A recent issue of Clinical Gastroenterology and Hepatology focused solely on the clinical features and management of inflammatory bowel disease. Even for those with expertise in IBD, there is a lot of useful information and concise reviews of what is known.
Here are some of my notes from this issue (part 2)
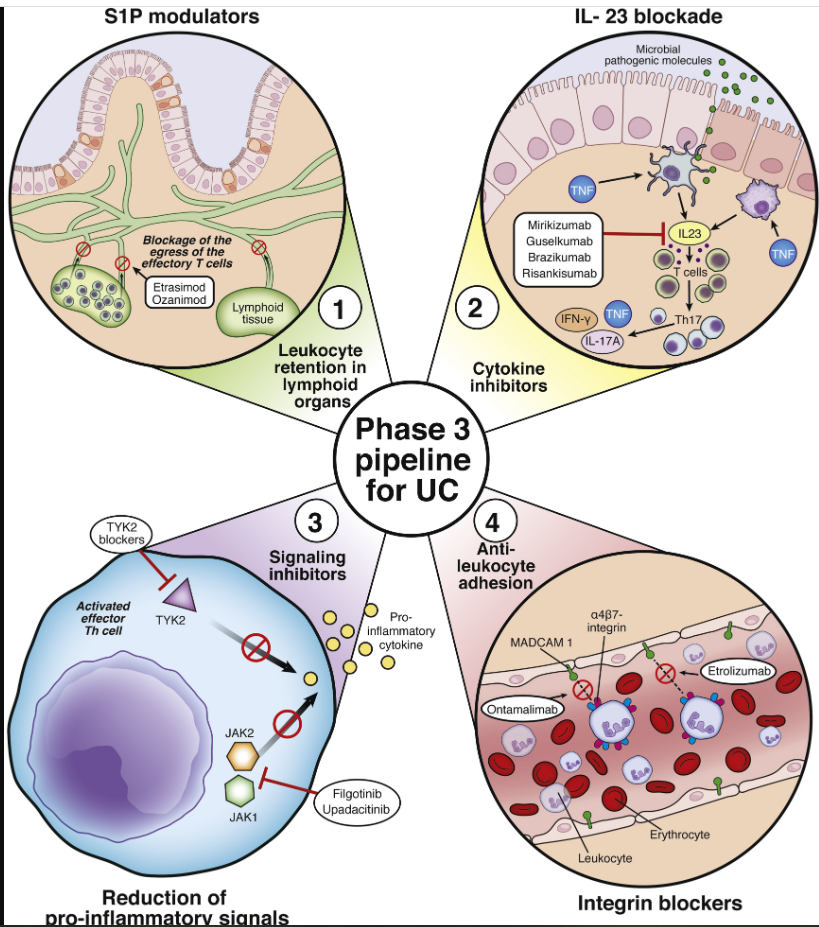
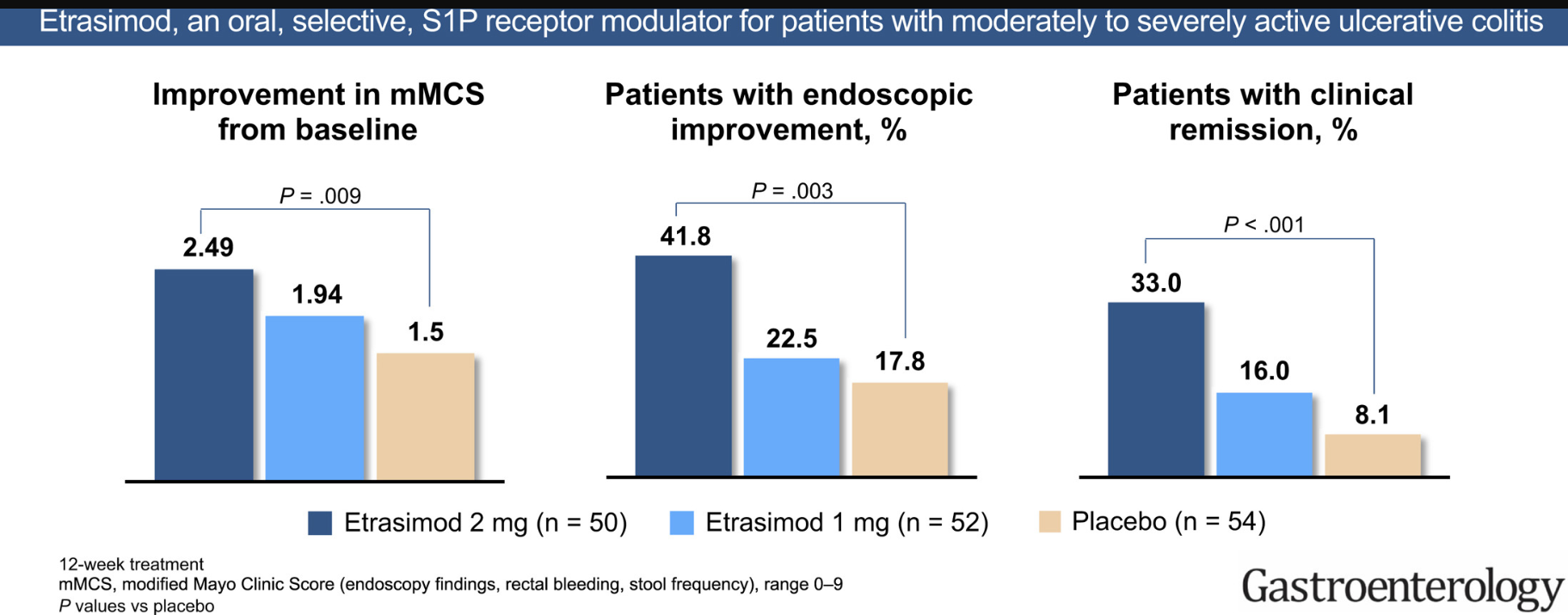
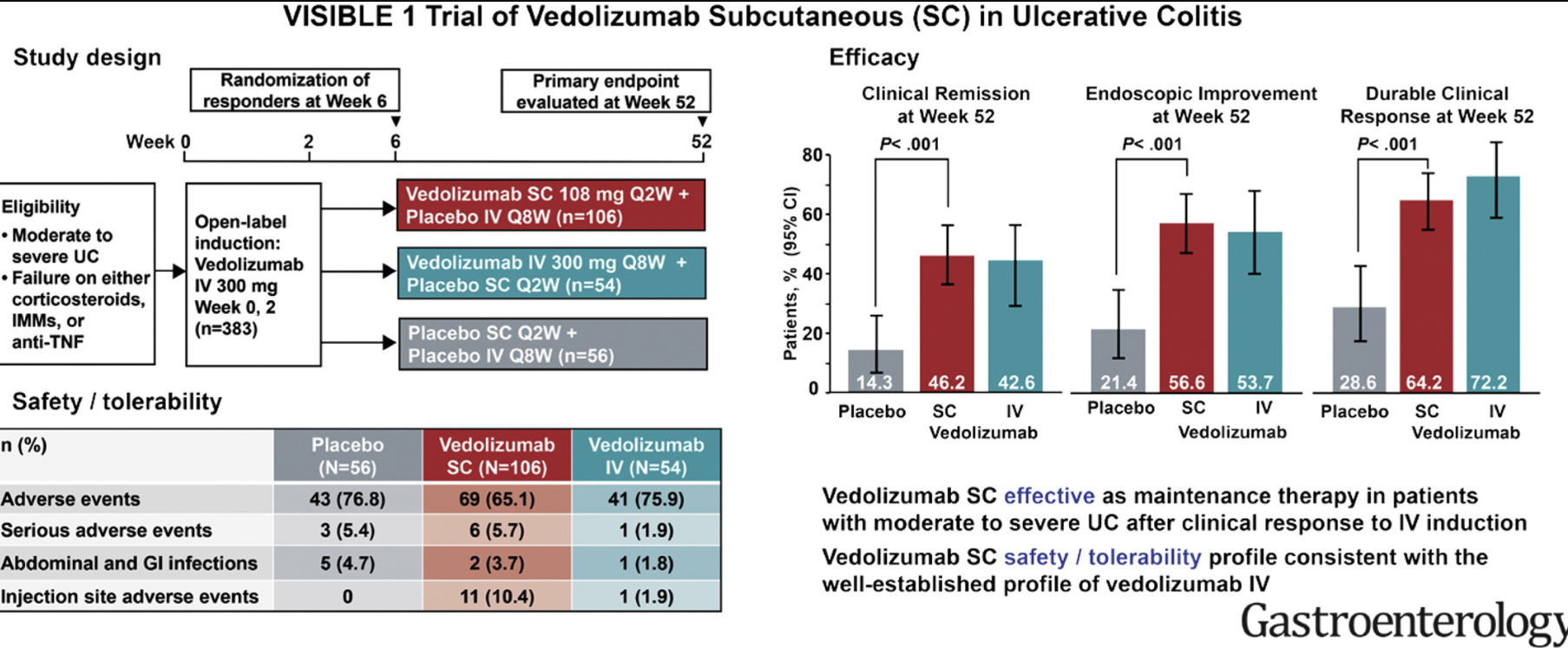
S Danese et al. Clinical Gastroenterol Hepatol: 2020; 18: 1280-90. Positioning Therapies in Ulcerative Colitis
This is a good article but recent AGA publications are probably better –there are some links below. One statement that was interesting: “the safety profile of vedolizumab seems even better than placebo in terms of risk of serious” adverse events. The authors favored infliximab in combination with azathioprine in those needing biologic therapy with moderate-severe UC.
Related blog posts:
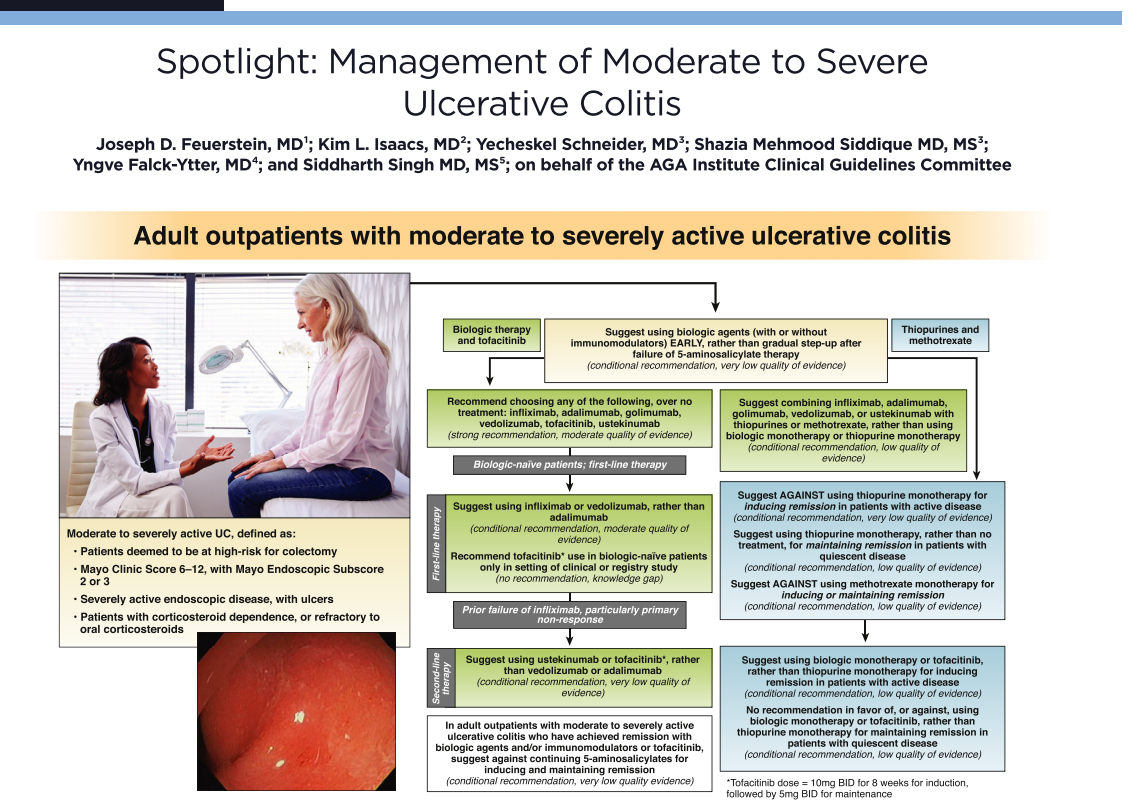
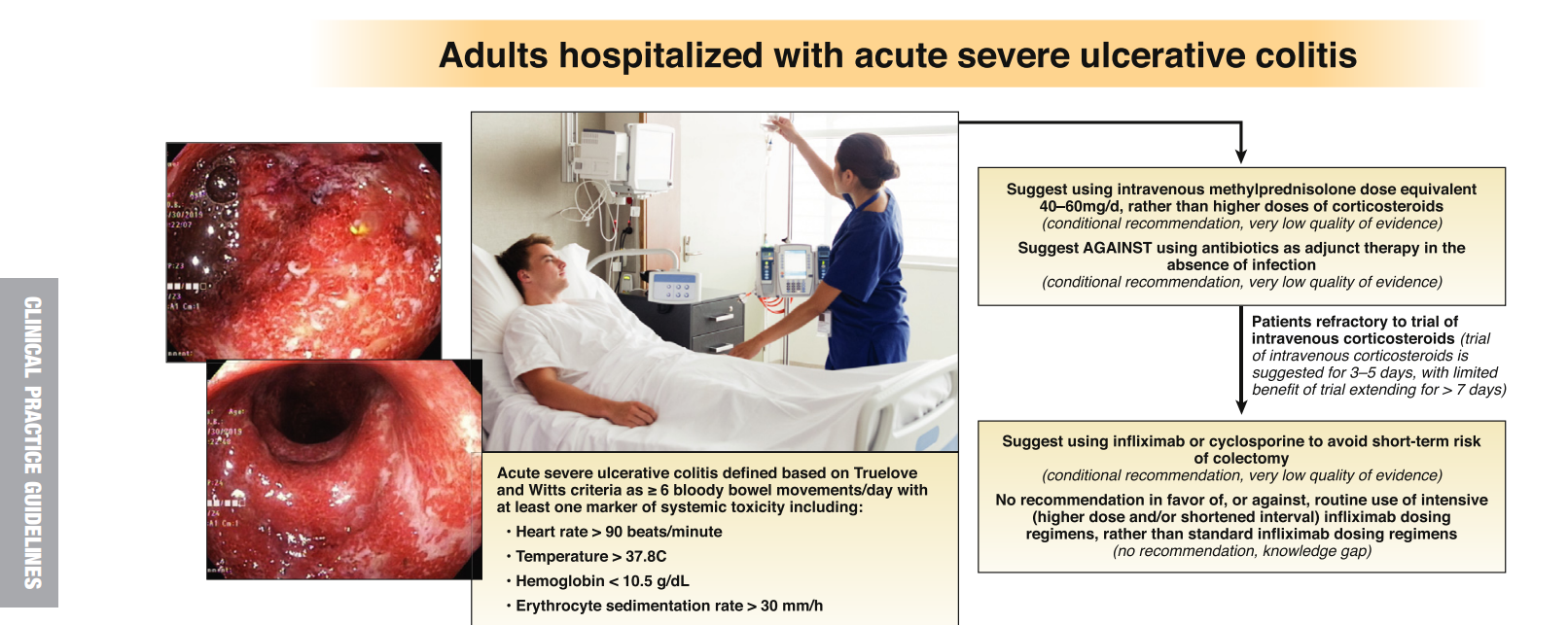
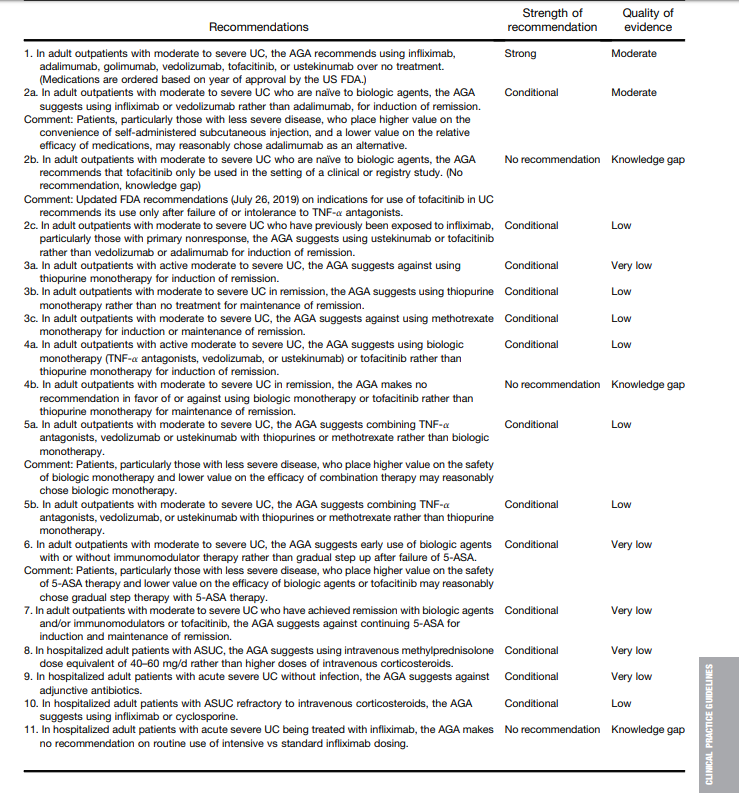
- AGA Guidelines: Moderate to Severe Colitis
- AGA Guidelines for Mild to Moderate Ulcerative Colitis
- Toronto Consensus: Practice Guidelines for Nonhospitalized Ulcerative Colitis
- Is There Renal Toxicity with Mesalamine Therapy for IBD? | gutsandgrowth
S Vermeire et al. Clinical Gastroenterol Hepatol: 2020; 18: 1291-9. How, When, and for Whom Should We Perform Therapeutic Drug Monitoring?
“Although reactive TDM, testing at time of loss of response, is widely accepted in practice, especially for anti–tumor necrosis factor antibodies, there are less data for the other monoclonal antibodies belonging to other classes. Besides reactive testing, there is a movement toward proactively adjusting biologic dosing to prevent loss of response, in keeping with the tight control philosophy of inflammatory bowel disease care.” The authors favor proactive monitoring: “we are now beginning to see with well-powered proactive TDM studies” that proactive monitoring can maximize the benefits of TDM with “the potential to maximize durability of biologics and improve the outcomes of IBD patients.”
Related blog posts:
- Can Therapeutic Drug Monitoring with Monotherapy Achieve Similar Results as Combination Therapy for IBD?
- Proactive Therapeutic Drug Monitoring -Different Time Points
- IBD Updates December 2019 | gutsandgrowth
- Briefly Noted: Induction Infliximab Levels Infliximab level ≥18 mcg/mL at week 6 was strongly associated with clinical and biologic response as well as achieving an infliximab level ≥5 mcg/mL at week 14 (AUC 0.85).
- Is Standard Infliximab Dose Too Low in Pediatrics?
- Combination Therapy Study Points to Central Role of Adequate Drug Levels
- Can Therapeutic Drug Monitoring with Monotherapy Achieve Similar Results as Combination Therapy for IBD? | gutsandgrowth The authors utilized TDM at week 10. If the IFX level was <20 mcg/mL, the dose and frequency of infliximab were both adjusted. If the level was between 20 & 25, either the frequency was adjusted or no adjustment, and if the level was >25, then no adjustment in dosing was performed.
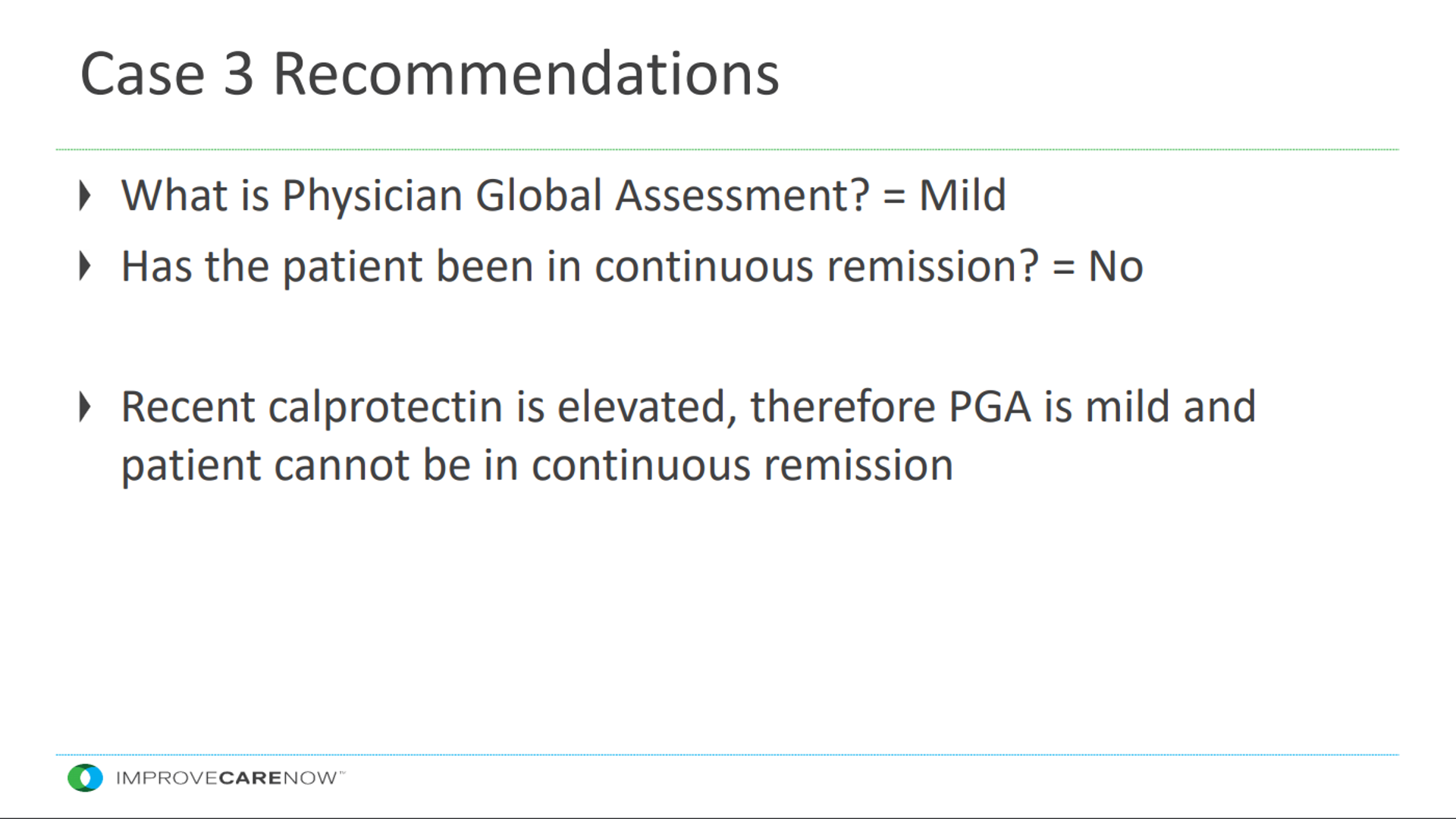
PS Dulai et al. Clinical Gastroenterol Hepatol: 2020; 18: 1300-8. How Do We Treat Inflammatory Bowel Diseases to Aim For Endoscopic Remission?
The initial part of this article reviews treatment targets -resolution of symptoms and resolution of endoscopic damage. The algorithm provides the authors’ suggested approach:
- At initiation of therapy, patients should have a full assessment. In addition to ileocolonoscopy, for patients with CD, the authors recommend cross-sectional imaging.
- After treatment initiation, the authors recommend biomarker assessment every 3 months. Mucosal assessment can occur 6-9 months after treatment initiation.
- For UC, the authors note that fecal calprotectin (FC) “appears to be more stratightforward, and a cutoff of 250 mcg/g can be used reliably across all scenarios to make treatment adjustments.” Though, they recommend endoscopic confirmation prior to transition to a biologic or small molecule therapy.
- For CD, the authors suggest making treatment adjustments in those with FC >250 mcg/g and in those with lower values, followup colonoscopy is recommended.
- The authors note that in the post-operative setting with CD, mucosal inflammation precedes symptomatic activity and “waiting for symptoms to emerge may unnecessary allow for disease progression.”
- The authors suggest that tighter disease control will reduce disease-related complications, while acknowledging a lack of prospective clinical trials.
- One thorny issue: :”For CD: it remains unclear what degree of residual mucosal healing is acceptable to impact important outcomes such as CD-related complications, hospitalizations, and surgeries.”
Related blog posts:
- What is the Calprotectin Threshold for Disease Progression with Crohn’s Disease?
- Prospective Monitoring of Calprotectin for Crohn’s Disease …
- What Treat-to-Target Could Look Like in Crohn’s Disease
- Treating to Target | gutsandgrowth
M Allocca et al. Clinical Gastroenterol Hepatol: 2020; 18: 1309-23. Use of Cross-Sectional Imaging for Tight Monitoring of Inflammatory Bowel Diseases
“Computed tomography is limited by the use of radiation, while the use of magnetic resonance enterography (MRE) is limited by its cost and access. There is growing interest in bowel ultrasound that represents a cost-effective, noninvasive, and well-tolerated modality in clinical practice, but it is operator dependent… Diffusion-weighted imaging (DWI) is a MR imaging technique that increasingly is used in both IBD and non-IBD conditions and has been shown to be a valuable and accurate tool for assessing and monitoring IBD activity.
L Beaugerie et al. Clinical Gastroenterol Hepatol: 2020; 18: 1324-35. Predicting, Preventing, and Managing Treatment-Related Complications in Patients With Inflammatory Bowel Diseases
The first part of this article reviews potential adverse effects from the medications used for IBD treatment, noting in Table 1 that there are not complications to monitor for with both vedolizumab and ustekinumab.
The article reviews infections, vaccination strategies and issues related to malignancy Some of the recommendations:
- vaccine against pneumococcus should be given before patients begin immunosuppressive therapy
- physicians should consider giving patients live vaccines against herpes zoster (in adults) before they begin immunosuppressive therapy or a recombinant vaccine, when available, at any time point during treatment
- sun protection and skin surveillance from the time of diagnosis are recommended
- despite concerns about therapy, the authors note that “the extensive use of immunosuppressive therapy leads to a substantial decrease in the incidence of IBD complications, with a globally favorable benefit-risk ratio, which can be optimized further thanks to a good degree of awareness and knowledge of drug complications.”
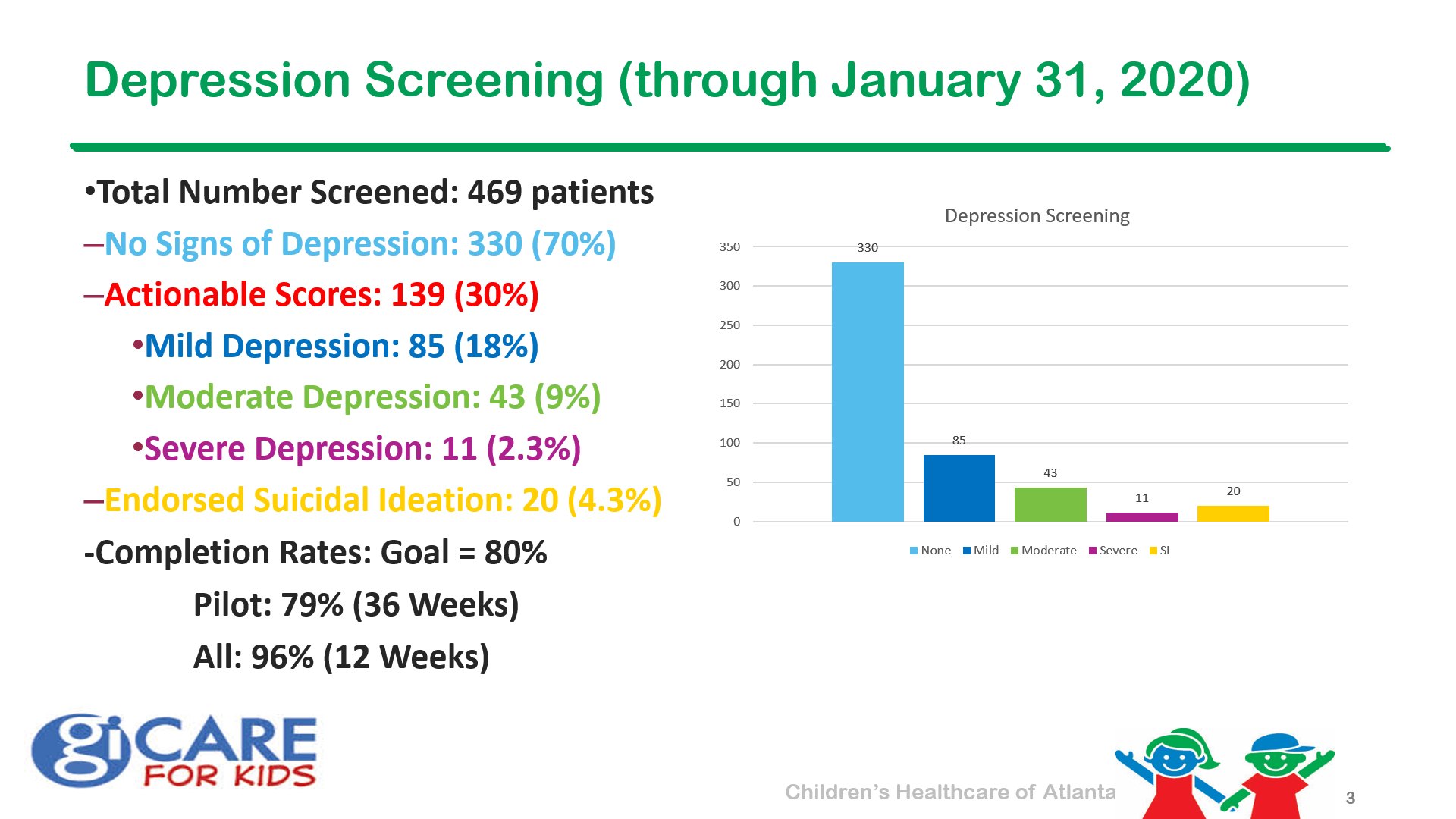
It is interesting that this article (and the entire issue) does not address mental health concerns related to the diagnosis of IBD. This likely creates more morbidity and complications than most of the other issues that are discussed.
Above: Why did the picture go to jail? Because it was framed.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.