Key finding: In this cluster randomized controlled trial (n=181, ages 6-10 years), screen media reduction in the treatment group resulted in an increase of 45.8 minutes per day of physical activity compare to the usual routine group.
This is a very helpful review. Table 1 lists treatment indications by group. For example, AASLD recommendations:
Table 3 compares the effectiveness of current treatments
Table 4 describes the large number (~50) of antiviral agents in development and their mechanism of action
The authors recommend HCC surveillance in those with cirrhosis every 6 months with ultrasound with or without serum AFP
“Although current therapy is associated with improved clinical outcome, it is not curative because of a lack of effect on cccDNA and integrated HBV DNA. Stopping therapy in the absence of HBsAg loss usually leads to relapse to active disease in most patients and thus treatment must be administered long term.”
“Many challenges remain, the sheer breadth of therapeutic approaches in development holds great promise for curing and eliminating chronic HBV infection”
My take: While it is likely that newer medications will help many with chronic hepatitis B, the best hope for eliminating HBV continues to be with prevention and vaccination.
Key finding: In this study with more than 30 years of prospective followup (n=214): n a multivariate analysis, both an HBsAg titer >4.44 log10 IU/mL at 15 years of age and HBV genotype C were predictors of advanced fibrosis (odds ratios, 15.43 and 4.77; P = .01 and P = .02, respectively).
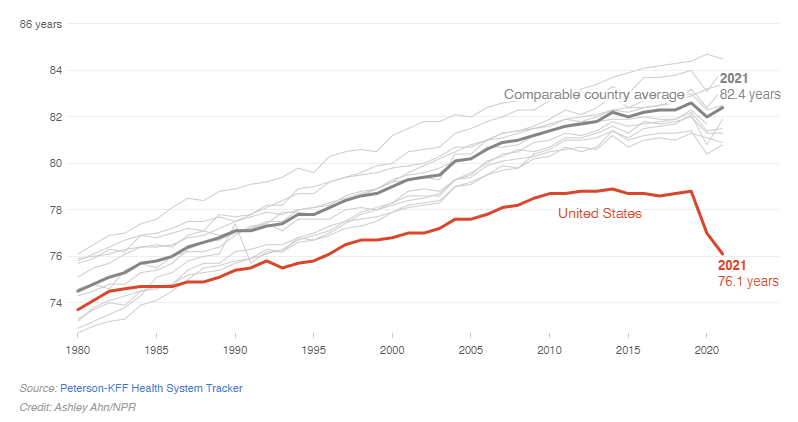
Life expectancy around the world decreased in 2020 due to COVID-19. Most peer countries rebounded by 2021, while the U.S. continued to decline.
An excerpt:
Just before Christmas, federal health officials confirmed life expectancy in America had dropped for a nearly unprecedented second year in a row – down to 76 years. While countries all over the world saw life expectancy rebound during the second year of the pandemic after the arrival of vaccines, the U.S. did not….American life expectancy is lower than that of Cuba, Lebanon, and Czechia.
Then, last week, more bad news: Maternal mortality in the U.S. reached a high in 2021. Also, a paper in the Journal of the American Medical Association found rising mortality rates among U.S. children and adolescents…
The panel looked at American life and death in terms of the public health and medical care system, individual behaviors like diet and tobacco use, social factors like poverty and inequality, the physical environment, and public policies and values. “In every one of those five buckets, we found problems that distinguish the United States from other countries.”
Yes, Americans eat more calories and lack universal access to health care. But there’s also higher child poverty, racial segregation, social isolation, and more. Even the way cities are designed makes access to good food more difficult.
“Two years difference in life expectancy probably comes from the fact that firearms are so available in the United States,” Crimmins says. “There’s the opioid epidemic, which is clearly ours – that was our drug companies and other countries didn’t have that because those drugs were more controlled. Some of the difference comes from the fact that we are more likely to drive more miles. We have more cars,” and ultimately, more fatal crashes.
My take (from authors): “the focus should… be on the fact that every other rich country has been able to figure out how to help people live longer, healthier lives. That means that Americans could do it too.” Meanwhile, lawmakers across the country are protecting kids from harm by stopping drag shows, banning books, and preventing care for transgender kids.
Methods: Electronic records of 100 children seen in the emergency room for gastrointestinal symptoms who had an abdominal radiograph performed were included. Four physicians from each specialty including gastroenterology, radiology, and emergency medicine interpreted the radiographs independently.
Key findings:
Overall agreement among all providers: 40.8%. Fixed margin kappa 0.18
Intradepartmental agreement: 41.5% for Peds GI, 36.7% for Peds EM, and 47.3% for Peds Radiology.
My takes:
The only surprising finding was the low intradepartmental agreement for Peds EM; many of my colleagues have insisted that all Peds EM think everyone has a high fecal burden (so there should have been uniform agreement)
This study reinforces expert guidance to avoid reliance on AXRs for the diagnosis of constipation
This retrospective cohort study (n = 1 365 447) using de-identified claims data from a national private payer (Optum Clinformatics Data Mart), between 2001 and 2018 found that receipt of at least 1 dose of MMR had lower risk for IBD than children who did not (hazard ratio, 0.71; 95% confidence interval, 0.59-0.85). This association persisted after adjustment for potential confounding factors.
My take: This study provides reassurance to encourage MMR vaccination
In this retrospective study (n=533), compare the efficacy and safety of ADA biosimilars SB5, ABP501, GP2017, and MSB11022 in treating IBD outpatients in a real-life Italian setting. Key findings:
Clinical remission was obtained in 79.6% of patients new to biologics and 59.2% of patients new to ADA but not to other biologics
Clinical remission was maintained in 81.0% of patients switched from the originator
No difference in efficacy and safety was found between ADA biosimilars.
My take: This study suggests that these biosimilars are equally effective; however, the fact that nearly 20% failed to maintain remission after switching from the originator ADA indicates more comparative (prospective) studies are needed
Key finding: In this questionnaire-based study among 1093 patients with inflammatory bowel disease (IBD), periodontitis and tooth loss were significantly associated with increased IBD-related disability and more disease activity in the preceding 12 month. This type of study does not allow one to draw conclusions about causality but does provide a good rationale to encourage regular attention to oral health/dentistry.
Methods: In this retrospective study (n=197) reviewed all CD patients between 1990 and 2014 who had undergone diversionary surgery with retention of the excluded rectum for at least 6 months and who had at least 2 years of postoperative follow-up.
Key findings:
92 (47%) of 197 patients ultimately underwent subsequent proctectomy; only 20 (10%) remained symptom-free with excluded rectums.
Only 28 (14.2%) of 197, and only 4 (5.9%) of 66 with initial perianal disease, were able to achieve reanastomosis without further problems
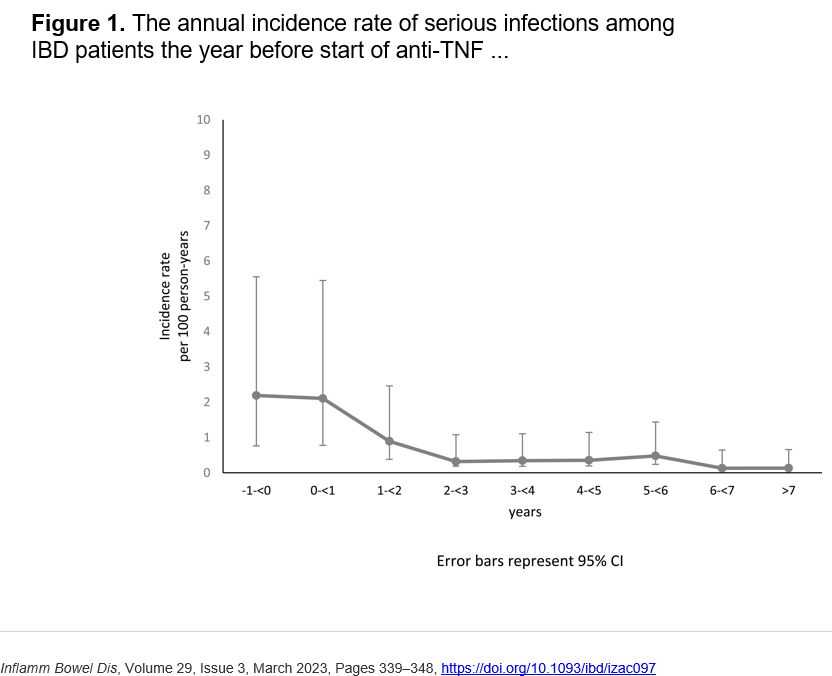
Methods: Retrospective study with 980 patients at 5 centers participating in the Swedish IBD Quality Register. Serious infections, defined as infections requiring in-patient care, the year before and after the start of anti-TNF treatment were evaluated.
A decline in the incidence rate can first be seen beyond 1 year of treatment with anti-TNF, with an incidence rate of 1.22 (95% CI, 0.90-1.66) events per 100 person year compared with 2.19 (95% CI, 1.43-3.36) events per 100 person year the year before treatment. This is a significant reduction of infections, with an incidence rate ratio of 0.56 (95% CI, 0.33-0.95; P = .030).
Key findings:
A 72.0% reduction in the incidence rate of perianal abscesses and intra-abdominal abscesses during treatment with anti-TNF was found compared with before treatment.
Figures 2 & 3 show than most infection rates decreased with treatment. CMV infection did not change significantly with 0.10 per 100 person-years prior to treatment and 0.14 per 100 person-years after starting anti-TNF therapy
” In the current study, patients younger than 20 years old experienced a substantial decrease of infection incidence rate ratio (0.11) with the introduction of anti-TNF treatment. The results could be explained by the fact that young patients have a more active disease with increased risk of infection before treatment with anti-TNF.”
“The most common type of infection after anti-TNF treatment was pneumonia. The high incidence of pneumonia confirms earlier data.9,36,37” However, the authors show that the rate of pneumonia dropped from 0.51 to 0.27 per 100 person-years after starting anti-TNF therapy.
The authors note that a prior study by “Zabana et al showed that patients with IBD had an increased risk for serious infection after starting immunosuppressive treatment compared with before treatment (median follow-up 3 years before and 5 years after)… the discrepancy in the result may be explained by selection bias. We included all patients starting anti-TNF treatment. However, Zabana et al included only patients who suffered from infections during immunosuppressive treatment and retrospectively examined the risk of infection before start of treatment.24“
Limitations of study: several other important factors affecting infections were not captured in this study including steroid exposure and nutritional status.
My take (from authors): “The incidence rate of serious infection among IBD patients did not increase with anti-TNF therapy. Instead, serious infections seemed to decrease more than 1 year after initiation of anti-TNF treatment.”
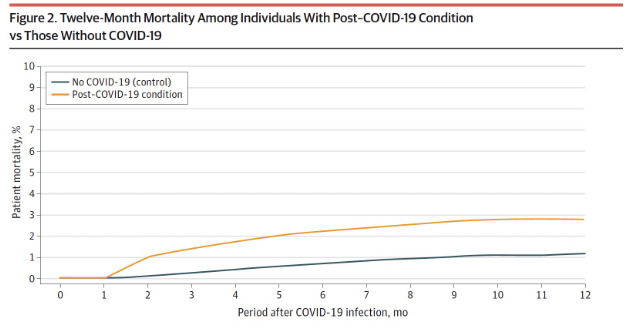
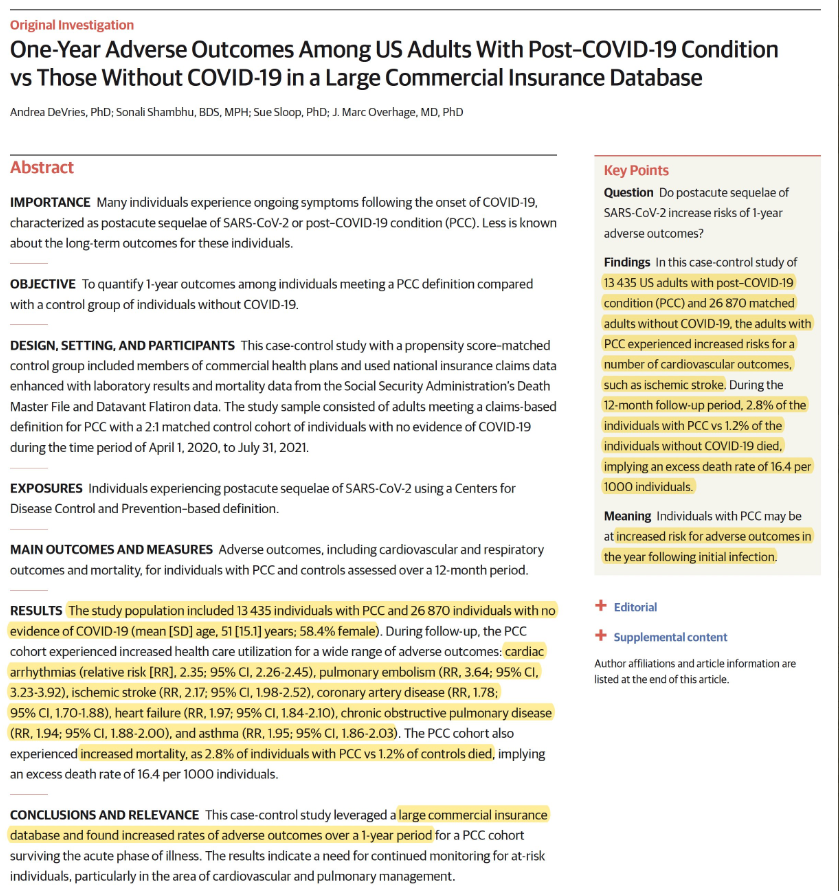
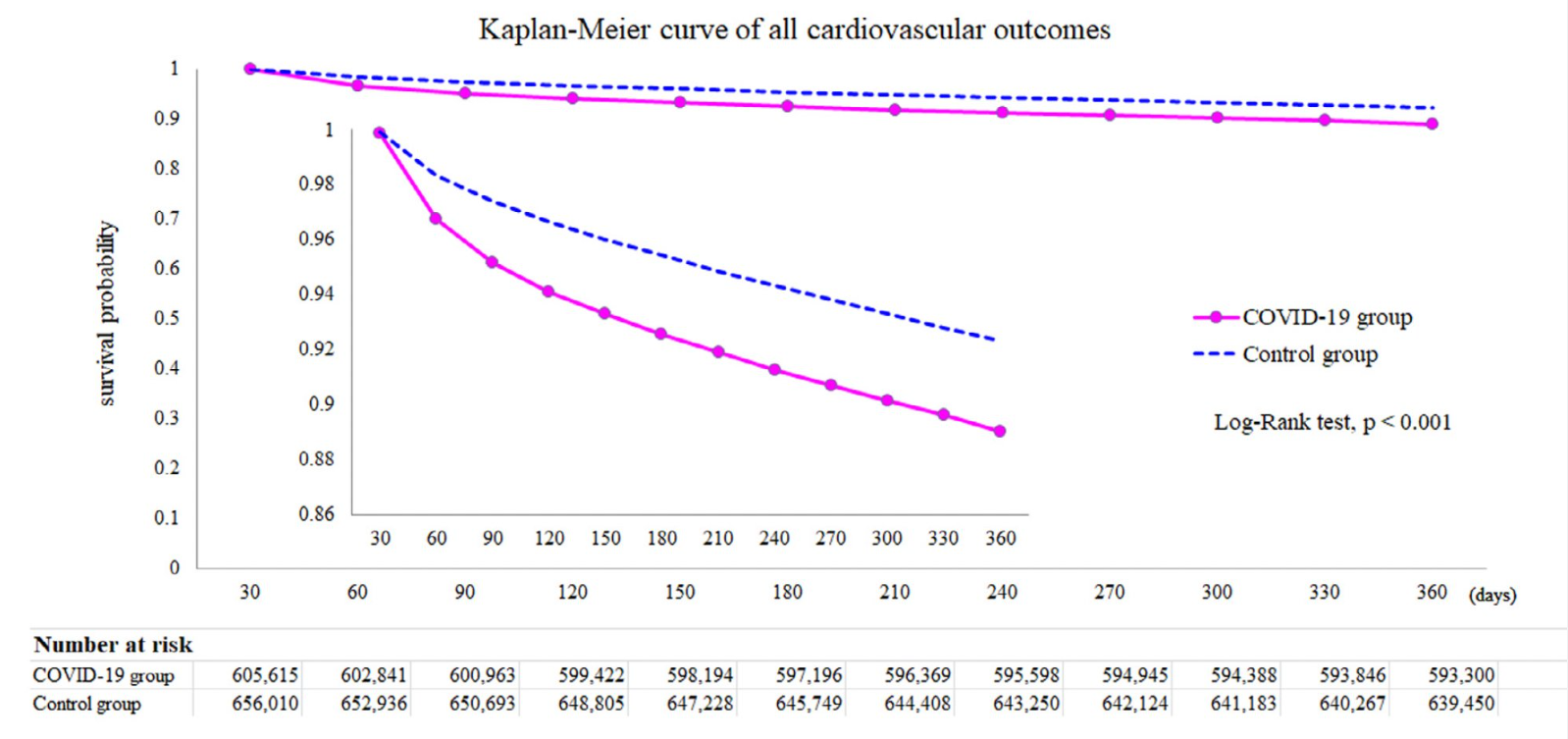
This case-control study leveraged a large commercial insurance database and found increased rates of adverse outcomes over a 1-year period for a post-COVID-19 cohort surviving the acute phase of illness. Methods: An index month was set by adding 30 days to the COVID-19 diagnosis date (this study looked at outcomes starting one month after diagnosis).
This study used the data from the US Collaborative Network in TriNetX. From a cohort of more than 42 million records between 1 January 2019 and 31 March 2022, a total of 4,131,717 participants who underwent SARS-CoV-2 testing were recruited.
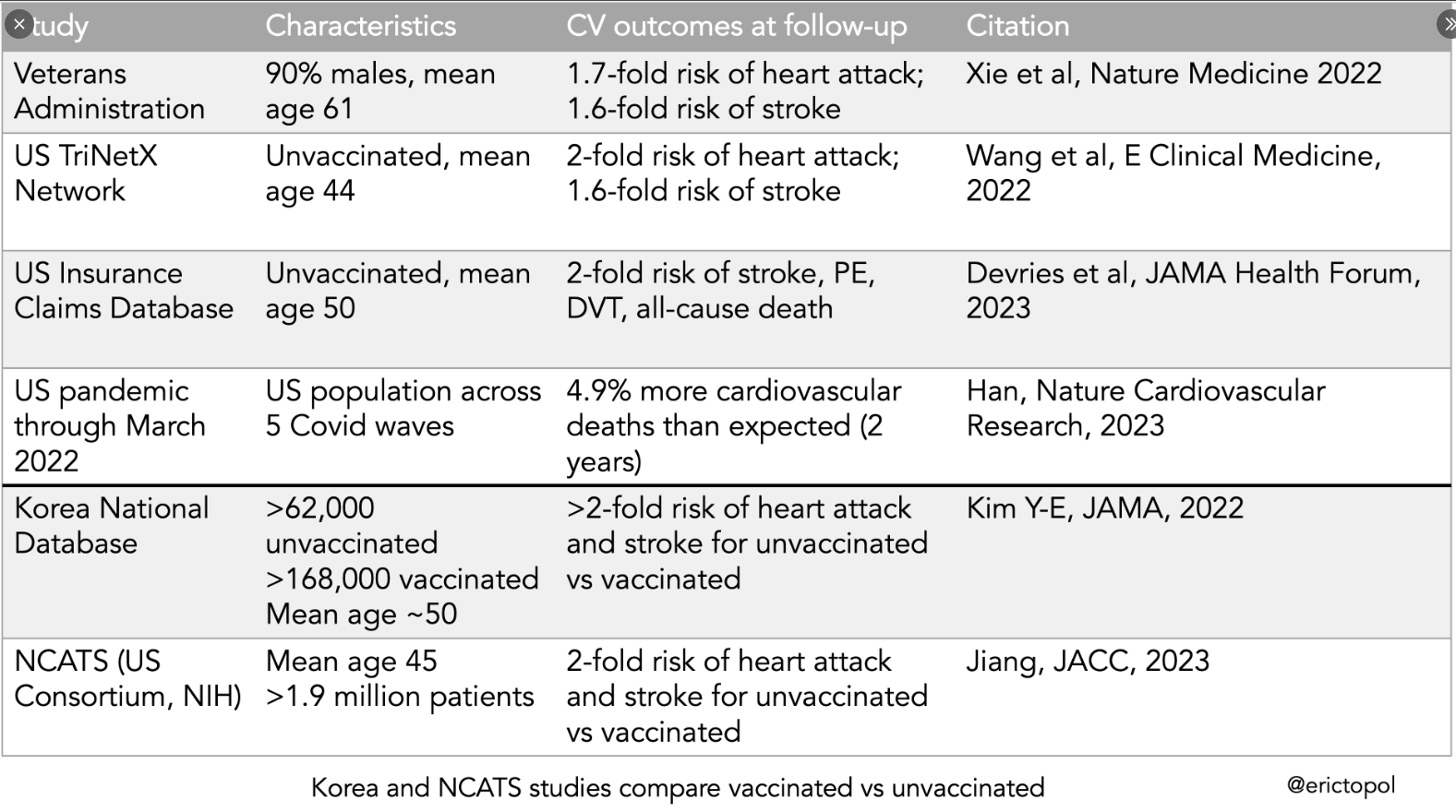
My take: Many detractors of vaccination have focused on potential cardiac adverse events. These studies indicate that COVID vaccination provides protection against major cardiovascular outcomes
This study, in agreement with prior studies of individuals with chronic liver disease, showed that statin use is associated with a lower risk of hepatocellular carcinoma in NAFLD as well, with a Hazard Ratio of 0.47 in a database with 272,431 adults with NAFLD. The authors note the concern about hepatotoxicity from statins; however, “severe liver injury from statins is fairly low. Indeed, the incidence of lovastatin-associated fulminant liver failure is about 2 in a million users.”
Porto‐sinusoidal vascular disorder (PSVD; also previously described as idiopathic noncirrhotic portal hypertension [NCPH]…”is a group of liver vascular diseases featuring lesions encompassing the portal venules and sinusoids unaccompanied by cirrhosis, irrespective of the presence/absence of portal hypertension. It can occur secondary to coagulation disorders or insult by toxic agents. However, the cause of PSVD remains unknown in most cases.”
Key findings:
In a group of 4 patients, a novel heterozygous mutation in the FCHSD1 gene was identified but not in 2 familial controls.
When this variant was introduced in mice using CRISPR, ” Nine out of the 15 mice carrying the human FCHSD1R183Wvariant mimicked the phenotype of human PSVD, including splenomegaly and enlarged portal vein.”
Aberrant FCHSD1 structure and function led to mTOR pathway overactivation
“Consumptive hypothyroidism (CH) is a rare form of hypothyroidism due to thyroid hormone inactivating enzyme type 3 (Deiodinase) overexpressed by hepatic/hepatic and cutaneous hemangiomas, and occasionally by some other extrahepatic visceral hemangiomas…Pediatric hepatologists should recognize the importance of periodical assessments of thyroid function in patients with hepatic hemangiomas”
“MRI of the abdomen in one of our patients (patient 1), before (A) and after (B) 19 months of treatment with propranolol/10 months of treatment with levothyroxine. The T2-weighted axial MRI images shows the regression of a diffuse infantile hepatichemangioma with innumerable T2 hyperintense masses throughout the liver with central hypointense central regions.”
In this multicenter randomized open-label, single-blind trial of patients (n=4270) 40 years or older (mean age 62 years) with polyps of 4 to 10 mm, cold snare polypectomy (CSP) was compared with hot snare polypectomy (HSP).
Key findings:
Eight patients (0.4%) in the CSP group and 31 (1.5%) in the HSP group had delayed bleeding (w/in 14 days) (risk difference, −1.1% [95% CI, −1.7% to −0.5%]).
Severe delayed bleeding (drop in Hgb of 2 g/dL) was also lower in the CSP group (1 [0.05%] vs. 8 [0.4%] events; risk difference, −0.3% [CI, −0.6% to −0.05%])
The CSP group had fewer emergency service visits than the HSP group (4 [0.2%] vs. 13 [0.6%] visits
Polyp type (in Table 2): 70% were adenomas, 5% were sessile polyps, and 23% were nonneoplastic which includes hyperplastic polyps, inflammatory polyps, and nonsignificant lesions. ~56% had a “polypoid morphology” and ~ 44% had a “nonpolypoid morphology.”
“Besides an improved safety profile, another advantage of CSP is its high efficiency. This study’s results showed that the time required for polypectomy is reduced by 26.9% with CSP (difference in mean, -44.0 seconds)”
Why is CSP safer?
“The shallower resection depth in CSP is one of the factors contributing to the lower bleeding risk. Besides the tearing force, electrocautery also applies more energy to the soft tissue… (28). Profound submucosal destruction may occur in 60% of cases, and the muscularis propria may be damaged in 20% of patients receiving HSP; however, all cold resections are limited to the shallow submucosa. Because larger vessels are usually located in the deeper submucosa, the shallow resection depth of CSP causes less arterial injury, thereby reducing the risk for delayed bleeding (29).”
My take: It would be helpful to replicate these findings in children mainly due to differences in polyp types that are found. Nevertheless, this study suggests that it is likely more risky to use cautery for small polyps (“including persons using antiplatelet agents or anticoagulants”).
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
I recently attended an online lecture which reviewed Alagille Syndrome and the emergence of an IBAT inhibitor for the management of cholestatic pruritus. Selected slides from Mirum Pharmaceutical Lecture: “Updates in the Treatment of Cholestatic Pruritus in Patients With Alagille Syndrome.” *I have no financial disclosures or conflict of interests in this medication or company.
The severe itching which is seen in most patients with Alagille is often quite detrimental to quality of life. It impacts sleep, causes irritability, skin damage, and physical distcomfort
Typically, the first week of receiving the medication, it is started at1/2 the maintenance dose.
Monitoring response can be done with the ItchCheck App, Itch score or Clinical scratch score
Monitoring hepatic blood tests and periodic monitoring of fat soluble vitamins is recommended
My take: Though Alagille syndrome is a multisystem disease, improvement in pruritus due to cholestasis with an oral daily medication is an important advance/option. There is little systemic absorption and thus far a reassuring safety profile.