I am a pediatric gastroenterologist at GI Care for Kids (previously called CCDHC) in Atlanta, Georgia. The goal of my blog is to share some of my reading in my field more broadly. In addition, I wanted to provide my voice to a wide range of topics that often have inaccurate or incomplete information.
Before starting this blog in 2011, I would tear out articles from journals and/or keep notes in a palm pilot. This blog helps provide an updated source of information that is easy to access and search, along with links to useful multimedia sources.
I was born and raised in Chattanooga. After graduating from the University of Virginia, I attended Baylor College of Medicine. I completed residency and fellowship training at the University of Cincinnati at the Children’s Hospital Medical Center. I received funding from the National Institutes of Health for molecular biology research of the gastrointestinal tract.
During my fellowship, I had the opportunity to work with some of the most amazing pediatric gastroenterologists and mentors. Some of these individuals included Mitchell Cohen, William Balistreri, James Heubi, Jorge Bezerra, Colin Rudolph, John Bucuvalas, and Michael Farrell. I am grateful for their teaching and their friendship. During my training with their help, I received a nationwide award for the best research by a GI fellow.
I have authored numerous publications/presentations including original research, case reports, review articles, and textbook chapters on various pediatric gastrointestinal problems. In addition, I have been recognized by Atlanta Magazine as a "Top Doctor" in my field multiple times.
Currently, I am the vice chair of the section of nutrition for the Georgia Chapter of the American Academy of Pediatrics. In addition, I am an adjunct Associate Clinical Professor of Pediatrics at Emory University School of Medicine. Other society memberships have included the North American Society for Pediatric Gastroenterology Hepatology and Nutrition (NASPGHAN), American Academy of Pediatrics, the Food Allergy Network, the American Gastroenterology Association, the American Association for the Study of Liver Diseases, and the Crohn’s and Colitis Foundation.
As part of a national pediatric GI organization called NASPGHAN (and its affiliated website GIKids), I have helped develop educational materials on a wide-range of gastrointestinal and liver diseases which are used across the country. Also, I have been an invited speaker for national campaigns to improve the evaluation and treatment of gastroesophageal reflux disease, celiac disease, eosinophilic esophagitis, hepatitis C, and inflammatory bowel disease (IBD). Some information on these topics has been posted at my work website, www.gicareforkids.com, which has links to multiple other useful resources.
I am fortunate to work at GI Care For Kids. Our group has 17 terrific physicians with a wide range of subspecialization, including liver diseases, feeding disorders, eosinophilic diseases, inflammatory bowel disease, cystic fibrosis, DiGeorge/22q, celiac disease, and motility disorders. Many of our physicians are recognized nationally for their achievements. Our group of physicians have worked closely together for many years. None of the physicians in our group have ever left to join other groups. I have also worked with the same nurse (Bernadette) since I moved to Atlanta in 1997.
For many families, more practical matters about our office include the following:
– 14 office/satellite locations
– physicians who speak Spanish
– cutting edge research
– on-site nutritionists
– on-site psychology support for abdominal pain and feeding disorders
– participation in ImproveCareNow to better the outcomes for children with inflammatory bowel disease
– office endoscopy suite (lower costs and easier scheduling)
– office infusion center (lower costs and easier for families)
– easy access to nursing advice (each physician has at least one nurse)
I am married and have two sons (both adults). I like to read, walk/hike, bike, swim, and play tennis with my free time.
I do not have any financial relationships with pharmaceutical companies or other financial relationships to disclose. I have helped enroll patients in industry-sponsored research studies.
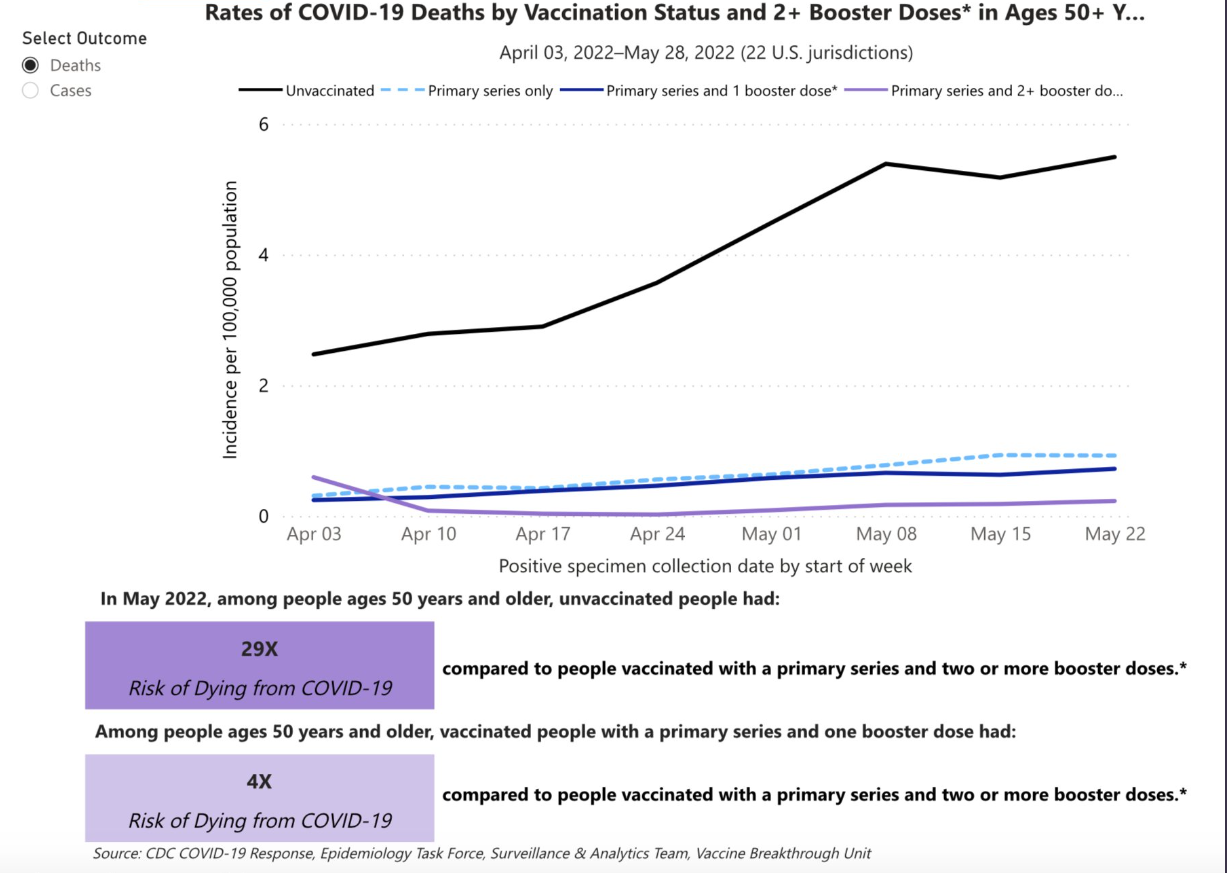
Getting boosted is important for those >50 years. There was a 29-fold reduction when comparing 2 boosters vs unvaccinated and a 4-fold reduction when comparing 2nd booster vs 1 booster. CDC: Rates of COVID-19 Cases and Deaths by Vaccination Status
Inborn errors of metabolism -bile acids: BASD, bile acid conjugation defects, peroxisomal defects
Inborn errors of metabolism -carbohydrates: galactosemia, hereditary fructose intolerance
Inborn errors of metabolism -amino acids: tyrosinemia type 1
Key Points:
Low GGT genetic disorders (>25 genetic mutations) include canalicular transporter defects, basolateral transporter defects, intracellular trafficking defects, defects of cytoskeletal and tight junction protein, transaldolase deficiency, bile duct paucity, and inborn errors of metabolism.
The authors note that the timing and utility of a liver biopsy is changing due to the advent of rapid molecular testing.
Potential treatments are reviewed include ursodeoxycholic acid, IBAT inhibitors, cholic acid, biliary diversion, and liver transplantation.
Multidisciplinary evaluation is often needed in patients with Alagille. 87% have cardiac anomalies, up to 36% have/develop cerebral vasculopathy, 21% develop post-transplant renal dysfunction, and 22% develop spontaneous or procedure-associate systemic bleeding (need for hematology consultation). In addition, pathologic fractures are common; one report found the rate of femur fractures was 50 times that in the general population which is likely related to intrinsic bone defects (as well as cholestasis).
My take: With the widespread availability of genetic testing which is needed due to the numerous etiologies, the diagnosis of ‘idiopathic’ chronic cholestasis has decreased and targeted therapies have emerged.
In this multicenter retrospective and prospective study was conducted in 32 children with cryptogenic intrahepatic cholestasis, whole exome sequencing identified 6 with MYO5B mutations. The most common signs were pruritus, poor growth, hepatomegaly, jaundice, and hypocholic stools.
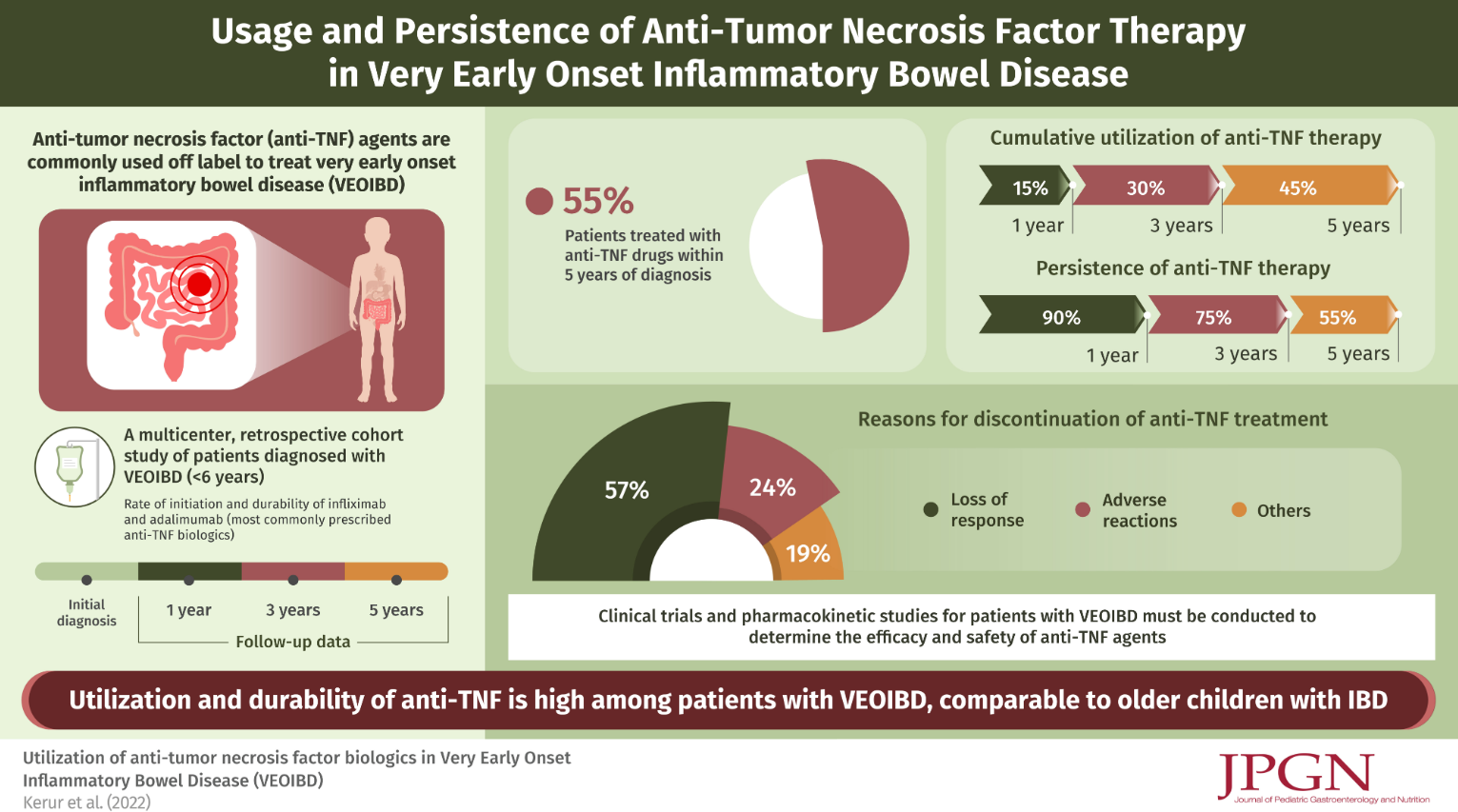
In this retrospective study, 120 of 294 children with VEO-IBD (diagnosed 2008 and 2013, PRO-KIDS network) received anti-TNF therapy (96% infliximab). 101 of these 120 had adequate data recorded. It is noted that additional data on this cohort has been previously published (IBD Updates: Outcomes of VEO-IBD, PIANO Study Update, and Insurance-Disparity Relationship). Key findings:
Anti-TNF durability was 90% at 1 year, 75% at 3 years, and 55% at 5 years
Patients with Crohn’s disease had better durability than those with UC/IBD-U (Hazard ratio 0.17)
The most common reason for discontinuation of anti-TNF were loss of response in 24 (57%) children
67 (66%) received combined therapy with an immunomodulator and this was associated with improved anti-TNF durability (Hazard ratio 0.30). However, authors note this was in era preceding widespread therapeutic drug monitoring.
The majority of children in the current study did not undergo testing for monogenic mutations
My take: Data for use of anti-TNF agents in this age group (< 6 yrs) has been limited. This study suggests similar effectiveness of anti-TNF agents in VEO-IBD compared to older groups. Given this groups increased risk for monogenic mutations, it is still a good idea, if feasible, to test for these disorders.
The authors, representing the American Board of Internal Medicine (ABIM), assert that “there aren’t always right answers, but some answers are clearly wrong.” In their commentary, they note that there is “growing allegiance to crowd-endorsed ‘facts.'” Yet, they expect physicians to adhere to higher standards; however, they note the inherent conflict between speech that can be prohibited by licensing boards and speech protected by the First Amendment.
Dietary supplements are another part of medicine with rampant misinformation. In fact, there is nearly ubiquitous misinformation through advertisements across all media segments. Americans spent ~$55 billion on dietary supplements in 2020. This commentary discusses a Senate bill, the Dietary Supplement Listing Act of 2022, which ostensibly would improve this situation.
However, this is NOT the case. This bill requires manufacturers to provide the FDA with a product’s name, ingredients and health claims. It mandates the FDA create a searchable database. What the legislation doesn’t do:
Provide the the FDA with a mechanism to confirm a product’s ingredients
Enable regulation of misleading health claims
Stop the promotion and sale of supplements with dangerous ingredients
Allow the FDA to remove products from its registry determined to have unlawful ingredients and remove products deemed hazardous
My take: This legislation needs to be strengthened to limit deception. In its current form, this registry would appear to confer FDA oversight to dietary supplements (which is minimal) and paradoxically legitimize dietary supplements .
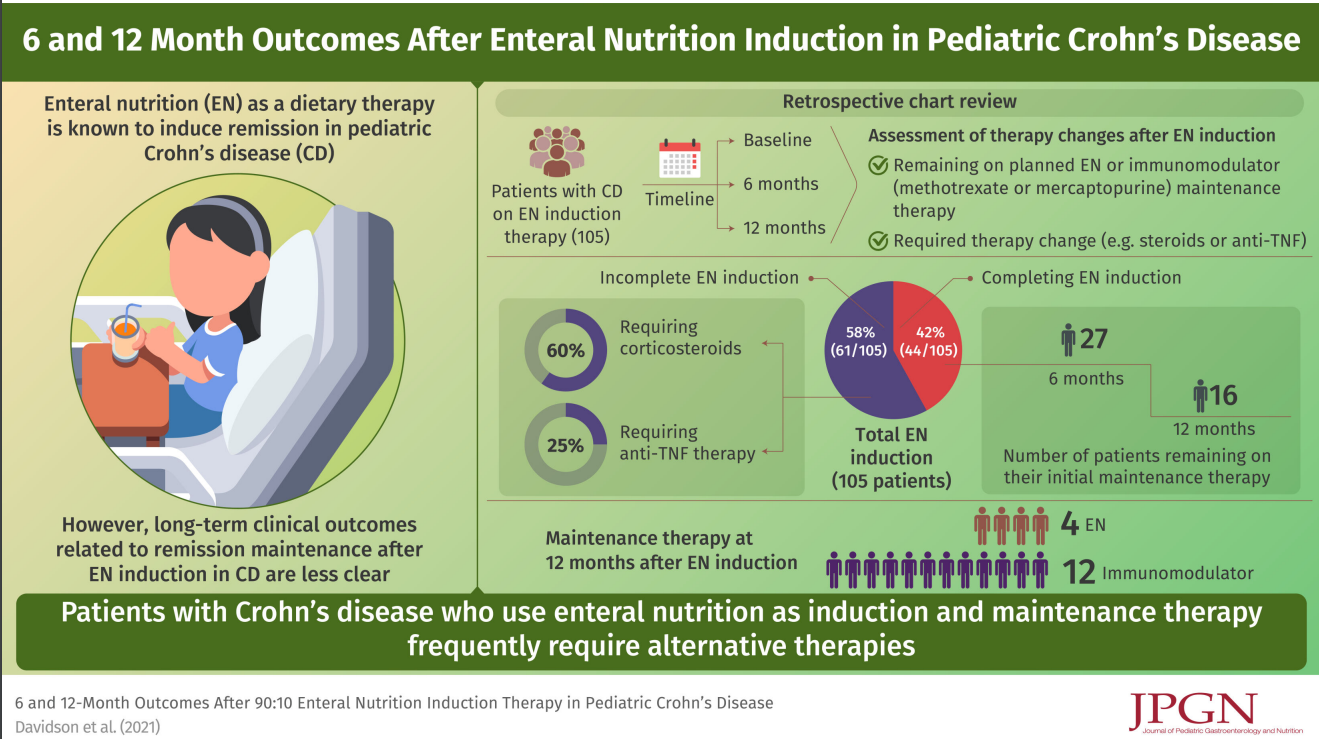
In this retrospective study (2013-2018), the authors examined outcomes in 105 children treated with a 90:10 enteral feeds (90% formula).
Key findings:
44/105 (42%) patients completed 8–12 weeks
After induction, 18 continued EN maintenance with a 80:20 then 70:30 protocol; however, only 10 remained on EN at 6 months and 4 remained on EN at 12 months
The associated editorial (pg: 1-2) make several points:
While EEN is effective and safe, this study and others have shown poor adherence
It is unclear how exclusive enteral nutrition needs to be in order to be effective. And, many patients instructed to receive 90% of their calories as formula are likely consuming higher amounts of table foods
We still are working out which foods need to be excluded
My take: This study shows that EEN is NOT a practical option for most patients beyond induction. Only 4 patients remained on EEN at 12 months.
In pooled analyses, multivitamin use was significantly associated with a lower incidence of any cancer (odds ratio [OR], 0.93 [95% CI, 0.87-0.99]…However, the evidence for multivitamins had important limitations
Limited evidence suggested some supplements may be associated with higher risk of serious harms (hip fracture [vitamin A], hemorrhagic stroke [vitamin E], and kidney stones [vitamin C, calcium])
Vitamin and mineral supplementation was associated with little or no benefit in preventing cancer, cardiovascular disease, and death, with the exception of a small benefit for cancer incidence with multivitamin use.
Beta-carotene: supplementation associated with increased risk of lung cancer and cardiovascular mortality.
Vitamins D and E: not associated with increased or decreased risk of all-cause mortality, cardiovascular disease or cancer. In summary, no benefit.
Based on these findings, the United States Preventive Services Taskforce 1) recommends against the use of beta-carotene or vitamin E supplements for the prevention of cardiovascular disease or cancer and 2) states that there’s insufficient evidence to assess the benefits or harms of multivitamins or other single or paired nutrient supplements for the prevention of cardiovascular disease or cancer.
My take: Most people will not benefit from vitamin supplements and should focus on developing a healthy diet. Certain populations, including pregnant women and those with intestinal disorders, do need additional vitamins.
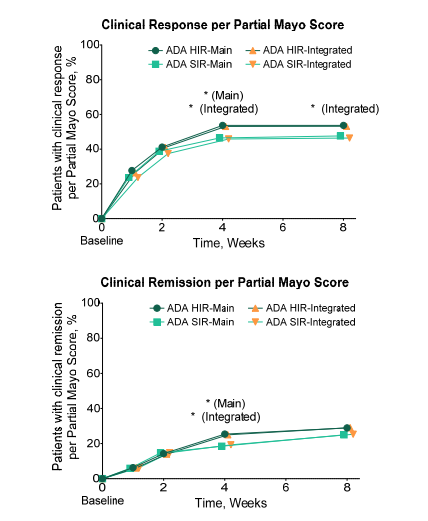
The main component of this double-blind, randomized (no placebo) study allocated 512 patients with ulcerative colitis to a higher induction regimen (HIR) of adalimumab and 340 patients to a standard induction regimen (SIR). A maintenance phase continued with 374 main patients who were clinical responders at week 8 (n=757 who completed induction). The study results are presented in a confusing manner, in part because of a subgroup from Japan as well as a great deal of data from both the induction phase and the maintenance phase.
Key findings:
In the main study, 13.3% vs 10.9% of patients receiving the higher induction regimen (HIR) vs standard induction regimen (SIR) achieved clinical remission (full Mayo score ≤2 with no subscore >1) at week 8 (induction primary end point; P = .265)
Among week-8 responders, 39.5% vs 29.0% receiving 40 mg ew vs 40 mg eow achieved clinical remission at week 52 (maintenance primary end point; P = .069).
Figure S2 below shows that approximately 50% of patients treated with adalimumab had a clinical response at week 8
My takes on this study:
Fairly low response to adalimumab: the clinical remission rate for adalimumab is low at week 8 (10-13%) and the 8-week response rate is less than 50%
Higher doses during induction were not helpful & did not result in significantly better responses at week 8
Therapeutic drug monitoring was not beneficial in this study
Higher doses during maintenance were associated with improved responses: patients receiving weekly adalimumab during maintenance treatment had improved week 52 remission. The editorial (pages 1831-1832) note that this effect was demonstrated in those with “elevated C-reactive protein, low albumin, extensive UC or long disease burden”
Figure S2: Clinical response was defined as Partial Mayo Score decrease from baseline ≥ 2 and ≥ 30% plus ≥ 1-point decrease from baseline in rectal bleeding subscore or absolute rectal bleeding subscore of 0 or 1. Clinical remission was defined as Partial Mayo Score ≤ 2 with no subscore > 1. ADA, adalimumab; HIR, higher induction regimen; SD, standard deviation; SIR, standard induction regimen
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
This retrospective study reviewed 395 CD patients received ustekinumab therapy (79 CD-ASD (autoimmune skin disease), 316 CD-none). ASD included atopic dermatitis, eczema, psoriasis/psoriaform dermatitis and alopecia. The skin disease group also included those with cutaneous manifestations of Crohn’s disease: erythema nodosum, pyoderma gangrenosum, pyostomatitis vegetans, Sweet’s syndrome, granulomatous vasculitis, and leukocytoclastic vasculitis. 55 of the 79 with CD-ASD had psoriatic disease, 20 had eczema, 11 had erythema nodosum, 8 had pyoderma gangrenosum.
Key findings:
Ustekinumab had greater efficacy in CD-ASD when evaluated by fecal calprotectin (P = .0337) and CRP (P = .078). For calprotectin, the values decreased by 61% after at least 5 months of therapy (394 to 164) in the CD-ASD group compared to 11% in the group without skin disease (365 to 265)
The CD-ASD group also showed better outcomes in Likert scores of endoscopy (P = .016), histopathology (P = .074), and imaging (P = .094).
My take: Ustekinumab appears to be particularly effective in patients with concurrent skin disease.
Preoperative TNFi exposure was not associated with postoperative infectious complications in a large prospective multicenter cohort. Any infection (18.1% vs 20.2%, P = .469) and SSI (12.0% vs 12.6%, P = .889) rates were similar in patients currently exposed to TNFis and those unexposed.