In Pediatrics, supplement 3 summarizes 76 articles: Synopsis Book: Best Articles Relevant to Pediatric Allergy, Asthma and Immunology
Some of the studies that are most relevant to pediatric GI doctors I am reviewing for this blog over the next few days.
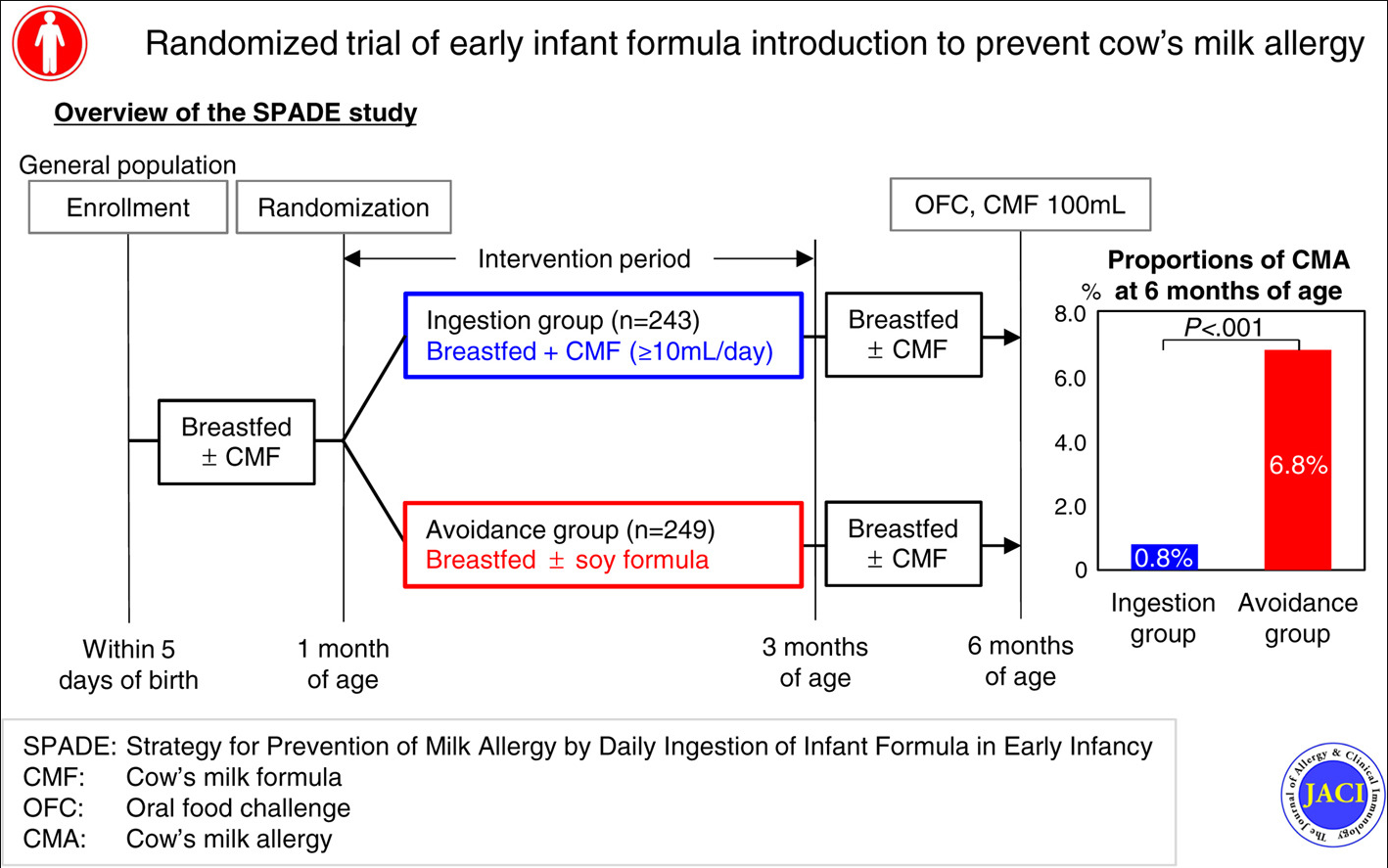
T Sakihara et al. J Allergy Clin Immunol 2021; 147: 224-232.e8. Randomized trial of early infant formula introduction to prevent cow’s milk allergy
In this randomized trial, infants (n=491 enrolled) in Japan were randomly allocated to ingest at least 10 mL of CMF (cow’s milk formula) daily (ingestion group) or avoid CMF (avoidance group) between 1 and 2 months of age. In the avoidance group breast-feeding was supplemented with soy formula as needed. Oral food challenge was performed at 6 months of age to assess CMA development. Continuous breast-feeding was recommended for both groups until 6 months of age.
Key findings:
- There were 2 CMA cases (0.8%) among the 242 members of the CMF ingestion group and 17 CMA cases (6.8%) among the 249 participants in the avoidance group (risk ratio = 0.12; 95% CI = 0.01-0.50; P < .001).
- Approximately 70% of the participants in both groups were still being breast-fed at 6 months of age.
My take: This study adds to the growing body of evidence that early introduction of allergenic foods lowers the likelihood of developing food allergies.
Related blog posts:
- Peanut Allergy Prevention Guidelines | gutsandgrowth
- LEAP-ON Study: Early Peanuts Prevent Allergies | gutsandgrowth
- The “EAT” Study | gutsandgrowth
- The Peanut Story -From NEJM Blog
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.