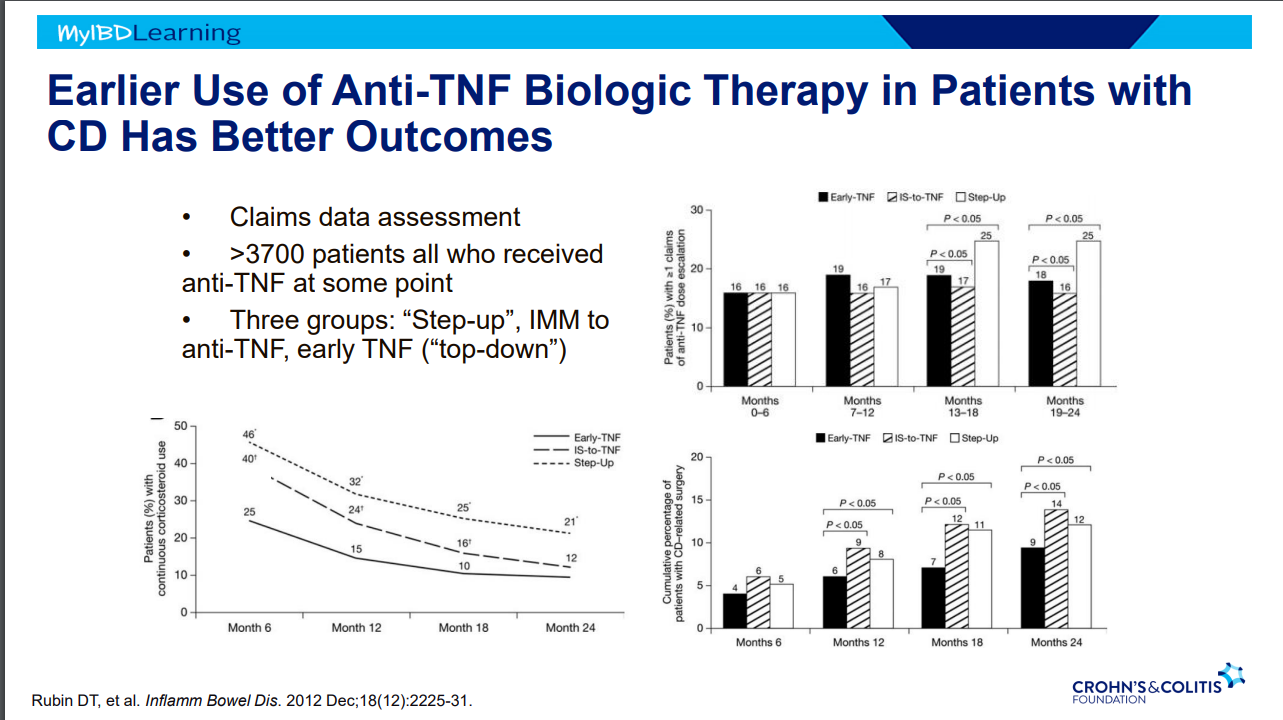
Anti-TNF Therapy in IBD -taught many lessons. Treat earlier –>better outcomes.
Anti-TNF Therapy
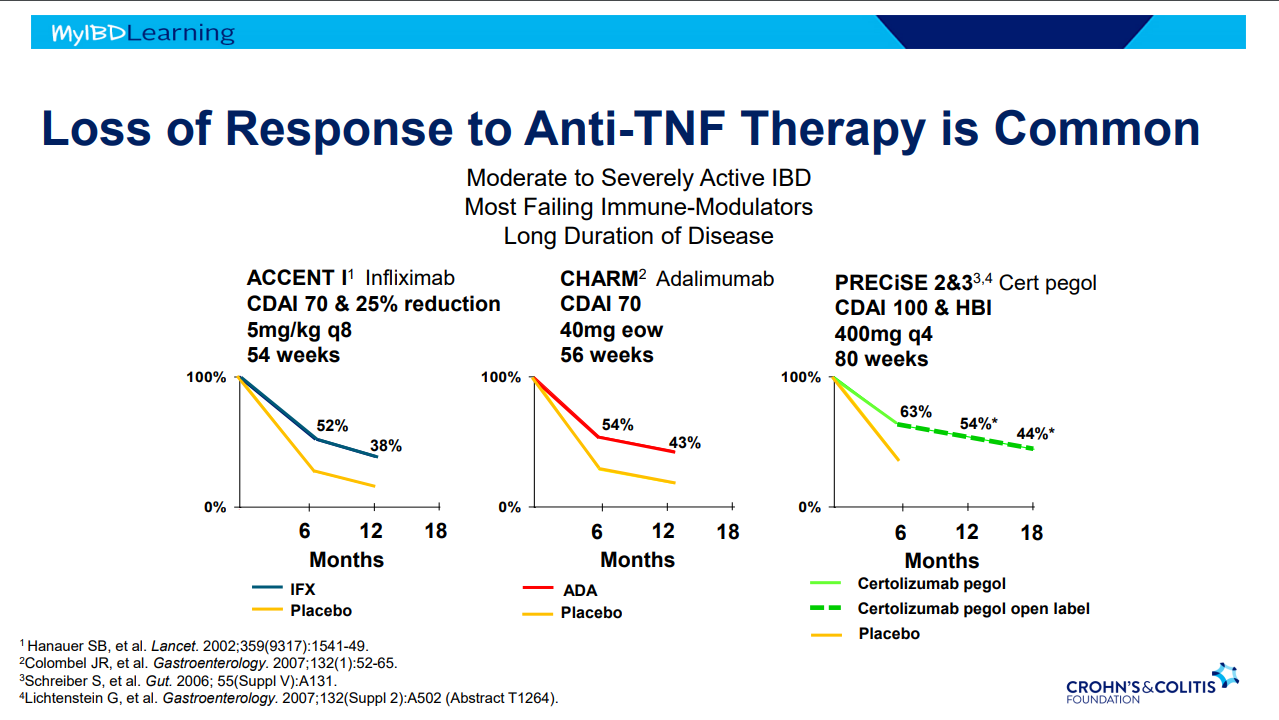
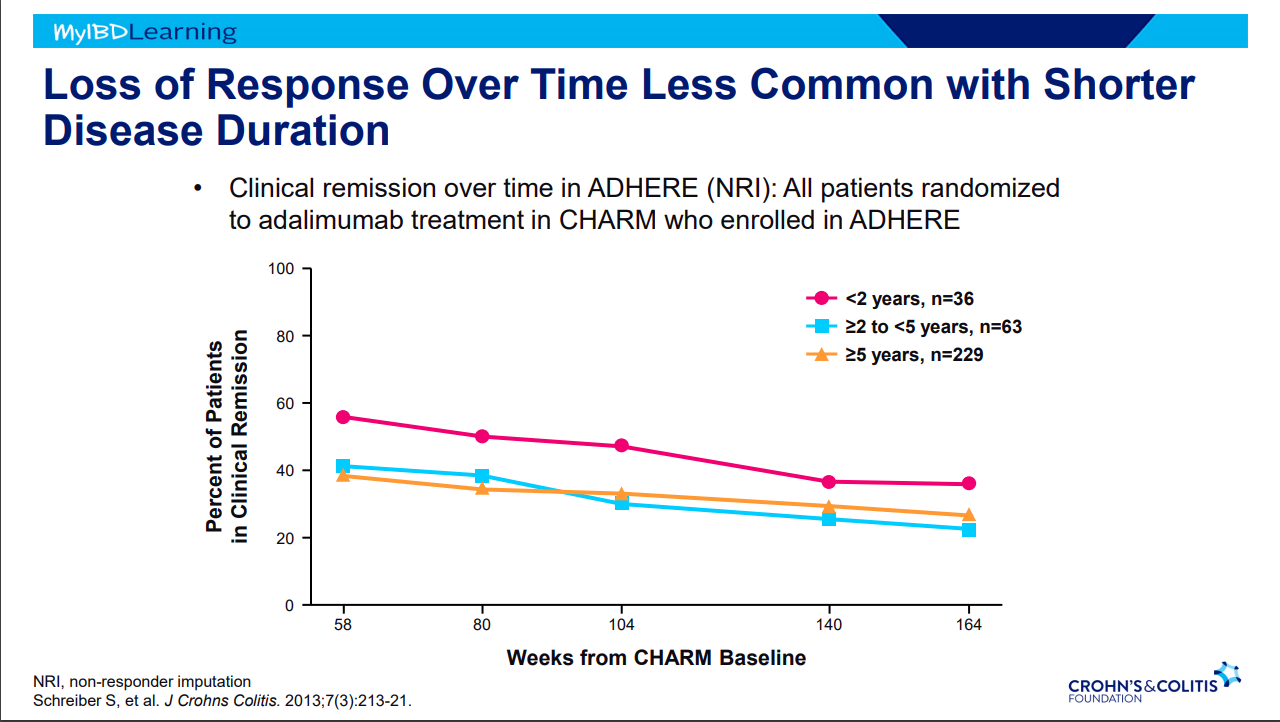
Frequent loss of response.
Earlier treatment with biologics result in better outcomes.
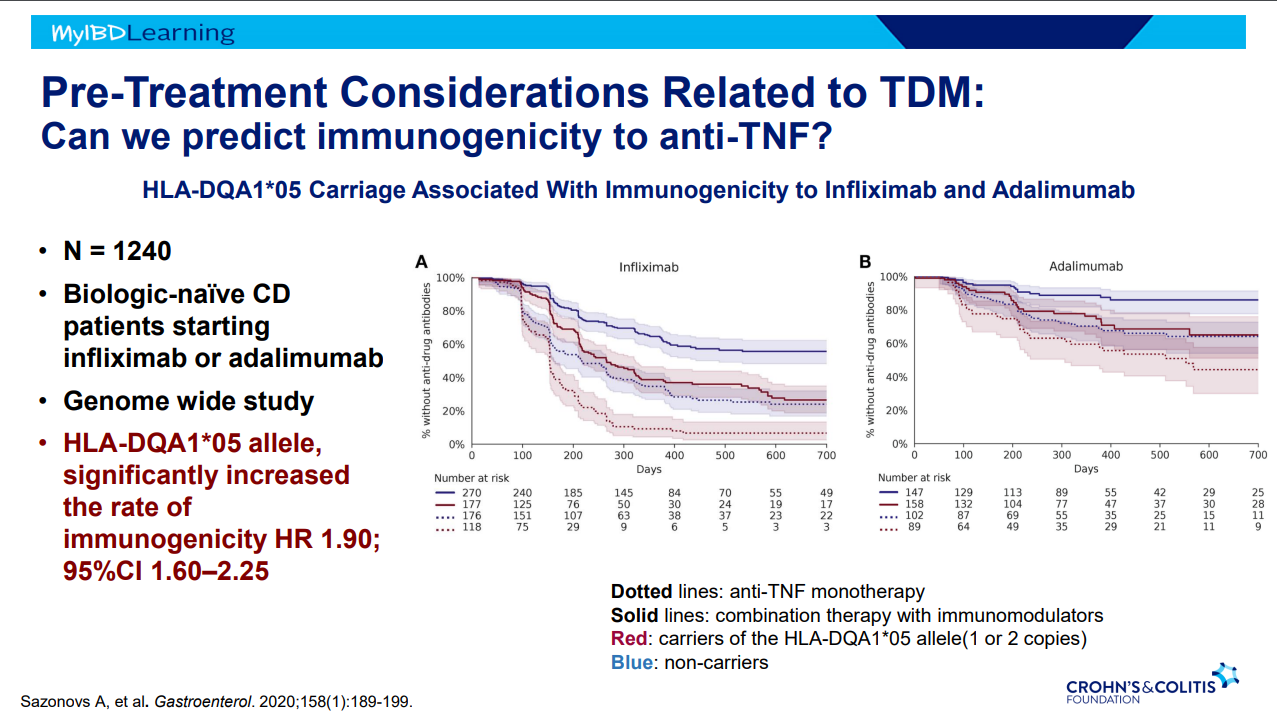
Immunogenicity is mainly an issue with anti-TNF agents and not much of an issue with other biologics. Episodic therapy is a big risk factor for anti-drug antibodies.
If staying with in-class medication, after anti-drug antibodies, need to take additional measures to prevent anti-drug antibodies (eg. Immunomodulators).
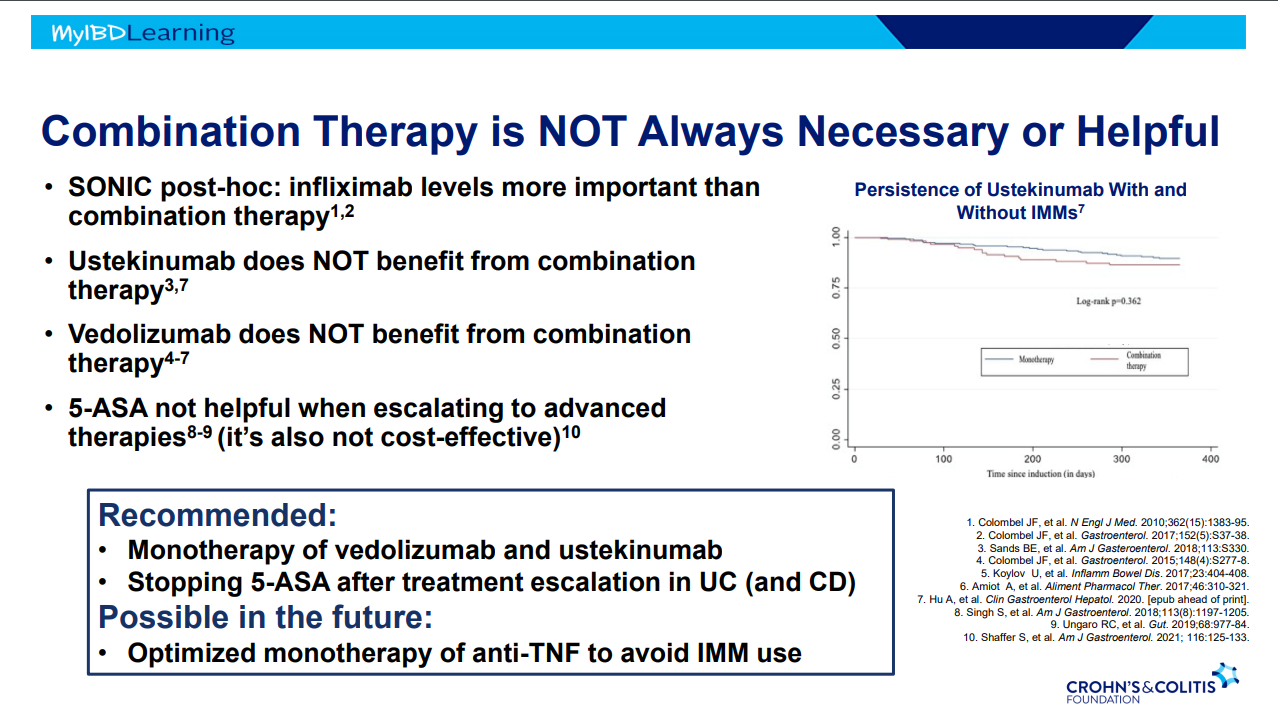
Combination therapy is more effective (SONIC, UC SUCCESS trials). This is due to using multiple mechanisms of disease control, reduction in anti-drug antibodies, and elevated serum drug levels.
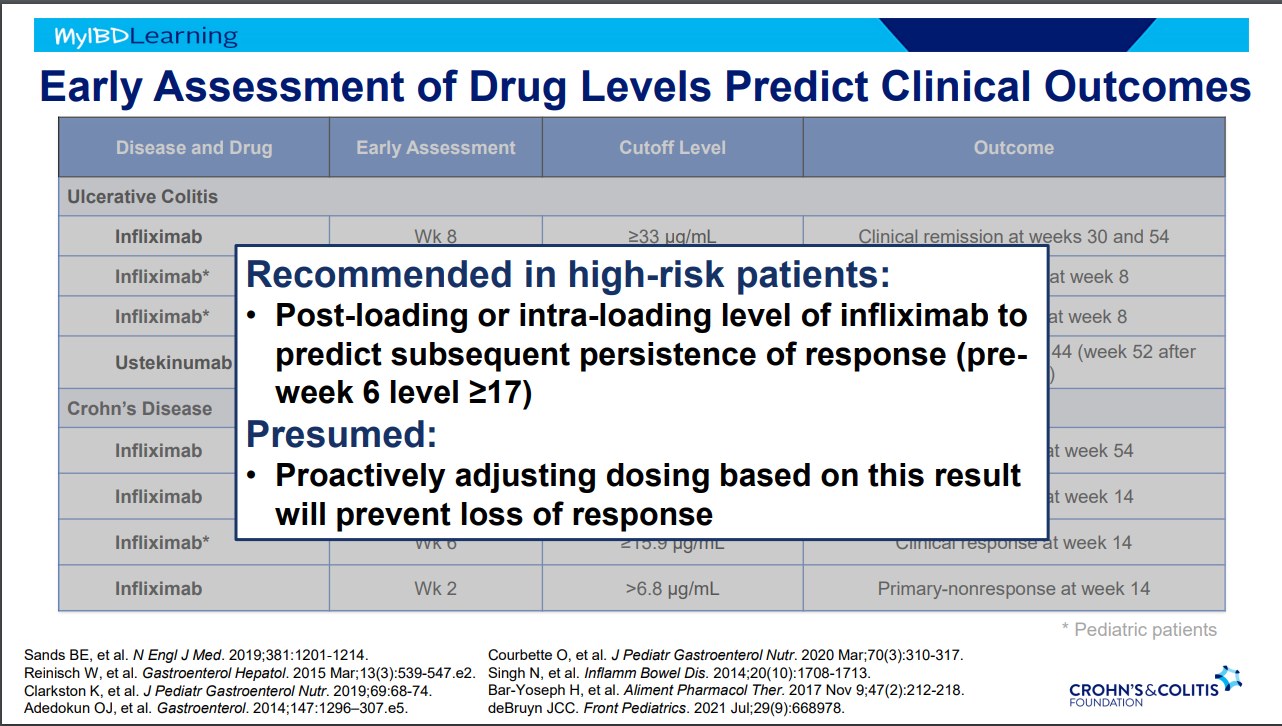
Good therapeutic levels appears to deliver similar results as combination therapy
Pre-week 6 level of 17 or greater, associated with good response in maintenance. If level is low, presumption is that higher dosing will be beneficial.
Higher levels of infliximab trough levels needed for perianal fistula healing (improved with ciprofloxacin). Higher levels could be causally-related to healing or could be a marker that there is less inflammation and a patient is responding.
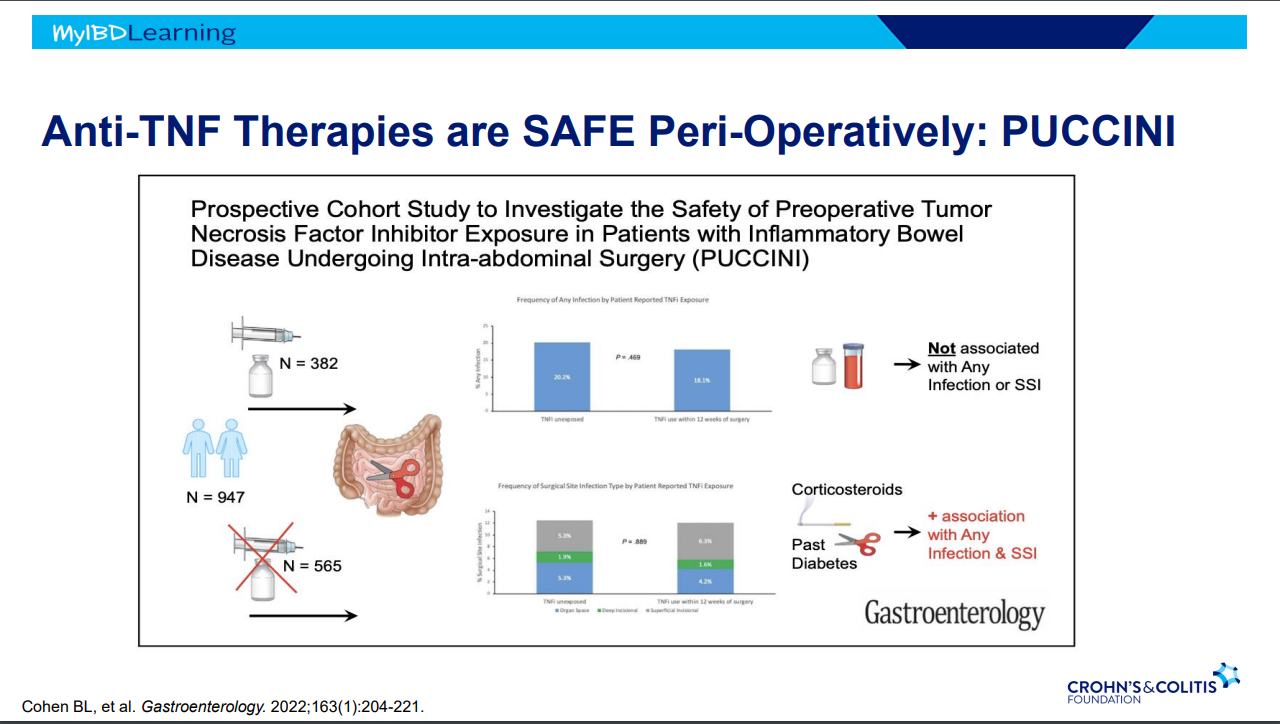
Anti-TNFs do not appear to increase risk of infections (see PUCCINI study)
Vedolizumab -terrific safety profile. No PML, no malignancy risk
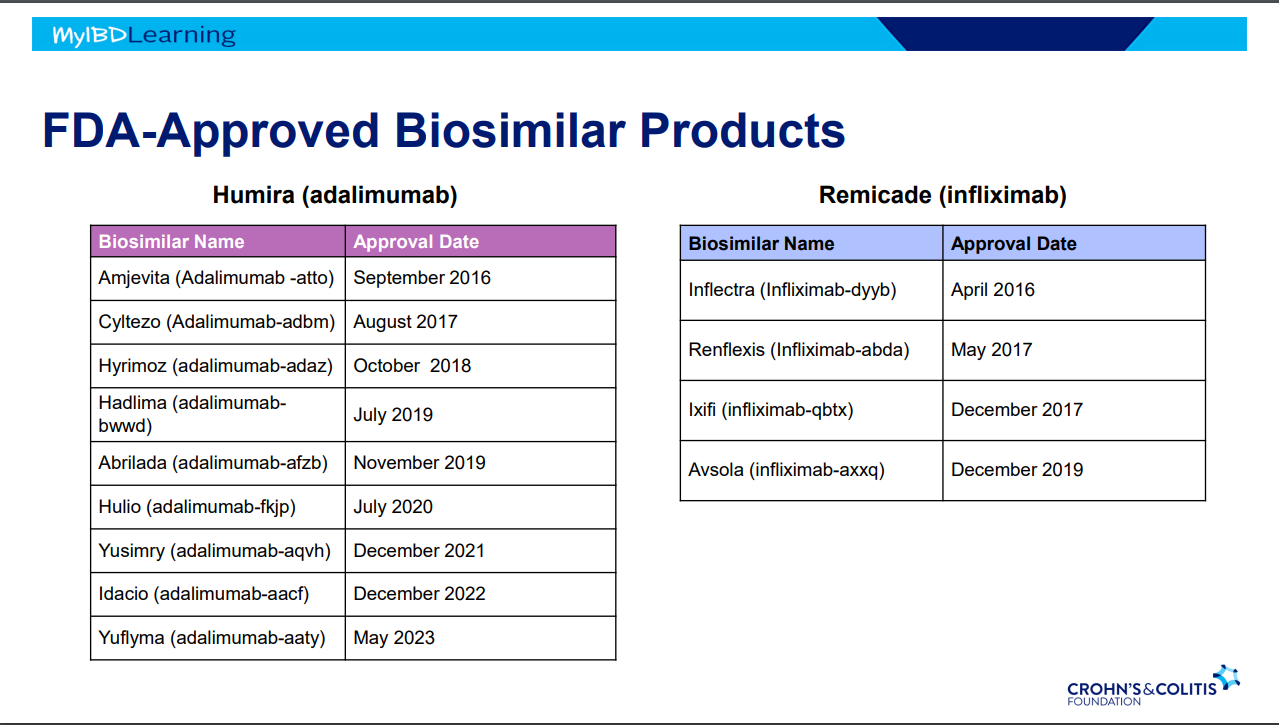
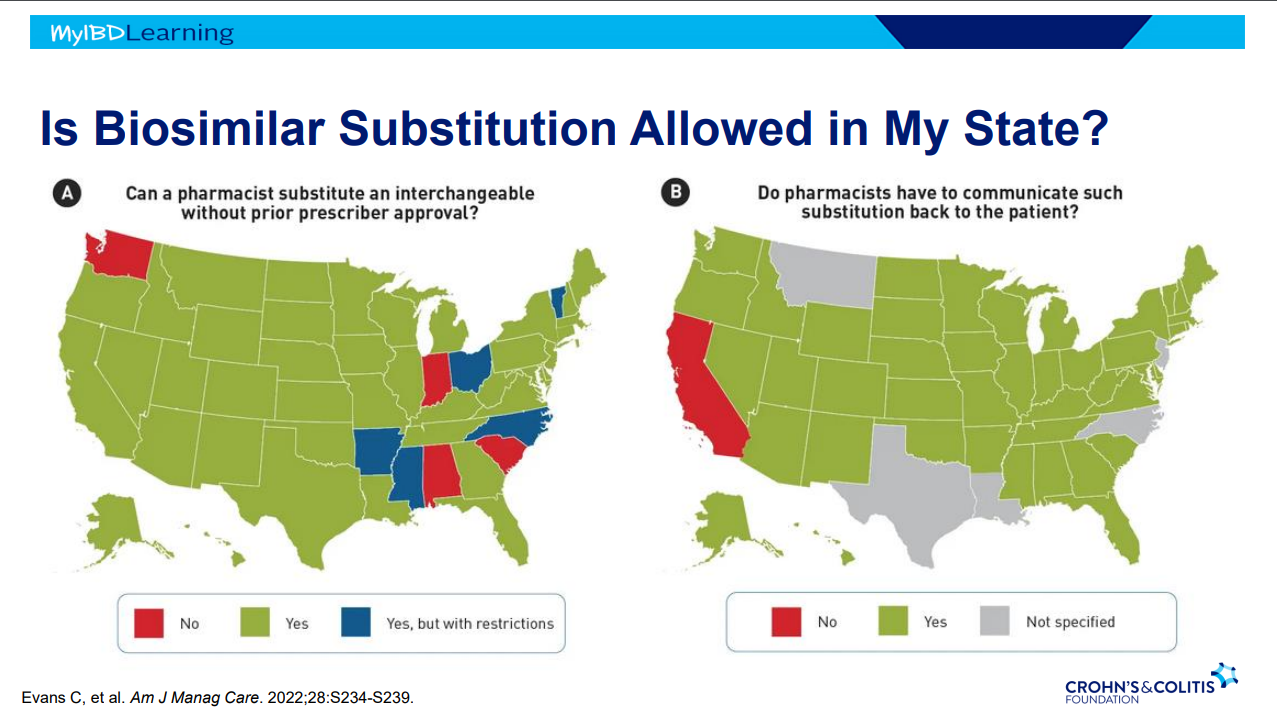
Biosimilars:
If biosimilar found effective for one approved condition, extrapolation given to all indications
IBD switching studies have NOT shown increased loss of response. Consider reassess prior to switch to help determine if patient truly in remission prior to switch. Switching often blamed for loss of response when many times the disease was not under good control prior to switch
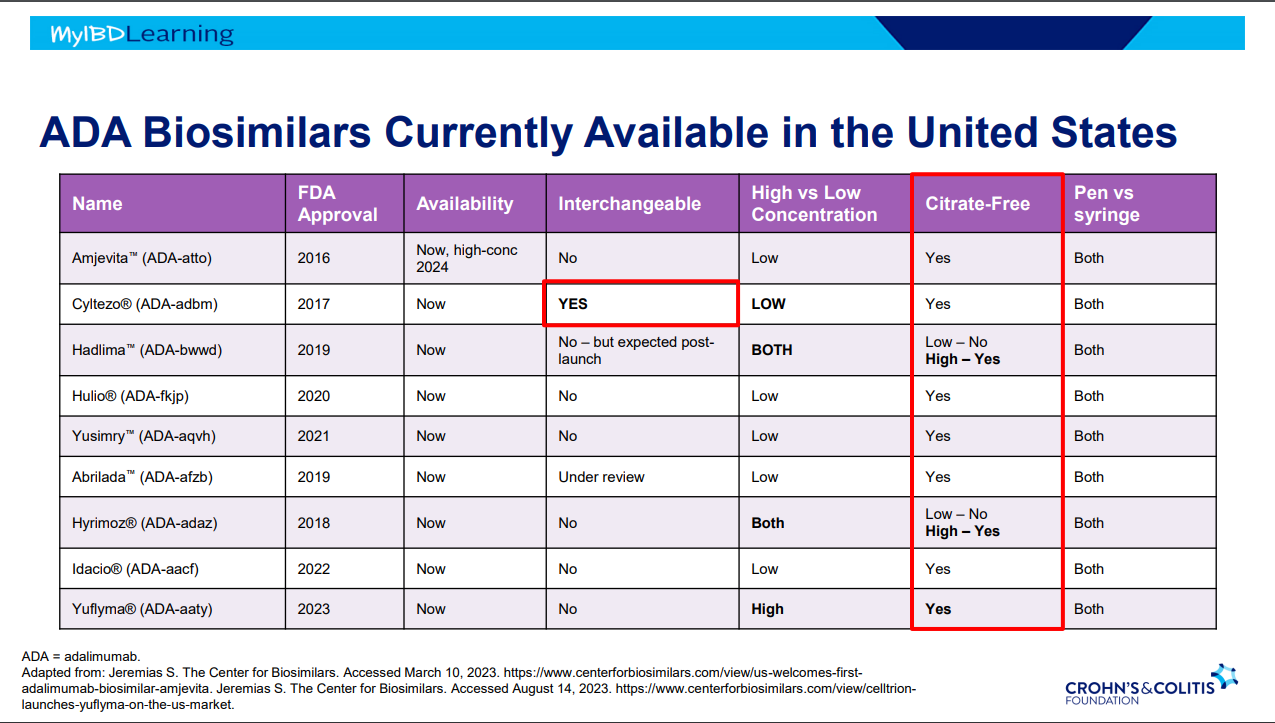
Interchangeable indicates that the drug can be switched by pharmacists
Biosimilars are saving insurers money but no proof that this is saving patients money
Anti-drug antibodies will cross-react to biosimilars
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
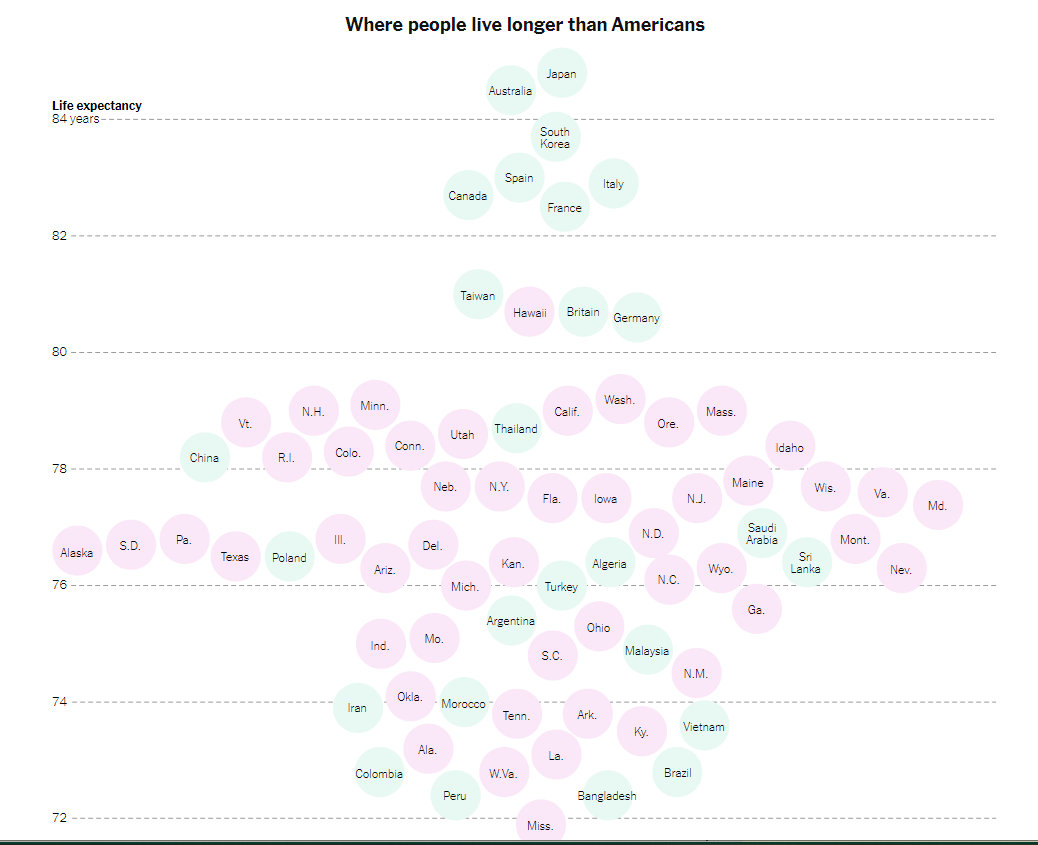
“It’s not just that life expectancy in Mississippi (71.9) now appears to be a hair shorter than in Bangladesh (72.4). Nor that an infant is some 70 percent more likely to die in the United States than in other wealthy countries….
All that is tragic and infuriating, but to me the most heart-rending symbol of America’s failure in health care is the avoidable amputations that result from poorly managed diabetes…A toe, foot or leg is cut off by a doctor about 150,000 times a year in America, making the United States a world leader of these amputations.
America’s dismal health care outcomes are a disgrace. They shame us. Partly because of diabetes and other preventable conditions, Americans suffer unnecessarily and often die young. It is unconscionable that newborns in India, Rwanda and Venezuela have a longer life expectancy than Native American newborns (65) in the United States. And Native American males have a life expectancy of just 61.5 years — shorter than the overall life expectancy in Haiti.“
The article recommends
Expanding Access to Health Care
Work on improving health behaviors: “smoking, eating habits and exercise — affect life expectancy even more than access to health care”…
Work on poverty and education: “America’s health dysfunction is rooted in a broader national dysfunction, including deep intergenerational poverty and despair. The medical system can efficiently amputate a foot, but an improvement in self-care of diabetes sometimes requires an injection of hope and improvements in education, job training, earnings and opportunity.”
This pediatric retrospective study (n=291, 2010-2020) showed a high response to infliximab in patients with inflammatory bowel disease (n=234 Crohn’s disease (CD), n=53 ulcerative colitis (UC)) over a 10-period. Mean duration of treatment among study participants was 2.9 years. Key findings:
53% (n=135) started with doses of 10 mg/kg and 64% (n=87) of those who started on 5 mg/kg were dose-escalated; thus, approximately 76% of patients in their cohort needed doses of 10 mg/kg.
Only 12% of patients discontinued treatment over the observed timeframe.
Patients with UC (P ≤ 0.01) and patients with extensive disease (P = 0.01) had lower durability, despite a higher starting dose of IFX (P = 0.03). Figure 2 indicated that durability in CD was ~93% compared to ~60% for UC with HR of 5.12. The HR for extensive disease (n=77) was 3.74 compared to those with limited disease (n=108). Still, ~75% of those with extensive disease continued on treatment
Common adverse events included 18 with skin findings (14 with psoriasis, 3 nonspecific rash, 1 with lupus), 23 with infusion reactions, 7 with AST/ALT >3 times ULN (or >120 IU/L), and 3 with serious infections.
Like the theme song from the 1996 Olympics (Reach, Gloria Estefan) reaching higher (dosing) resulted in being stronger (i.e.. better outcomes).
My take: This study showed really good outcomes associated with “accelerated” infliximab dosing.
The view before starting a climb at NRocks (Circleville, WV)Highest point of our climb
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.