Methods: In this prospective non-blinded trial, 22 responders to 6-food elimination diets underwent sequential food reintroduction guided by esophageal sponge cytology
Key findings:
At the post food reintroduction evaluation, sponge cytology and biopsy histology were in agreement in 59% (13/22) of cases using a cutoff of <15 eos/hpf and 68% (15/22) of cases using a cutoff of <6 eos/hpf. With the cutoff of <15 eos/hpf, the median absolute difference was 38 eos/hpf.
Interestingly, the authors noted a high rate (23%) of dietary responders who had dietary reintroduction without a dietary trigger being identified; this is possibly related in part to lower sponge sensitivity, and possibly due to a short food reintroduction period of 2 weeks prior to testing.
The authors in their discussion note that it is unclear whether the values from the sponge or from the biopsy is more reliable.
My take: This is a disappointment for those of us waiting for a reliable non-invasive measure of EoE activity. Those with abnormal sponge results are fairly likely to have abnormal endoscopy; however, many of those with normal values with sponge testing are likely to have active EoE.
Using a retrospective cohort design with 22,257 patients (51% female) with a mean age of 61 years, Key Findings:
There was a 2% per year rate of developing symptomatic gallstones
Overall, 14.5% developed symptoms with a median followup of 4.6 years
Cumulative incidence of becoming symptomatic: 10.1% at 5 years, 21.5% at 10 years, and 32.6% at 15 years
The strongest predictors of developing SGs were female gender (hazard ratio [HR], 1.50), younger age (HR per 5 years, 1.15), multiple stones (HR, 2.42), gallbladder polyps (HR, 2.55), large stones (>9 mm) (HR, 2.03), and chronic hemolytic anemia (HR, 1.90). Elevated BMI was associated with increase risk; for example a BMI >40 had a HR of 1.60.
Statin use was associated with a reduced risk of with HR 0.61
My take: This large retrospective study of adults indicates that if given enough time, more than 1/3rd of individuals will develop symptomatic gallstones. Surgical intervention should be considered in those with significant risk factors.
This article explains how generic and biosimilar companies have tried to navigate the ‘patent gamesmanship’ that brand-name manufacturers have used to delay competition for their products beyond the typical 20 years after an application is filed.
Key points from this article:
“The Hatch–Waxman Act, provided a partial solution by explicitly authorizing manufacturers to market generic drugs if they don’t claim any indications protected by active method-of-use patents.3 Such skinny labeling enables generics manufacturers to market their products for older, non–patent-protected indications without infringing later-issued method-of-use patents…43% of products that were the first available generic formulation of a brand-name drug included skinny labels”
The article delves into the GlaxoSmithKline v. Teva case which centers on the overlapping potential indications for the beta-blocker carvedilol. Teva had used skinny labeling to get approval for hypertension (HTN) but was sued by GlaxoSmithKline as carvedilol can be used for congestive heart failure (CHF).
Much of the case centers on the paradox that “by law, generics [& biosimilars] manufacturers are required to use very similar labels” as the labeling of original products even though the generic has requested approval for a much narrower approval. In this case, when the Teva generic was used for CHF, GlaxoSmithKline sued since the product was approved for HTN.
Another example: Humira has “more than 70 patents on inventions ranging from the active pharmaceutical ingredient and primary indications to the drug’s purity, various formulations, and secondary indications.” For a generic/biosimilar to address all of these (potentially-endless) patents is a huge barrier.
Based on this ruling, “brand-name manufacturers can thus now create labels that reference material related to new method-of-use patents and then sue generics manufacturers for patent infringement.”
“Lack of action by both the Supreme Court and Congress would allow brand-name drug manufacturers to wield a powerful new weapon to delay or deter the entry of generic and biosimilar drugs, which could have important implications for health care costs and patient welfare.”
My take: My prediction is that these tactics by drug manufacturers, despite their extensive financial connections with lawmakers, will eventually backfire and result in extensive changes to the regulations regarding exclusivity and pricing.
In an unrelated article in the same issue, Golda Grinberg provides a first-hand account of how families could benefit by the consideration of hospice in children with extensive medical problems. NEJM 2023; 388: 486-487. Please Look at My Baby — When Clinicians Should Say the Word “Hospice”
“To the surprise, perhaps even shock, of the SICU team, we tossed an option B onto the table: if we truly could not extubate, we suggested, maybe we should skip the trach and transition to comfort care….When presented with a child in whom previous extubation attempts had failed and who was becoming more deconditioned by the day, the SICU team had made the standard, safe, and familiar recommendation for an acute problem: place a trach… It would have been tremendously helpful if, from the beginning, we’d had an open conversation with our son’s medical team and discussed all the options.”
My take: Most parents are happy with their medical decisions for their children. However, it is not uncommon to hear parents say many years later that they wished that they had been informed of the long-term dire outlook of their children and the possibility of deescalation of care in children with severe medical conditions before embarking down the ‘standard’ path.
This is a lengthy article with a great deal of useful information. Here are some of the important recommendations most relevant for pediatric gastroenterologists/hepatologists:
In patients with PSC without known inflammatory bowel disease (IBD), diagnostic colonoscopy with histological sampling should be performed and may be repeated every 5 years if IBD is not initially detected
In patients with PSC in whom IBD is diagnosed, high‐definition surveillance colonoscopy with biopsies should start at age 15 years and be repeated at 1‐year to 2‐year intervals to evaluate for colonic dysplasia
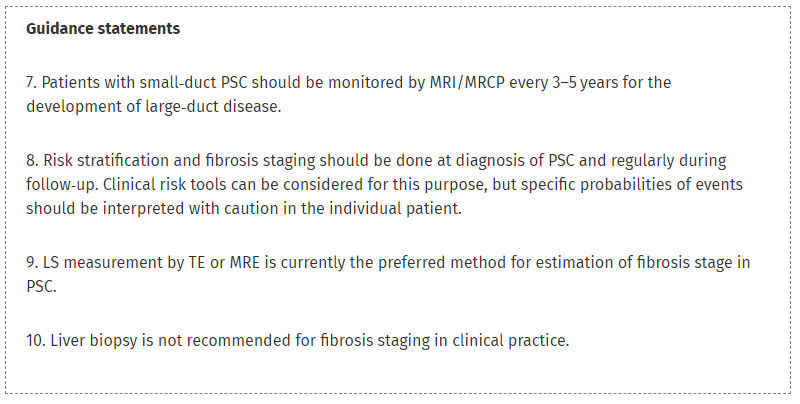
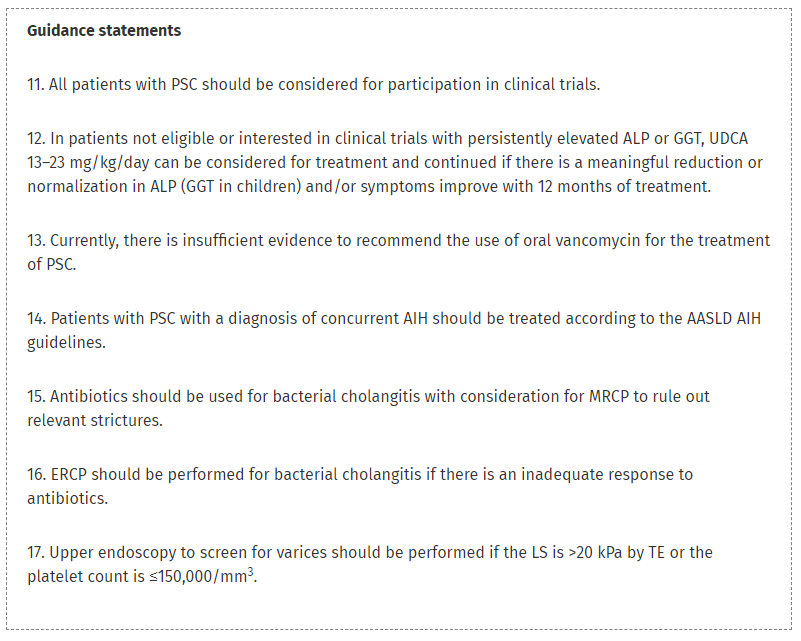
New clinical risk tools for PSC are available for risk stratification, but probabilities of events in individual patients should be interpreted with caution
All patients with PSC should be considered for participation in clinical trials; however, ursodeoxycholic acid (13–23 mg/kg/day) can be considered and continued if well tolerated with a meaningful improvement in alkaline phosphatase (γ‐glutamyl transferase in children) and/or symptoms with 12 months of treatment
Upper endoscopy to screen for varices should be performed if the LS is >20 kPa by TE or the platelet count is ≤150,000/mm3
Bone density examinations should be performed to exclude osteopenia or osteoporosis at diagnosis and at 2‐year to 3‐year intervals thereafter based on risk factors
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
Esmati et al.1 present a fascinating analysis of the impact on waitlist outcomes of a 2014 Eurotransplant (ET) policy that prioritizes patients younger than the age of 2 years with biliary atresia for deceased donor liver transplantation (DDLT) offers
Waitlist mortality decreased from 6.7% before to 2.3% after implementation of the new policy. Unexpectedly, this was not associated with an increase in DDLTs
During the same time period, the proportion of young patients with BA who underwent living donor liver transplantation (LDLT) increased from 55% to 74%.
Without adaptions to the pediatric Model for End‐Stage Liver Disease (MELD) or Pediatric End‐Stage Liver Disease scores, children can never fairly “compete” for deceased donor livers because of the tremendous volume and demand from the adult candidate list
My take (borrowed from editorial): There are many potential ways to achieve the desired goal of zero pediatric waitlist mortality. And, multiple strategies can successfully be pursued in parallel: prioritize children, increase use of LDLT, and increase/mandate use of split livers.
Another (unrelated) study in this issue -easy way to assess mobility (a key element of frailty) in adults with decompensated liver disease: AJ Groff et al. Liver Transplantation29: 226-228. Open Access! A novel method using the level of mobility to predict mortality in patients admitted for decompensated cirrhosis: A prospective study The authors found the following: a value of <8 on The Johns Hopkins Highest Level of Mobility score (JH‐HLM, see below) was associated with much higher risk of mortality compared with those with a JH‐HLM score of 8.
In this study with 580 children, consecutively recruited from 2016 to 2020, the authors examined outcomes after ingestion of sharp-pointed foreign bodies (FBs).
Key findings:
Mean age was 50 months.
Sharp/pointed FBs mainly included fragments of metal 270 of 580 (46.55%) and glass 180 of 580 (31%).
FBs were endoscopically removed in 79 of 580 (13.6%) children whereas the remaining FBs passed through the gastrointestinal tract over an overall mean time of 29 hours
No cases of intestinal perforation nor prolonged retention were observed.
The most common metal objects were earrings (n=72). Other objects: screws (n=20), dental works (n=20), nails (n=13), open safety pins (n=7), fish bones (n=65)
My take: I have not had a severe complication from sharp-pointed FBs (in nearly 30 yrs of pediatric GI practice); this article confirms the overall low risk that they pose.
In this retrospective study with 56 patients with autism spectrum disorder (ASD) and 123 controls underwent colonic manometry (CM). Key findings:
The rate of abnormal CM findings between ASD and matched controls (24% vs 20%, P = 0.78) did not differ significantly
The authors noted that higher rates of abnormal CM with duration of constipation and with soiling in children with ASD. However, “even in the minority of cases with abnormal colonic motility, chronic stool retention due to functional constipation over time likely caused impaired motility in the majority of these cases. In 6 of the 8 ASD cases with abnormal CM finding, impaired motility was isolated to the distal colon while normal motility occurred in the proximal colon.”
My take: In this highly-selected group of patients with ASD from specialized motility centers, only 2 had abnormal colonic motility affecting the entire colon. Overall, patients with ASD did NOT have higher rates of abnormal CM studies. Hence, for most children with ASD, CM has little value.
This was a very large retrospective study (with more than 90 authors) with 1433 children.
Key findings:
Only 40.3% of children reach adulthood with their native liver; 54.4% had their native liver at 10 years of life
“It is noteworthy that bile duct paucity was reported in only 65% of liver biopsies performed during the first 3 months of life, the period during which there are diagnostic challenges with distinguishing ALGS from syndromic BA.” Thus, with a liver biopsy, there is a significant risk of misdiagnosis
The all‐cause mortality rate was 8.5%
The total bilirubin level between 6-12 months of life had significant predictive value. In the associated editorial: “The authors reported that 79% of patients with median TB of <5.0 mg/dL..reached adulthood with their native livers, whereas only 31.6% and 18.2% of patients with median TB levels between” 5-10 and >10 mg/dL survived into adulthood with their native livers.
The editorial makes the point that this data will be helpful and ongoing studies will be needed to determine the effectiveness of novel treatments (e.g. IBAT inhibitors)
My take: This is a very useful study in understanding the long term outcomes of Alagille syndrome.
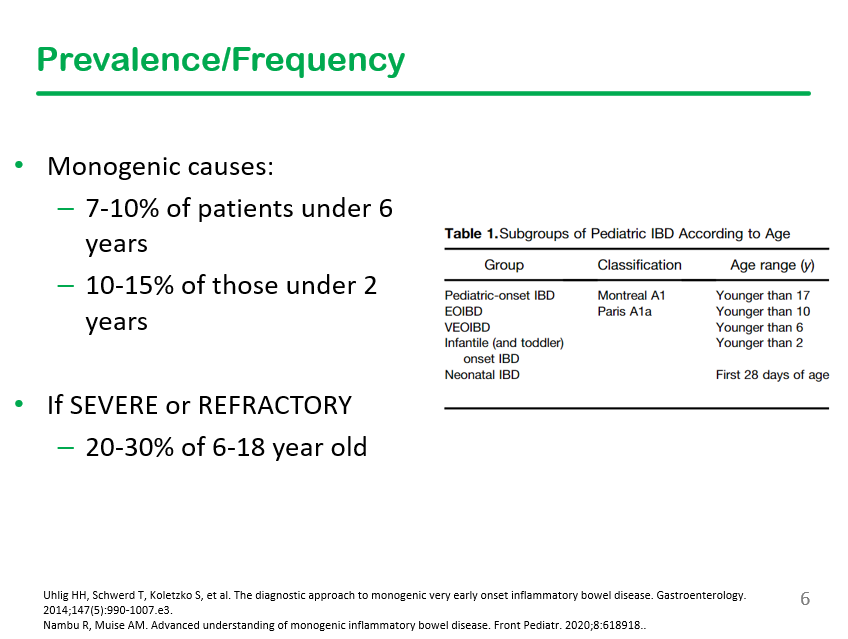
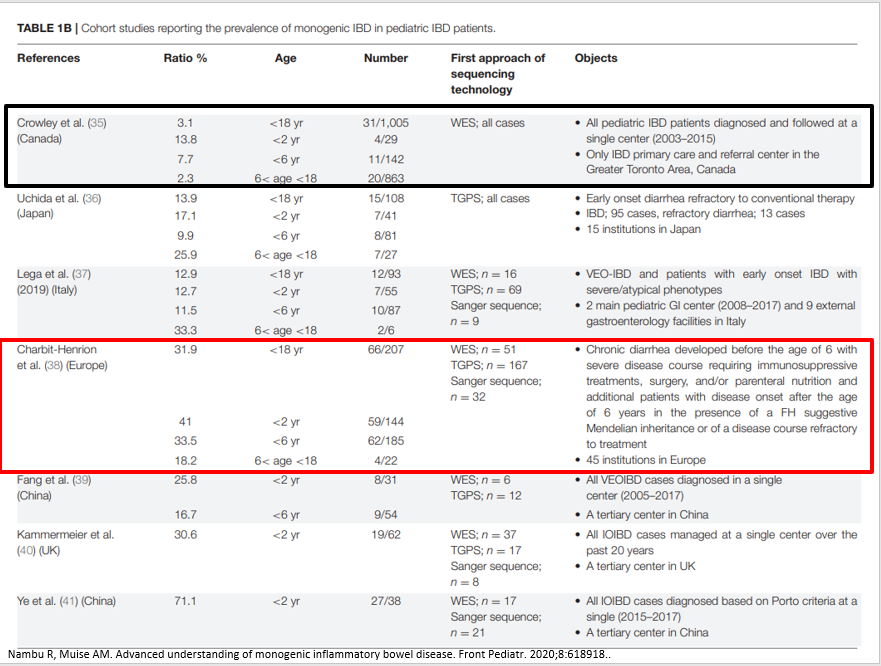
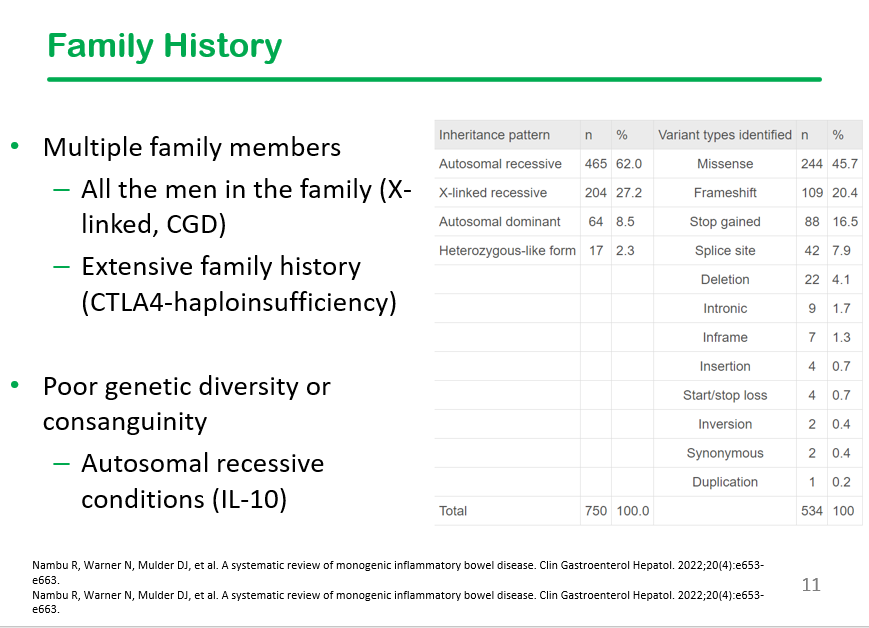
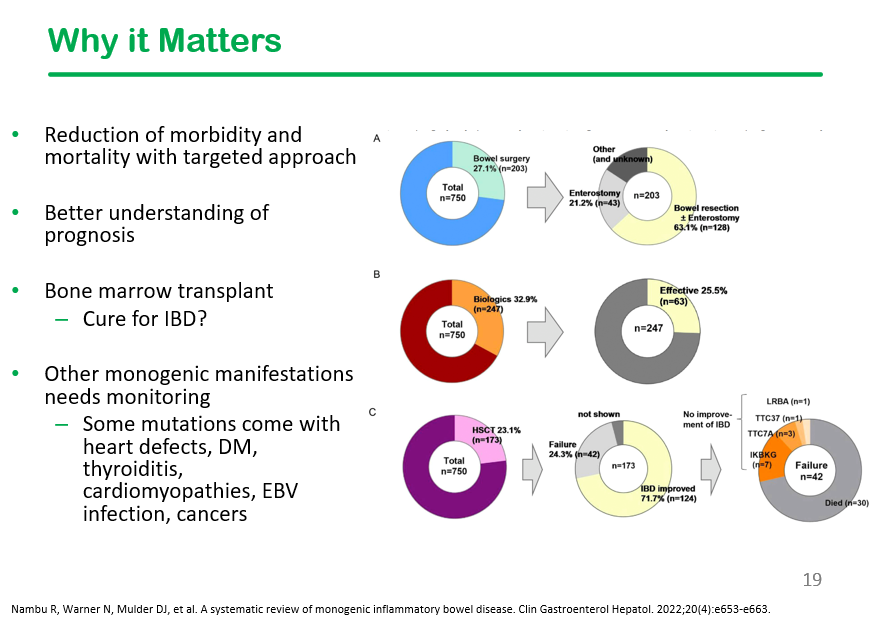
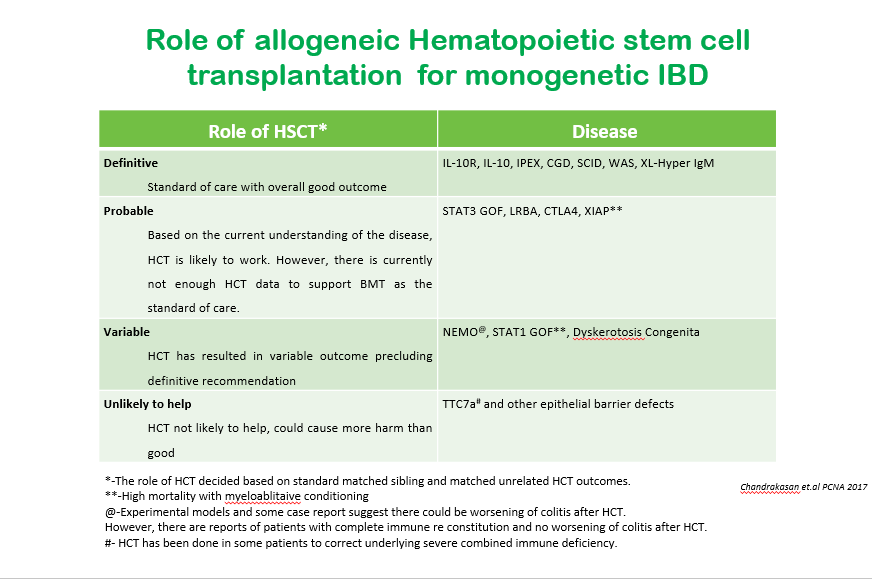
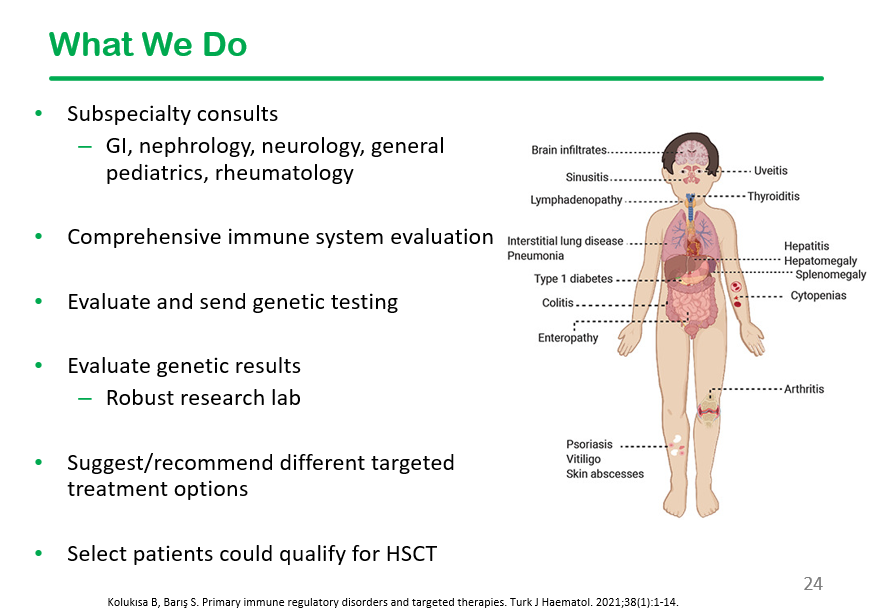
At our center, we are fortunate to work with an immune dysregulation clinic (Dr. Shanmuganathan Chandrakasan, Dr. Taylor Fitch) that helps sort out patients with inflammatory bowel disease with underlying monogenetic disorders. This is very important as specific treatments, including hematopoietic stem cell transplants (HCST), may be needed. The likelihood of an underlying monogenetic disorder is much more frequent in the VEO population. A recent talk on this topic by Taylor Fitch was given to our group. Here are some of the slides:
Generally, about 2% of those older than 6 years of age have monogenetic disorders, but it is much higher in those with severe or refractory disease.
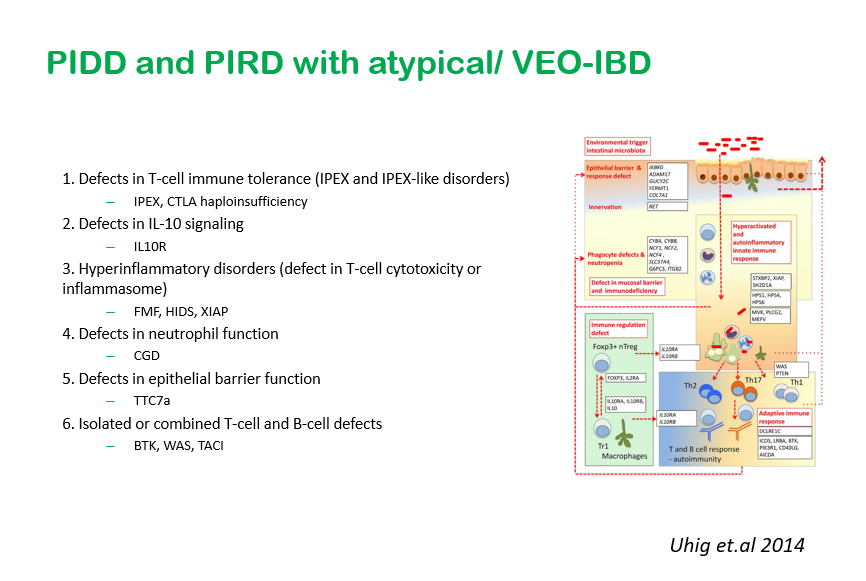
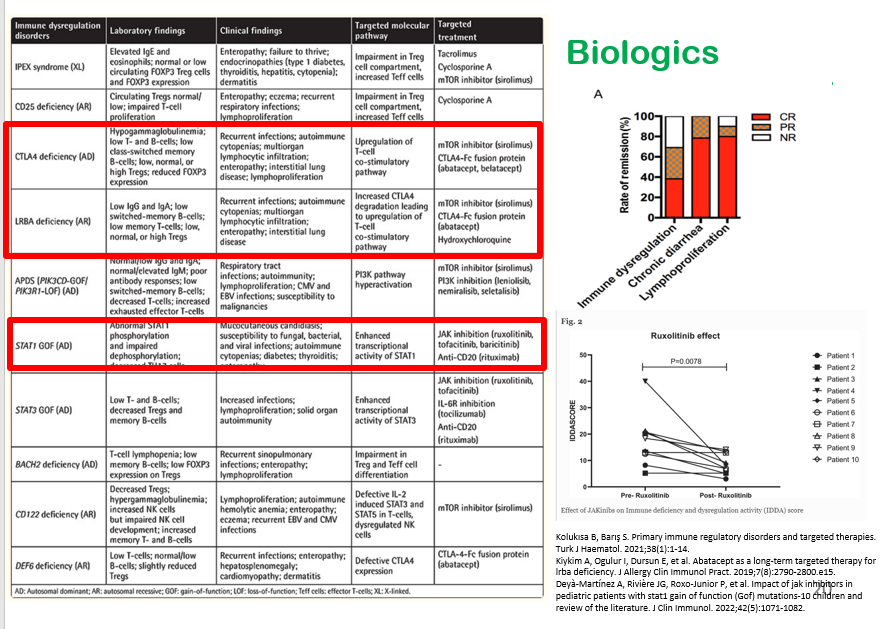
This slide shows six major categories of immune defects.
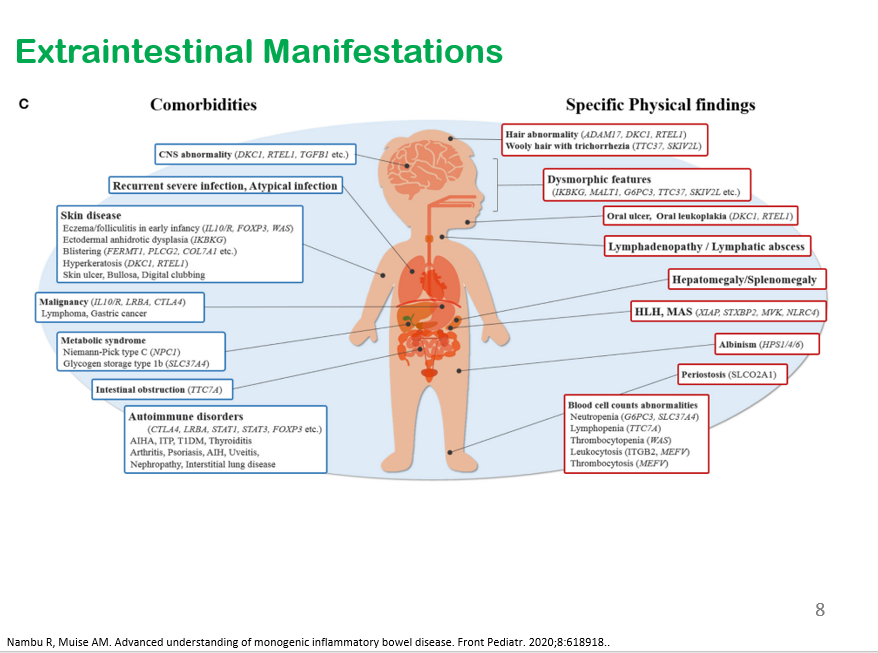
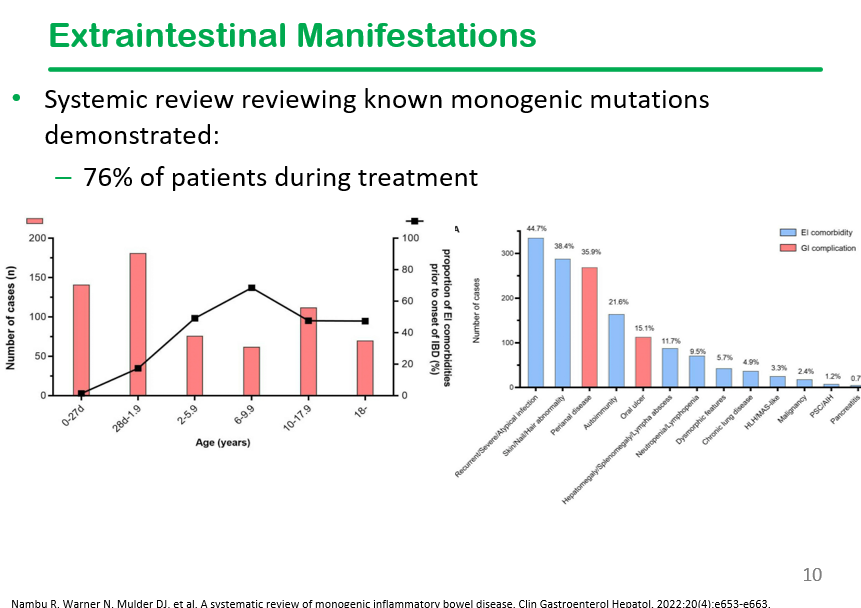
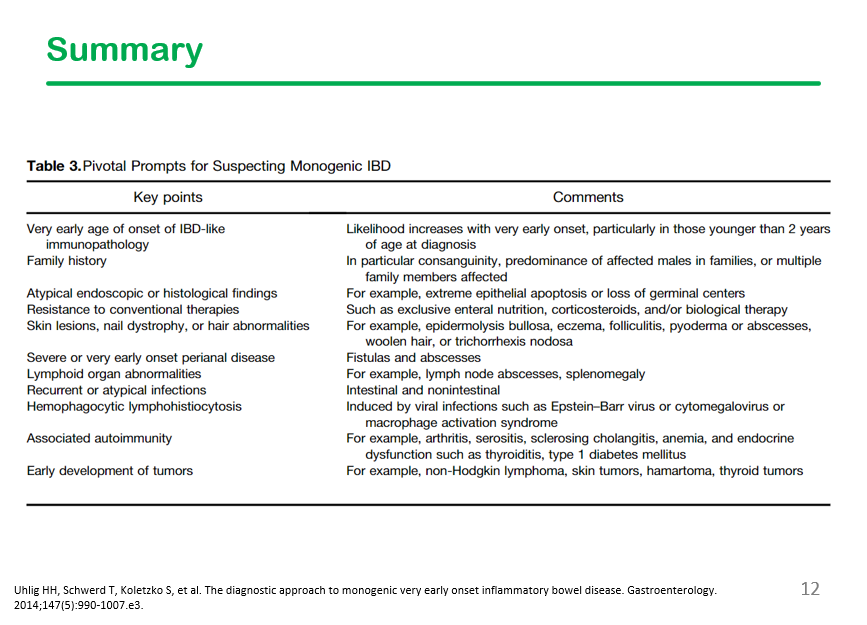
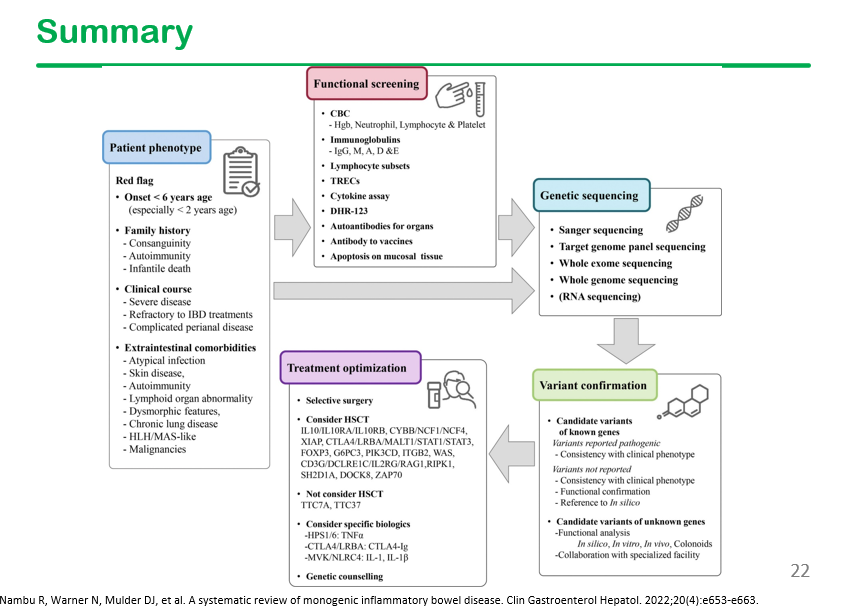
This slide shows the high frequency of extraintestinal manifestations in patients with monogenetic disorders, particularly recurrent infections, skin/hair abnormalities, and autoimmunity. Perianal disease is also frequent in this population.
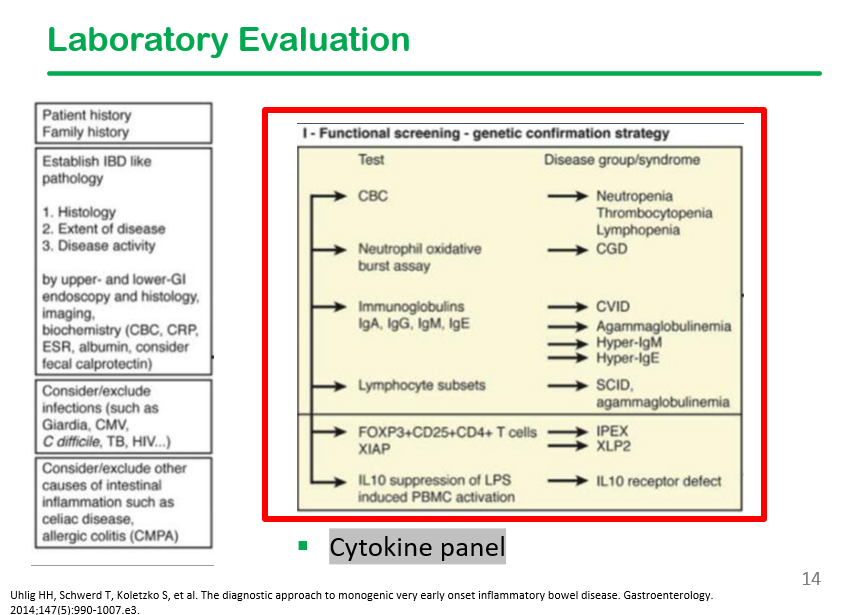
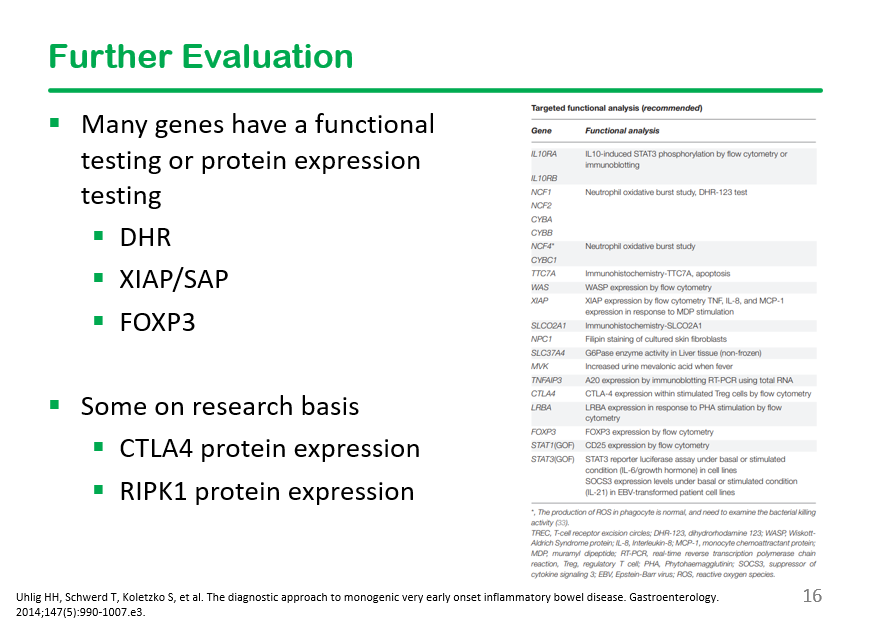
In the discussion, it was noted that DHR testing is often unreliable, especially if the specimen is not run promptly.
My take: I have had several patients with IBD/immune dysregulation, including a patient with CTLA4 and a patient with TTC7A. Making these diagnoses led to specific treatment recommendations. The patient with CTLA4 is doing well with abatacept therapy.
For those in Atlanta, a referral can be made via EPIC order and/or via contact with immune dysregulation team members. Epic order:
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
S Corlette, CH Monahan. NEJM 2022; 387: 2297-2300.
There are a lot of problems with the U.S. Healthcare system. This article focuses on healthcare coverage.
The U.S. has a patchwork system of health insurance coverage “in which people’s access to services and level of financial protection — not to mention whether they have coverage at all — varies depending on their birthplace, age, job, income, location, and health status…Many people in the United States work for employers that do not offer insurance or do not sufficiently subsidize it, making it unaffordable for lower-income workers.”
“No one would purposefully design the system we have. Unlike many of our peer countries, the United States has never had a centrally planned, cohesive system to help its citizens obtain and pay for health care services. Ours is a system built on happenstance, unintended consequences, and gap filling…”
“The United States has made sporadic efforts at creating a national system of health coverage…These efforts all foundered in the face of opposition from health insurers, the American Medical Association, and other health industry stakeholders, as well as concerns about the proposals’ costs.”
“Americans who have “good” insurance today may be surprised to learn that they, too, are vulnerable. Underinsurance is a growing problem, as fewer and fewer Americans are able to afford their share of costs. Premiums and deductibles continue to increase as health care costs rise, straining the budgets of families, employers, and state and federal governments. Unless and until policymakers curtail the power of health care monopolies to drive up costs and do more to limit health care prices across our array of public and private coverage systems, virtually everyone’s access to affordable care is at risk… the primary reason millions of Americans remain uninsured or have insurance coverage that leaves them financially exposed is the high costs in our health care system. Constraining the growth of costs while reducing inequities in access and outcomes will require new but difficult reforms.”
My take: There are no simple solutions to the high costs of our health care or to assuring adequate coverage. At every level, there are excessive costs which undermine these goals:
Hospitals charge exorbitant fees and try to monopolize markets
Insurance companies have split loyalties and often deny expensive but necessary care
Pharmaceutical companies charge as much as the market will bear even with older generics. Increasingly, newer medications are very expensive
Health care providers have no incentives to constrain costs. Even salaried physicians may feel complicit by being part of systems owned by hospitals and venture capital firms which have excessive charges.
Although deaths from Covid have slowed, the disillusionment among health workers has only increased. Recent exposés have further laid bare the structural perversity of our institutions. For instance, according to an investigation in The New York Times, ostensibly nonprofit charity hospitals have illegally saddled poor patients with debt for receiving care to which they were entitled without cost and have exploited tax incentives meant to promote care for poor communities to turn large profits. Hospitals are deliberately understaffing themselves and undercutting patient care while sitting on billions of dollars in cash reserves. Little of this is new, but doctors’ sense of our complicity in putting profits over people has grown more difficult to ignore…
And many physicians are now finding it difficult to quash the suspicion that our institutions, and much of our work inside them, primarily serve a moneymaking machine…Our health care institutions as they exist today are part of the problem rather than the solution.”