My notes from Georgia Chapter of CCFA’s conference. There could be errors of omission, transcription and/or errors in context based on my understanding.
Sandy Kim, MD –Children’s Hospital of Pittsburgh
Diet in Inflammatory Bowel Disease: Food for Thought
This was a terrific lecture –though much of the topic has been reviewed recently in this blog: Dietary Therapy for Inflammatory Bowel Disease.
Key points:
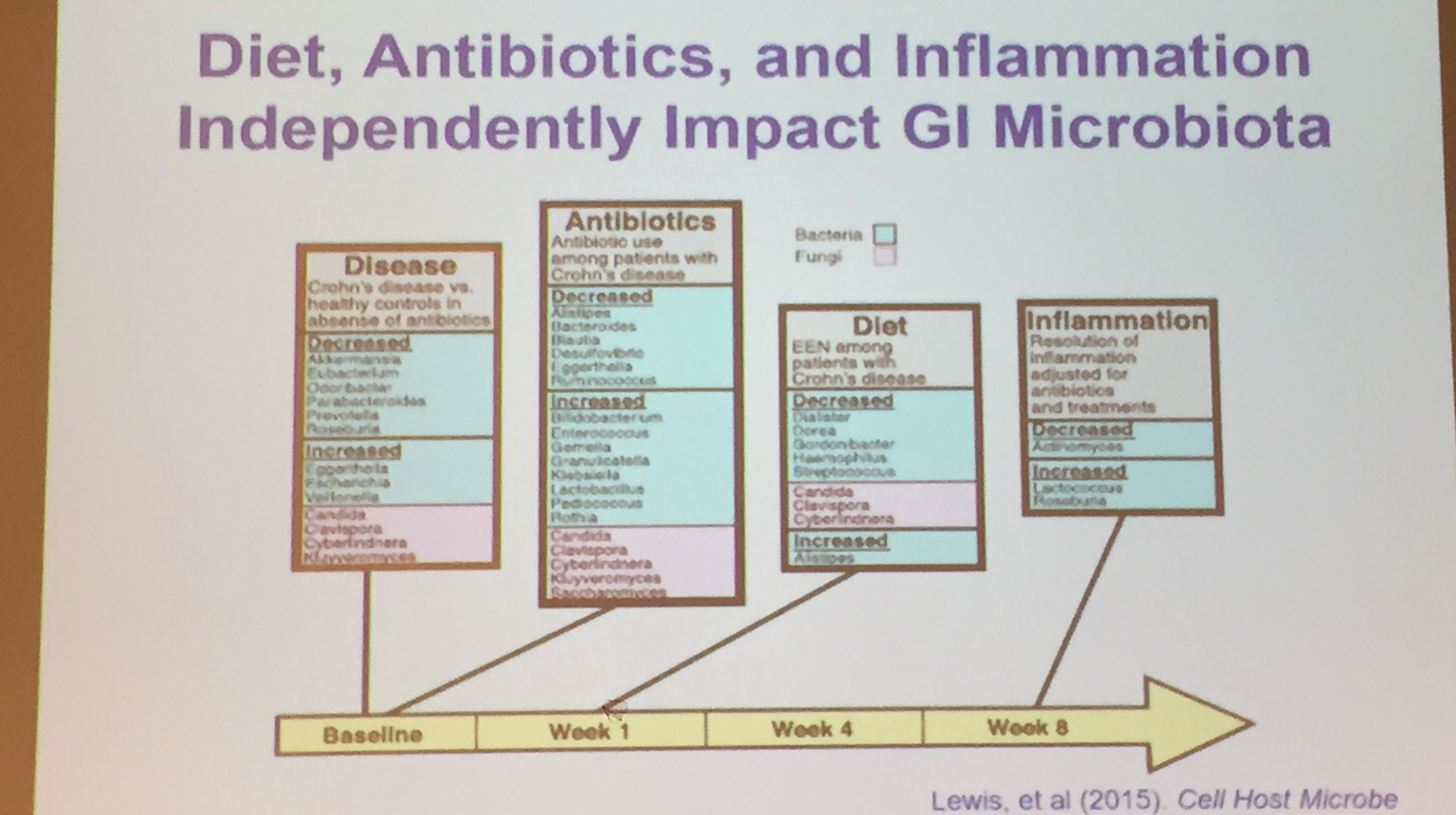
- Changes in diet can change microbiome quickly, within 24 hrs
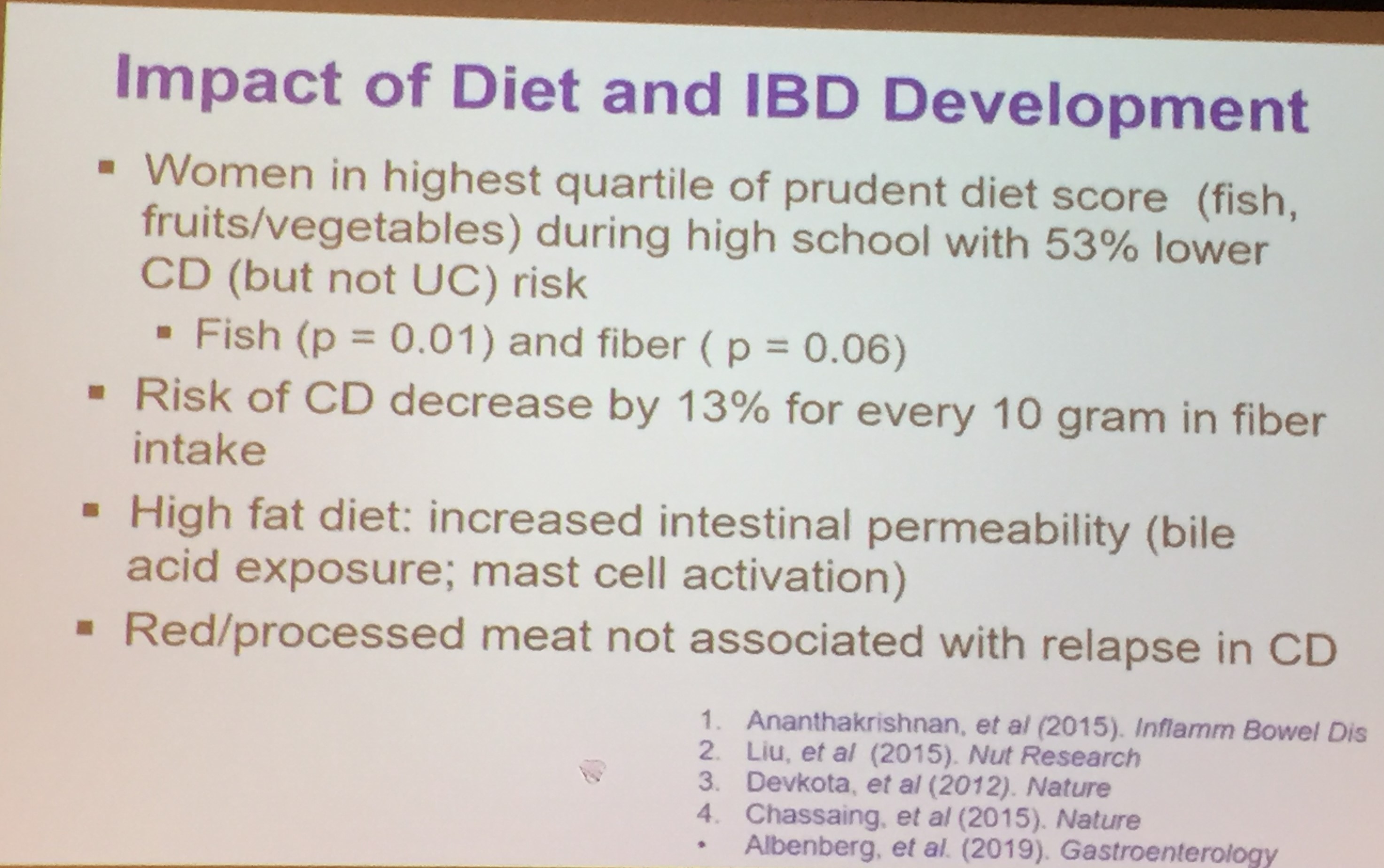
- Some diets (eg. more fruit/vegetables/fish) may help lower risk of developing IBD
- Dietary therapy, especially exclusive enteral nutrition (EEN), is effective therapy for Crohn’s disease
- Why does EEN work? It is not clear. There are some changes in microbiome but decrease or little change overall in microbial diversity
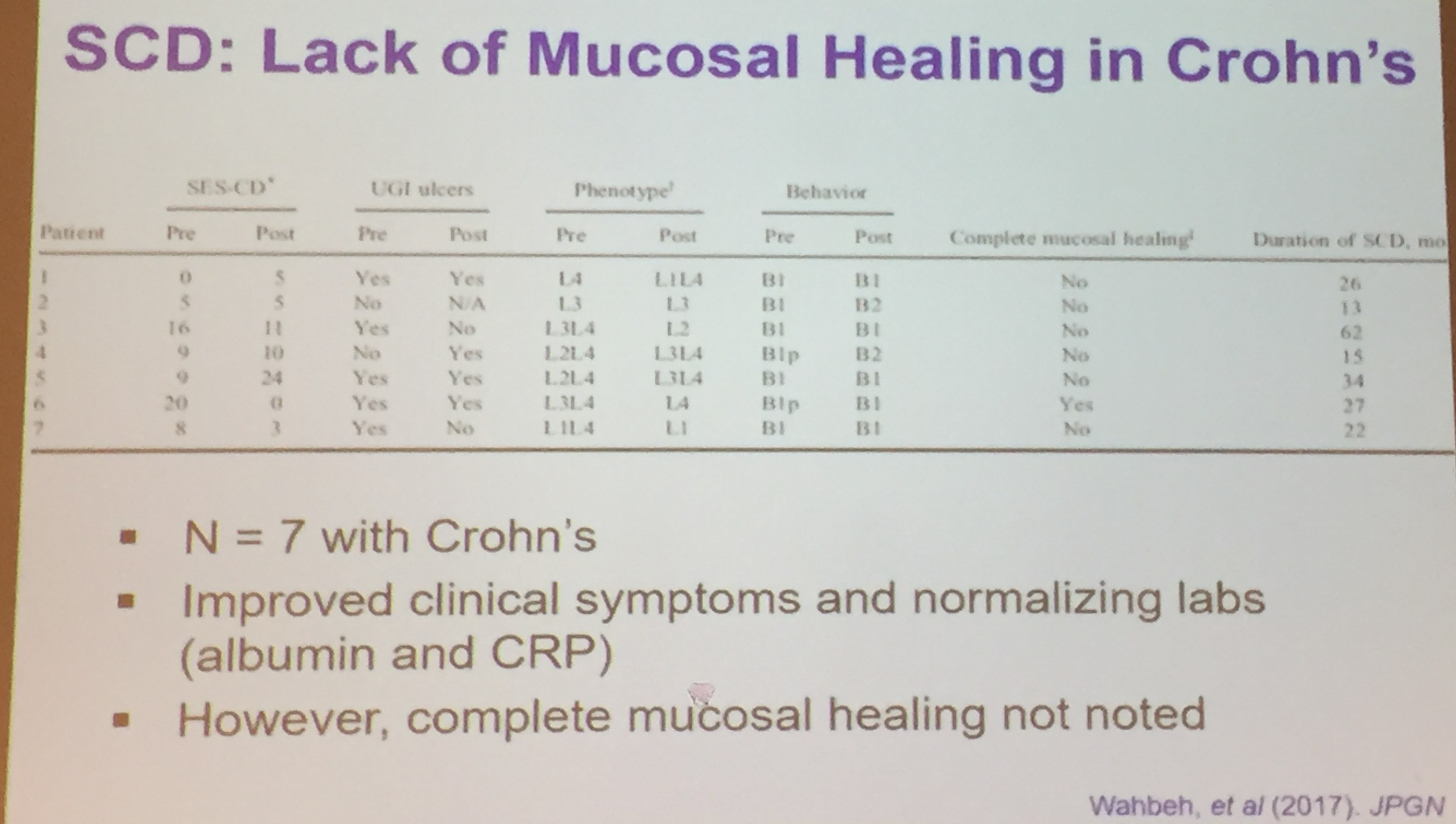
- Reviewed newer dietary approaches: SCD (www.nimbal.org), CD-TREAT, Crohn’s Disease Exclusion Diet


Related blog posts:
- Good Food and Bad Food for Crohn’s Disease -No Agreement | gutsandgrowth
- Pushing the Boundaries on Dietary Therapy for Crohn’s Disease: CD-TREAT
- IBD Briefs August 2019: CD Exclusion Diet
- Position Paper: Nutrition in Pediatric IBD
- Specific Carbohydrate Diet | gutsandgrowth
- Disappointing Results from SCD Diet (small study)
- Crohn’s Disease with Isolated Colonic Involvement Less Responsive to EEN
- Practical Advice on Enteral Nutrition | gutsandgrowth
- Head-to-Head: Enteral Nutrition vs. anti-TNF
Frank Farraye, MD –Mayo Clinic
Health Maintenance in the Adult Patient with IBD
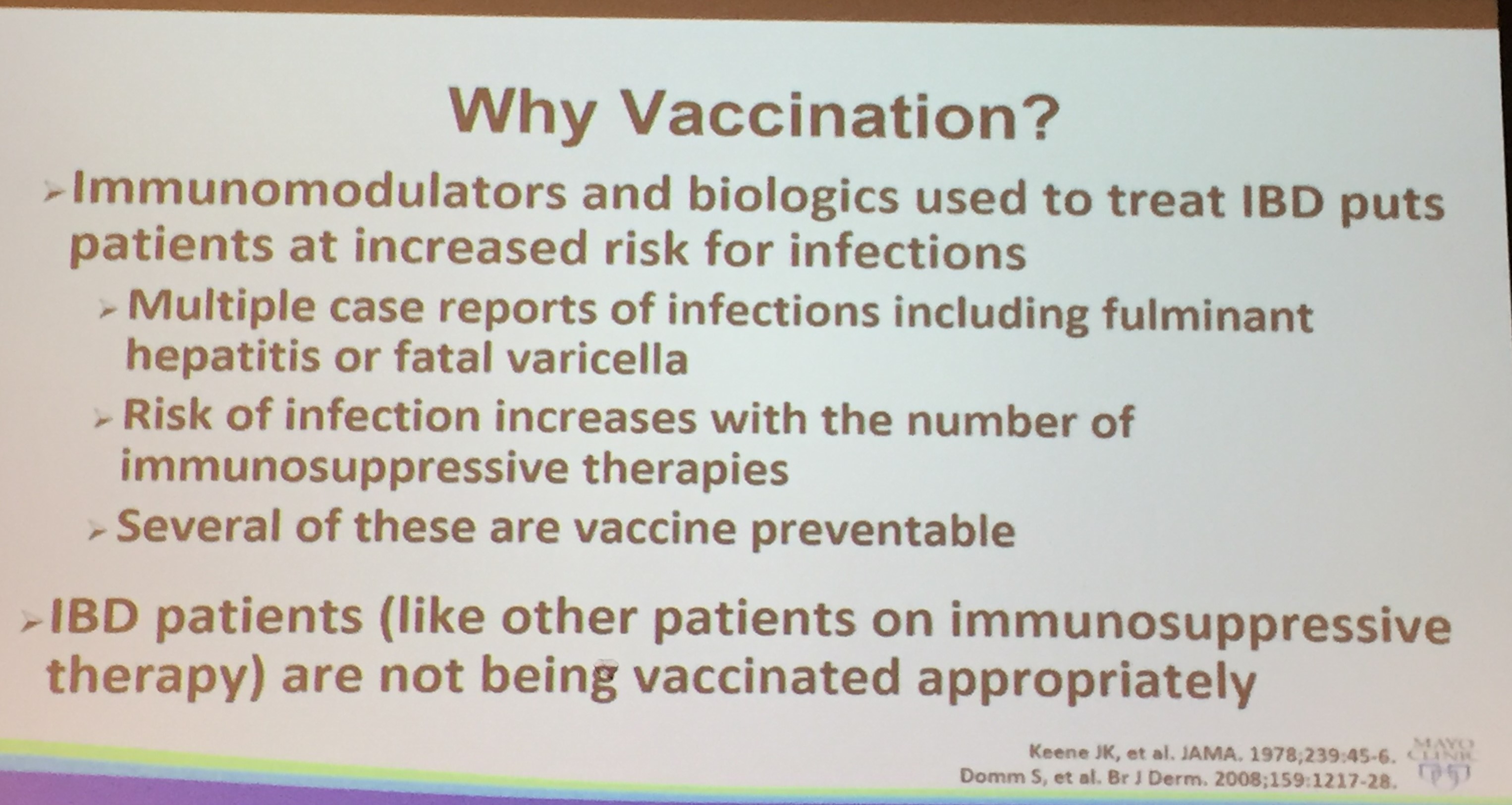
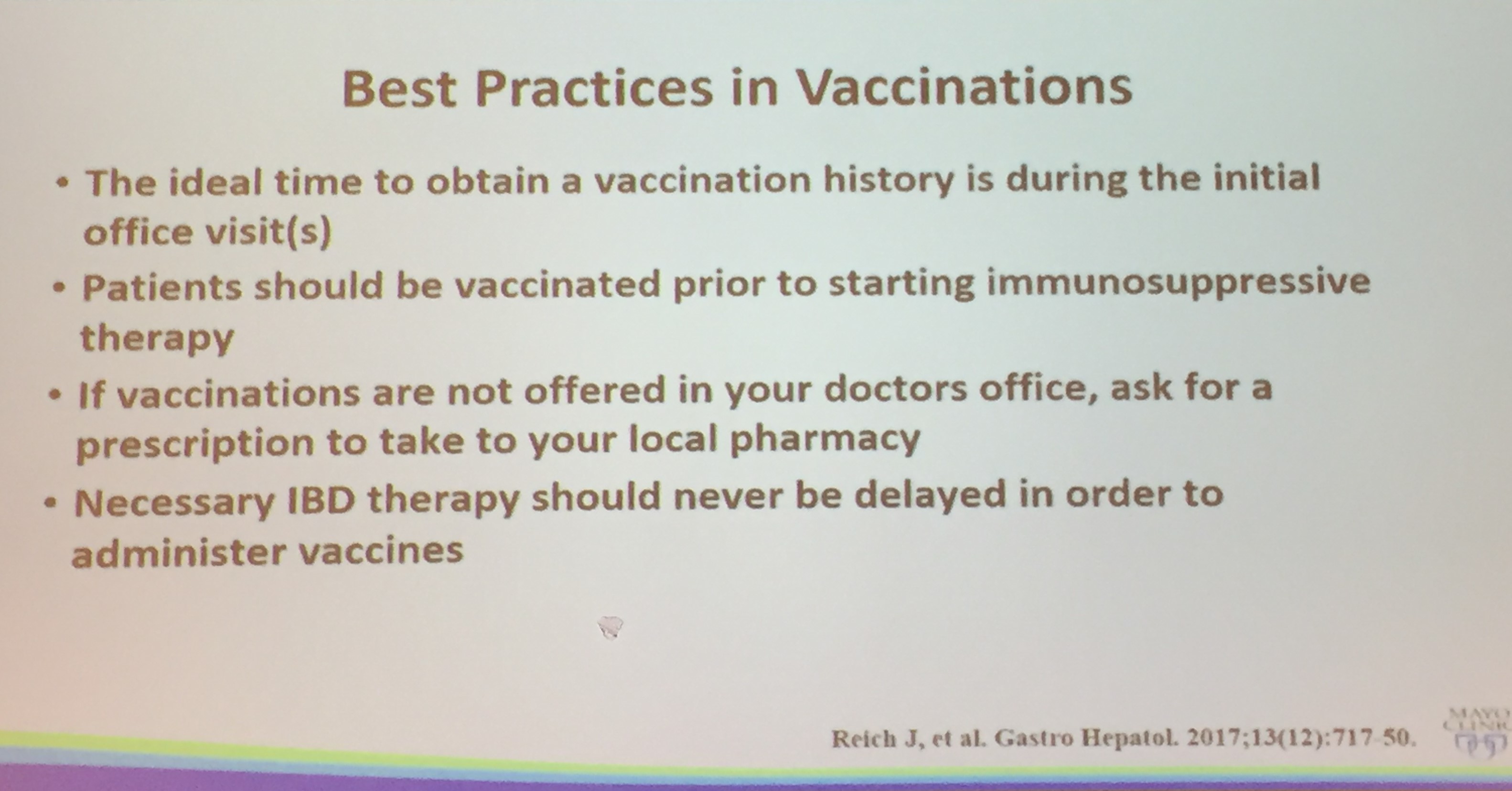
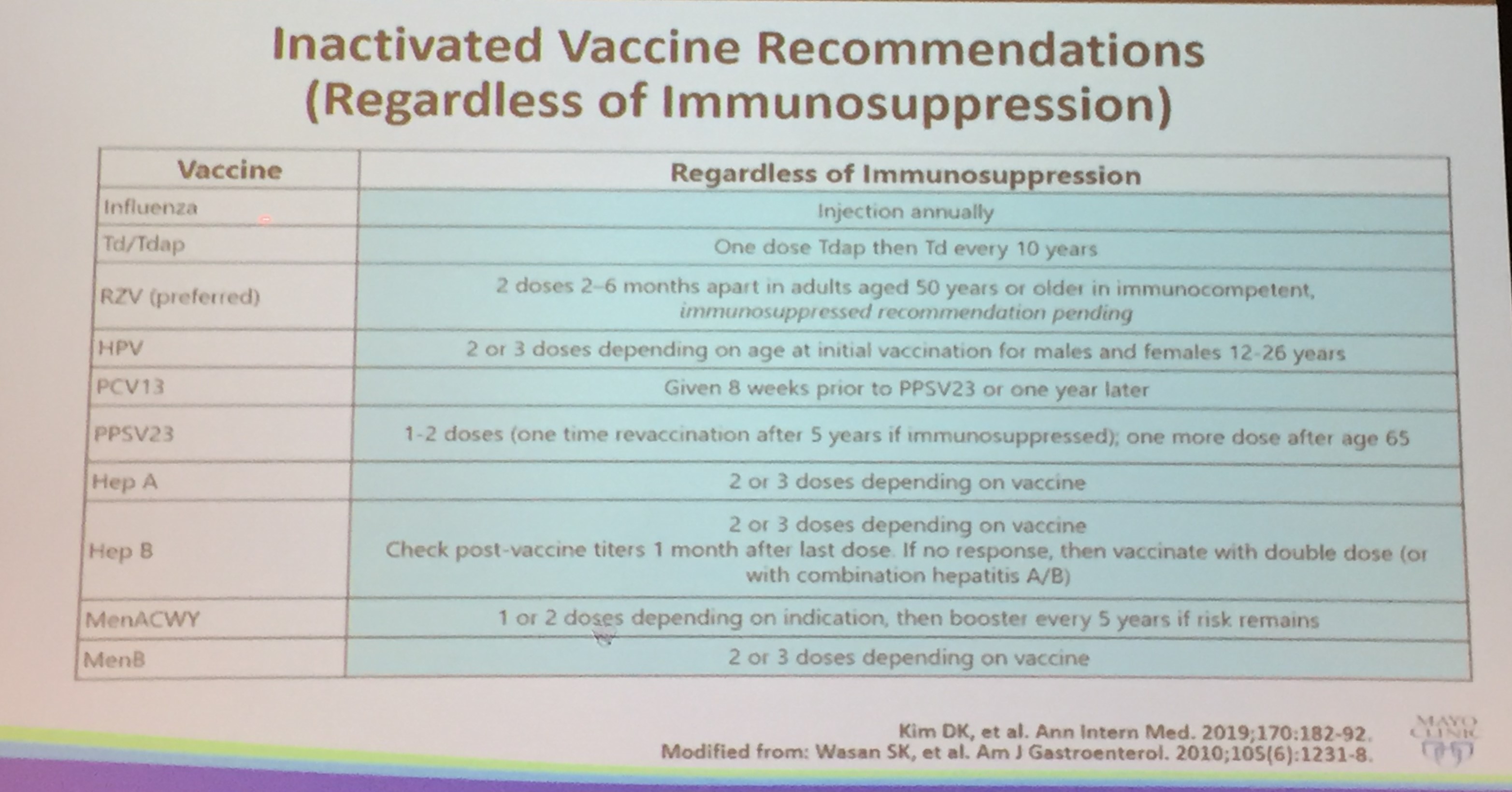
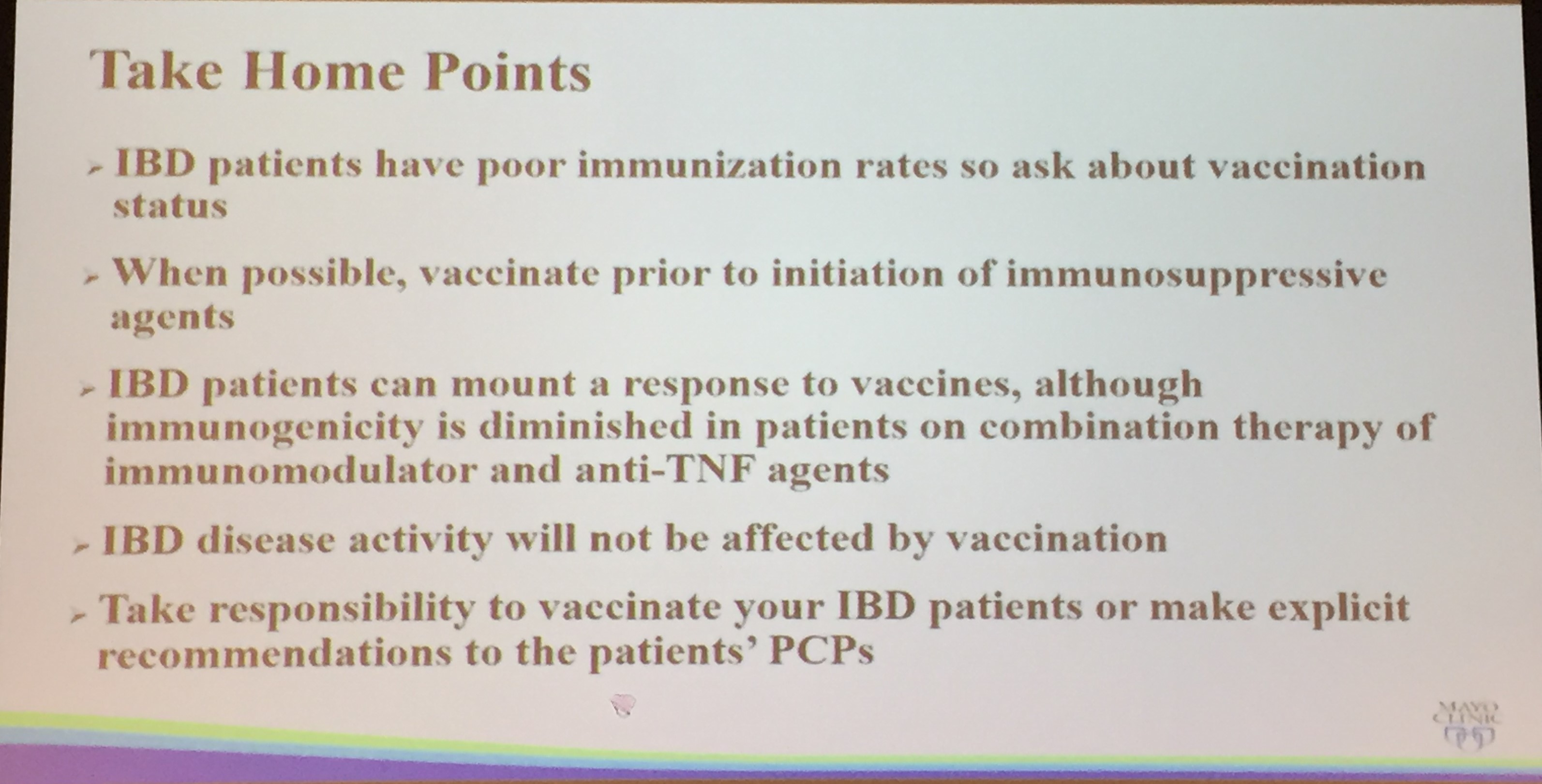
- Good Practice: Update Vaccinations in IBD population
- Recent concerns include measles outbreak, and frequent occurrence of Herpes zoster
- No evidence that vaccination exacerbates IBD
- New Hepatitis B Recombination Vaccine (Heplisa-B) -2 doses given over one month (for patients older than 18 years. Seroprotective anti-HBs after two doses: 95.4%
- Shingrix -new recombinant Zoster vaccine. Overall efficacy 97.2%. Frequent adverse reactions
- Women with IBD should undergo annual cervical cancer screening
- IBD patients should be seen by dermatology
- Consider depression screening in IBD patients
- Counsel patients to quit smoking
- Consider bone density screening in at risk patients
One audience member (Jeff Lewis, MD) pointed out that more attention needs to be paid to depression and anxiety which are much more common and more frequently health-threatening than issues like vaccination.
Related blog posts:
- Vaccination and Inflammatory Bowel Disease for Adults with IBD
- Immunization Recommendations from CDC 2013 | gutsandgrowth
- Because It Doesn’t Just Happen to Other People
- Protecting the Most Vulnerable
- Why Rich Kids Get Measles More Often in the U.S.
- The Paradox of Vaccine Resistance
Disclaimer: These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.