A new and promising approach — which Dong, Rao, and their colleagues describe in the journal Nature — focuses on curbing intestinal inflammation rather than fighting the bacteria directly…
In response to the toxin, the sensory neurons secrete the neuropeptides substance P and calcitonin gene-related peptide (CGRP), while the pericytes, which surround blood vessels, produce pro-inflammatory cytokines. In a mouse model, this drove intense neurogenic inflammation and tissue damage —the same kind of damage that occurs in patients…
FDA-approved drugs already exist to block the triggering neuropeptides. Aprepitant, used for nausea and vomiting, blocks substance P signaling. Small molecules related to olcegepant or monoclonal antibodies such as fremanezumab, used for migraines, inhibit CGRP signaling.
In the mouse model, these drugs reduced inflammation and tissue damage. Somewhat surprisingly, they even reduced the burden of C. diff bacteria in the animals’ intestines.
My take: Clinical trials are needed to see if these therapies can improve outcomes more than current treatments.
In this study with 39,734 commercially-insured initiators of IBD medications (18-64 year old), 34% had a colonoscopy by 12 months and 42% at 15 months. The authors state that “it is evident that patients without any colonoscopy during this interval are not being followed under an optimal long-term T2T (treat-to-target) paradigm.”
This retrospective study examined 123 patients with Crohn’s disease and 40 with ulcerative colitis who had dose intensification with ustekinumab (to either every 4 weeks, n=91, or every 6 weeks, n=72). Dose escalation was effective in both achieving and maintaining corticosteroid-free clinical remission for 61% of patients with Crohn’s disease and 40% with ulcerative colitis at 24 months; endoscopic remission was noted in 43% with Crohn’s disease and 55% with ulcerative colitis.
Using data from multiple studies with 1157 patients, only 9 tofacitinib patients developed Clostridioides difficile infection (CDI) which was lower than the placebo group. CDI were all mild–moderate in severity and resolved with treatment in 8 patients. Six of 9 patients continued tofacitinib treatment without interruption. The low rate of infection was likely in part due to screening for CDI prior to treatment. In addition, “it is possible than the lower rates of CDI …may be due to better-controlled disease…, thus reducing susceptibility to infection.”
One clinical pearl in the discussion: “When considering treatment [for CDI], initial therapy with oral vancomycin should be considered instead of metronidazole, and treating for at least 21 days should also be considered [in patients with IBD due to]…lower rates of CDI recurrence.”
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
In this multicenter retrospective cohort (n=42), the authors examined the efficacy and safety of fecal microbiota transplantation (FMT) in immunocompromised (IC) children with Clostridioides difficile infection (CDI). Etiology of IC included: solid organ transplantation (18, 43%), malignancy (12, 28%), primary immunodeficiency (10, 24%), or other chronic conditions (2, 5%)
Key findings:
23 (55%) of FMT was delivered via colonoscopy, 17 (40%) were delivered via enteric tube, and 2 (5%) via capsule
Success rate was 79% after first FMT and 86% after 1 or more FMT.
There were serious adverse events (SAEs) in 13 out of 42 (31%) patients; 4 (9.5%) of which were likely treatment-related (all patients recovered). These events included cecal perforation, aspiration pneumonitis, diarrhea and fever. Given retrospective design of study, AEs were likely underreported
My take: Though there are the potential for significant adverse effects, FMT is effective in a high percentage of immunocompromised children with CDI.
I am happy to say that this is the last nightcall that I will have this year!
Today, I’ve compiled some of my favorite posts from the past year. I started this blog a little more than 10 years ago. I am grateful for the encouragement/suggestions from many people to help make this blog better. Also, I want to wish everyone a Happy New Year.
This good update provides a lot of useful information regarding fecal microbiota transplantation (FMT) and a word of caution regarding its future availability.
Key pointsregarding FMT:
Long-term safety remains unknown. FMT may lead to susceptibility to chronic inflammatory, allergic, and autoimmune diseases. “FMT has been associated with durable transmission of pro-carcinogenic bacteria from adult donors to pediatric recipients…although the long-term consequences…are unknown.”
Due to transfer of extended spectrum beta-lactamase (ESBL) E coli to 2 immunocompromised adult recipients, further screening of FMT was implemented.
Though there is no published evidence of SARS-CoV-2 fecal transmission, the FDA “advised additional precautions and testing in March 2020; “however, there are no molecular tests with stool…which have received emergency use authorization.” Hence, most FMT programs were on hold as of January 2021.
After 2021, OpenBiome, whose product was recently available again, is expected to stop distribution of FMT donor product due to increased costs of screening and the “promising biotherapeutics” that are in phase III trials.
Biotherapeutic is “loosely defined as drug therapy products where the active substance is extracted from a biological specimen.” The new products are likely to have “increased standardization, safety and practicality.”
The problem in pediatrics: none of these biotherapeutic products have started trials in children. This will lead to treatment problems. Even if one wanted to set up donor-directed FMT, it will be difficult to complete all of the screening recommended by the FDA. It could lead to self-administration by families with uncertain risks.
My take: My first reaction to this article: ‘Oh crap!’ It is sad and ironic that I will miss having available commercial stool for FMT.
Methods: A multicampus, retrospective cohort evaluation was conducted among patients aged ≤18 years with any history of clinical CDI and receiving systemic antibiotics in a subsequent encounter from 2013–2019. This study identified 30 and 44 patients received oral vancomycin prophylaxis (OVP) and no OVP, respectively. Eligible patients had to be >12 months of age and having at 3 unformed stools everyday.
OVP dosing: “vancomycin doses of 10 mg/kg (up to 125 mg per dose) every 12 hours during concomitant antibiotic use. OVP duration was intended to continue while on systemic antimicrobial agents and for 5 days after completion of antimicrobial agents (extended prophylaxis tail), but practice varied, and duration was ultimately left to the discretion of the provider.”
Key finding:
The incidence of CDI recurrence within 8 weeks of antibiotic exposure was significantly lower in patients who received OVP (3% vs 25%; P = .02) despite this group having notably more risk factors for recurrence. After adjustment in a multivariable analysis, secondary OVP was associated with less risk of recurrence (odds ratio, 0.10; 95% confidence interval, 0.01–0.86; P = .04).
This study is in agreement with studies in adults (Brown CC, et al. Oral Vancomycin for Secondary Prophylaxis of Clostridium difficile Infection. Ann Pharmacother. 2019 Apr;53(4):396-401). In this review, the authors state: “Variable dosing regimens and lack of safety data are limitations.. clinicians can consider vancomycin 125 mg orally once or twice daily in high-risk patients receiving broad-spectrum antibacterial agents.”
My take: In patients at high risk of recurrent CDI, OVP should be considered as secondary prophylaxis when receiving systemic antibiotics.
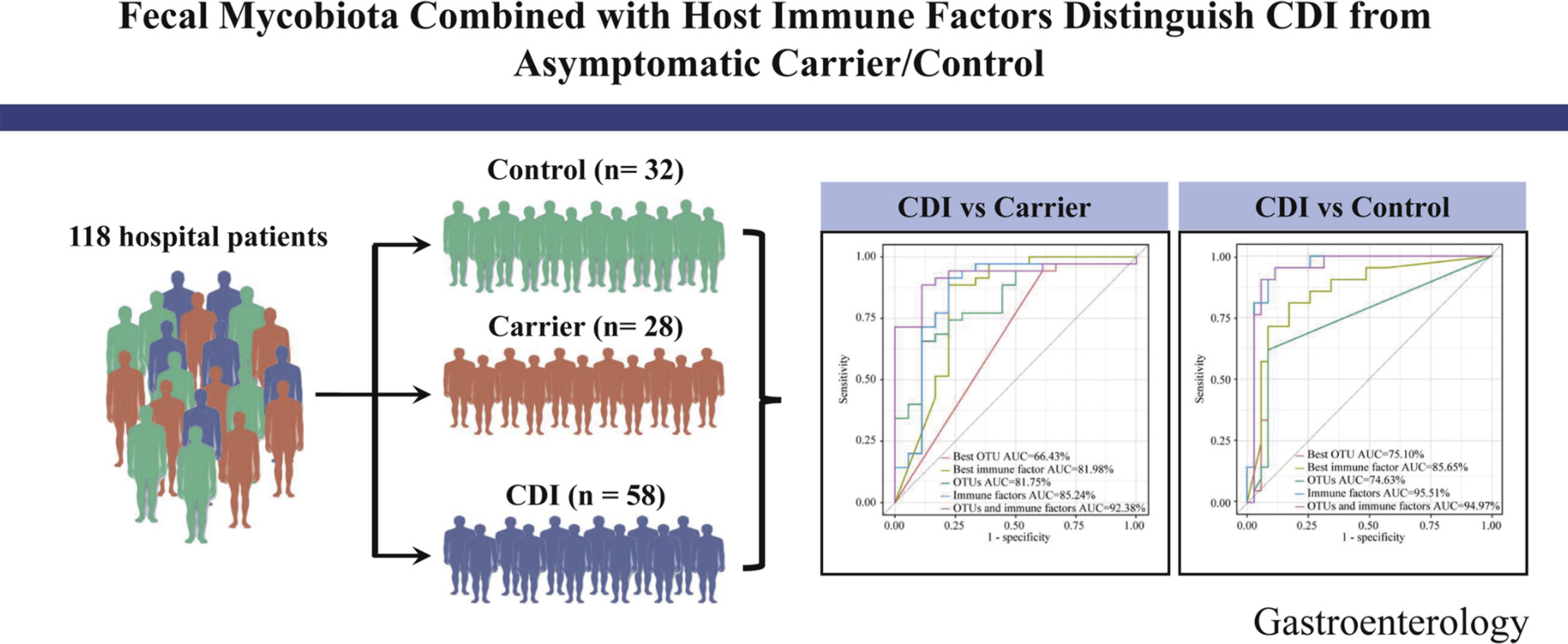
The ratio of Ascomycota to Basidiomycota was dramatically higher in patients with CDI than in Carrier and Control (P < .05).
Using 4 fungal operational taxonomic units combined with 6 host immune markers in the random forest classifier can achieve very high performance (area under the curve ∼92.38%) in distinguishing patients with CDI from Carrier.
My take: It is interesting that fecal fungal diversity (mycobiome), in addition to bacterial diversity, is reduced in those with Clostridium difficile infection (CDI) compared to both control groups and those with Clostridium difficile asymptomatic carriage.
In this prospective study (2012-2018) with 609 patients (median age 56 years), the authors studied long-term outcomes. Key findings:
At 1 year, 9.5% reported additional CDI episodes. Diarrhea occured in more than half of all patients, although it lasted for than a week in most patients.
Among 477 with long-term data, 188 patients post-FMT developed new medical conditions/symptoms.
Weight gain was reported by 46 patients (10.3%) post-FMT. In these patients, the median weight gained was 30 pounds (range, 10–70). Of these patients, 11 (23%) had preexisting obesity.
Approximately 3% of patients each reported new-onset diabetes mellitus and dyslipidemia, whereas 2.3% reported thyroid disease.
Gastrointestinal symptoms were the second most frequently reported (13.4%). New-onset IBS was reported by 4%, IBD by 0.3%, chronic diarrhea by 5.0%, and chronic constipation by 1.6% of patients.
Serious infections were reported by 11.8% of patients: CDI in 5.7%, Pneumonia in 4.5%, UTI in 1.8% and Sepsis in 1.2%. Median time to the infections was 29 months (range, 0–73) following FMT; only 1 patient reported an infection (CDI) within the first month after FMT.
No deaths were considered related to FMT
Limitation: no control group
My take (borrowed from authors): “FMT appears safe and effective, both in the short-term and long-term. Several new medical conditions were reported post-FMT, in particular, weight gain and IBS.”
Guideline recommends AGAINST using probiotics for prevention of C difficile infection (CDI)
Guideline cautions AGAINST testing individuals at low risk for CDI (eg. not having diarrhea)
Guideline recommends either vancomycin or fidaxomicin (lower CDI recurrence) for all cases of CDI and consideration of metronidazole for nonsevere cases. Fidaxomicin is recommended for CDI recurrence after vancomycin or metronidazole.
Guideline recommends combination of highly sensitive test and highly specific test for diagnosis of CDI. “CDI-related complications are rare in NAAT-positive, toxin EIA-negative patients, who, even when untreated, may have clinical courses similar to those without CDI…If both are positive, the diagnosis of CDI can be made reliably. If both are negative, CDI is unlikely. Discordant results when NAAT or GDH is positive and toxin EIA is negative require clinical evaluation and consideration of the possibility of colonization or that the patient has CDI but toxin levels are below the limits of detection (see below).