TA Fick et al. J Pediatr 2021; 239: 206-211. Trisomy 18 Trends over the Last 20 Years
Methods: A retrospective analysis using the Kids’ Inpatient Database from 1997 to 2016 (10,151 admissions) was performed for trisomy 18.
Key Findings:
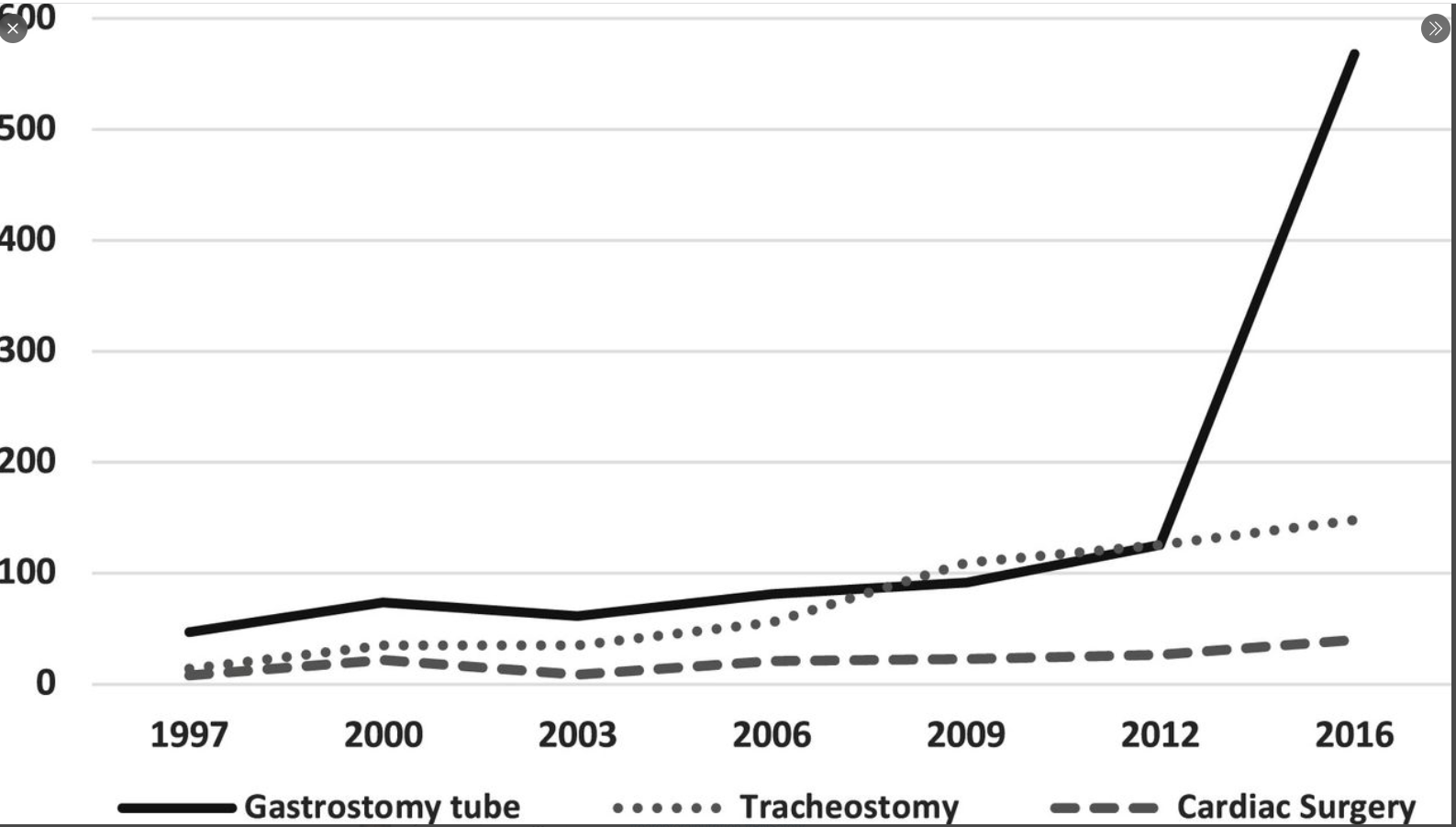
- Gastrostomy tube placement increased 12-fold during the study period, tracheostomy increased 11-fold, and cardiac intervention increased 5-fold
- The overall mortality rate (based on inpatient data) decreased in those with trisomy 18 from 32% in 1997 to 21% in 2016
- Limitations: their data are limited to only hospitalized children and do not include all patients with trisomy 18 or capture population incidence
My take: This study documents a change in the approach to treating children with Trisomy 18. Compared to 20 years ago, these children are being offered more medical/surgical treatments rather than only palliative interventions.