
M Jachs et al. Clin Gastroenterol Hepatol 2023; 21: 2318-2326. Open Access! Carvedilol Achieves Higher Hemodynamic Response and Lower Rebleeding Rates Than Propranolol in Secondary Prophylaxis
Associated editorial: J Bosch. Clin Gastroenterol Hepatol 2023; 21:2195-2196. Open Access! Carvedilol as Best β-Blocker for Secondary Prophylaxis of Variceal Bleeding: Are We There, or Not Yet?
Key findings:
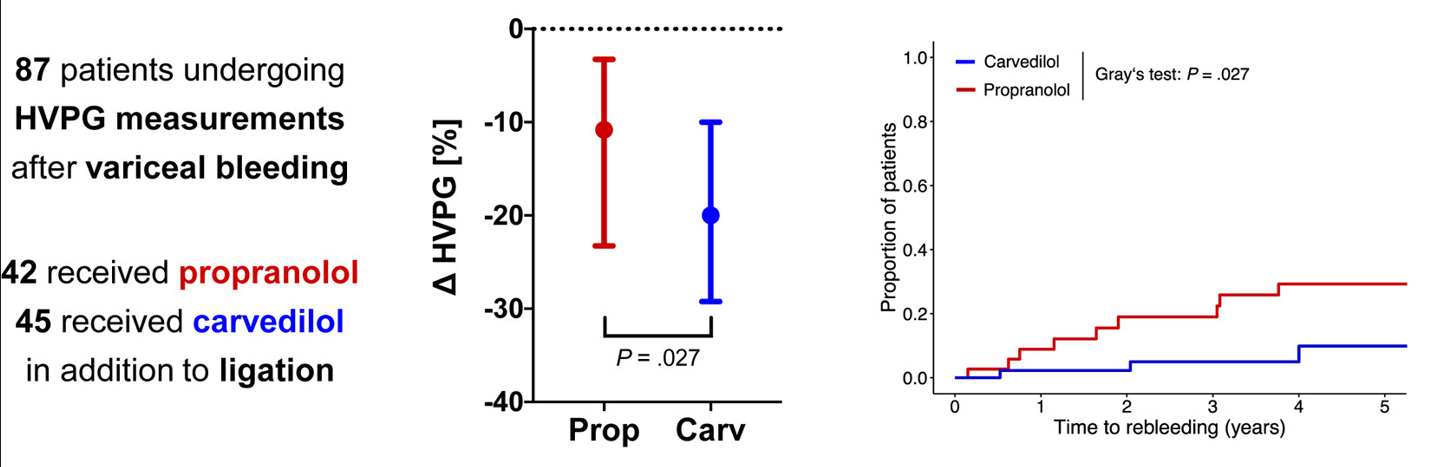
- In a retrospective cohort comprising 87 adult patients receiving NSBB (non-selective beta blocker) in addition to band ligation after variceal bleeding, carvedilol induced more profound decreases in hepatic venous pressure gradient compared with propranolol. The higher rate of chronic hepatic venous pressure gradient response to carvedilol (53.3% vs 28.6%; P = .034) was paralleled by lower rates of variceal rebleeding, liver-related death, and further nonbleeding decompensation.
In the discussion and the editorial, it is noted that there is high-quality evidence that carvediol is superior for primary variceal prophylaxis in adults. “Carvedilol increasingly is used for the prevention of variceal bleeding, 2 and, based on the recent landmark PREDESCI study, overall hepatic decompensation/ascites3 in compensated cirrhosis, because it induces HVPG response (a ≥10% decrease in HVPG is sufficient in primary prophylaxis17) in up to 75% of patients vs 50% when using propranolol. However, it induces more pronounced decreases in blood pressure, which may be detrimental in patients with (refractory) ascites.15“
Though there are concerns about dropping blood pressure, the editorial notes that “up to two-thirds of patients with compensated cirrhosis” have high blood pressure. The editorial concludes that “the study still strongly suggests that carvedilol is at least as safe as propranolol…. I am in complete agreement with the authors in suggesting that carvedilol is likely to represent the best NSBB in the treatment of portal hypertension regardless of the clinical scenario, including prevention of decompensation, ascites, first bleeding, or recurrent bleeding.” The author notes that the “recent Baveno VII recommendations declare carvedilol as the preferred NSBB, and support its use in all compensated patients with direct (HVPG ≥10 mm Hg) or indirect signs of clinically significant portal hypertension.”(J Hepatol. 2022; 76: 959-974. Baveno VII: renewing consensus in portal hypertension)
My take: In adults, Carvediol is the best NSBB for portal hypertension. In children, who may be more prone to hypotension, more data is needed.
Related blog posts:
- New Paradigm in Treating Varices and Cirrhosis Management (in Adults) (2021)
- #NASPGHAN19 Liver Symposium (excellent presentation by Dr. Romero on varices in children and portal hypertension)
- Transient Elastography in Pediatric Liver Disease
- Elastography-Accuracy in Children (great picture of Lake Moraine)










{kind=link}