A recent yard sign from my wife for neighborhood walkers during the pandemic
P Ducrotte el al (Gastroenterol 2020; 158: 506-14, editorial 461-3) examined the use of an implanted gastric electrical stimulation (GES) in 172 patients in a randomized crossover trial (mean age 45 years). GES device was implanted and left unactivated until patients were randomized in a double-blind manner to receive stimulation (for 4 months) or not. Patients had vomiting that was either idiopathic, postsurgical or associated with diabetic gastroparesis (n=72).
Key findings:
- A significant decrease in vomiting occurred with the device on based on a nonvalidated vomiting score. During the ON period, vomiting was improved with score of 2.2 compared to vomiting score of 1.8 with device off. 30.6% of patients reported at least a 1 point improvement with device ON compared to device OFF. However, 16.5% of patients reported improvement with device OFF compared to device ON.
- Gastric emptying was not accelerated during treatment (device on) compared to no treatment
- GES was NOT associated with increased quality of life
- GES was not associated with improved nutritional parameters
- Adverse effects included pain (n=26) or infection (n=16) at the insertion site of GES; 3 patients required GES removal.
My take (from editorial): “Taking into account the modest magnitude of therapeutic benefit, the cost of the treatment and the potential for adverse events with GES, it seems advisable to exhaust all (symptomatic) therapeutic options” beforehand.
Related blog posts:
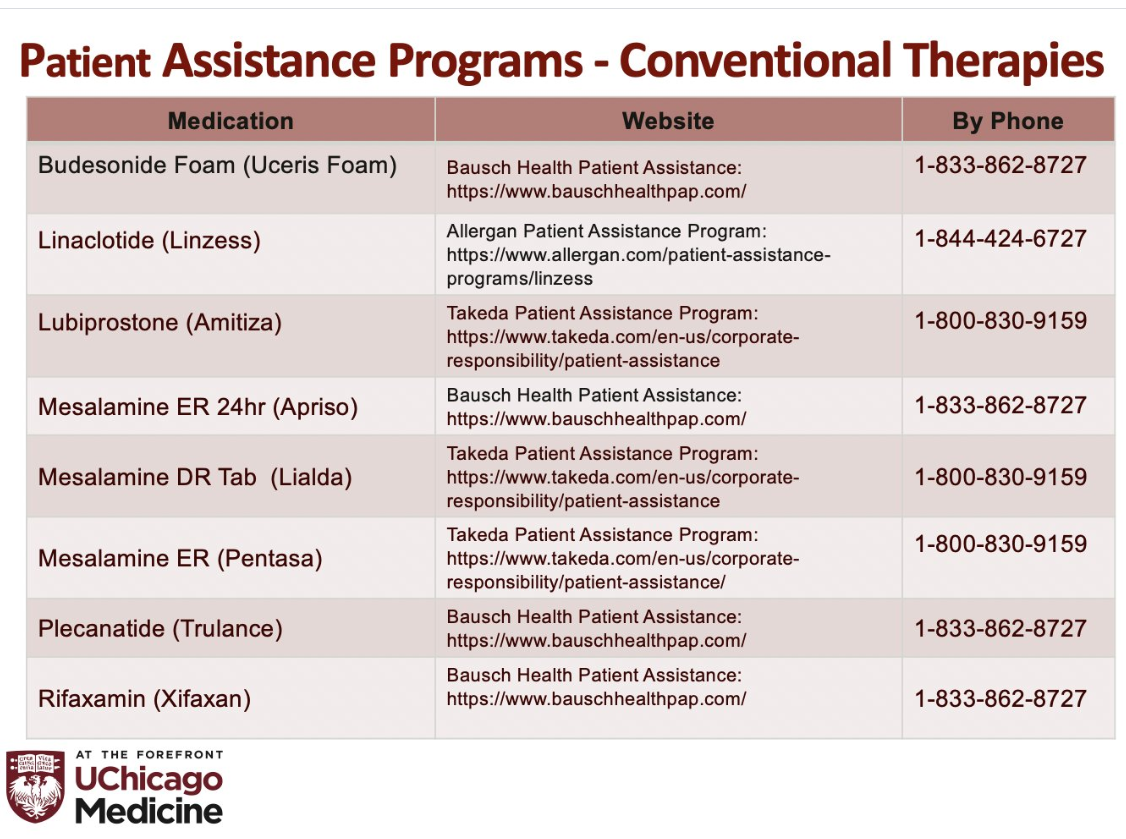
IBD Resources (from David Rubin, MD):


COVID-19 March 2020: MMWR Report (Link to report from Bryan Vartabedian 33mail)
- March 1-28 2020, 84% of hospitalized U.S. patients had underlying diseases -he most common being obesity, hypertension, chronic lung disease, diabetes mellitus, and cardiovascular disease.
- Hospitalization rates increased with age, with a rate of 0.3 (per 100,000) in persons aged 0–4 years, 0.1 in those aged 5–17 years, 2.5 in those aged 18–49 years, 7.4 in those aged 50–64 years, and 13.8 in those aged ≥65 years