M-F Yuen et al. NEJM 2022; 387; 1957-1968. Efficacy and Safety of Bepirovirsen in Chronic Hepatitis B Infection
This study is nicely summarized in a “quick take” video and also reviewed in an accompanying editorial by J Hoofnagle (pages: 1996-1998).
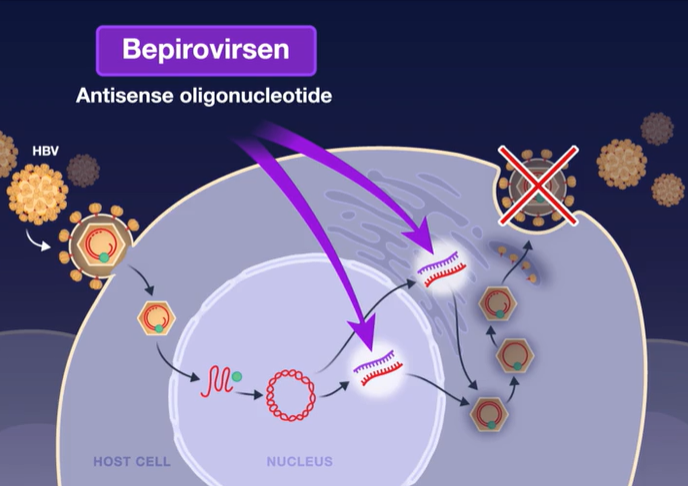
In this phase 2b, randomized, investigator-unblinded trial involving 457 participants with chronic HBV infection (1/2 receiving nucleotide analogue (NA) therapy), the authors evaluated bepirovirsen is an antisense oligonucleotide that targets all hepatitis B virus (HBV) messenger RNAs and acts to decrease levels of viral proteins.
Background: HBV infection affects 4% of worldwide population and has a prevalence of 0.3% in the U.S. Worldwide, HBV causes more than 1/2 million deaths each year.
Key finding:
Mechanism of Action: Bepirovirsen is an antisense oligonucleotide that targets all hepatitis B virus (HBV) messenger RNAs and acts to decrease levels of viral proteins.
Current therapies (like entecavir and tenofovir) are able to suppress viral replication but have low rates of clearance of HBsAg and most often HBV relapses when medications are stopped. This is due to covalently closed circular DNA which can persist in hepatocytes despite these medications.
In Dr. Hoofnagle’s editorial, he notes that bepirovirsen is one of several RNA-based HBV therapies that are being pursued. There are also “the more malleable small interfering RNA molecules (“-sirans”) are currently in early-phase clinical trials.”
My take: While these studies point to new therapies for those afflicted with HBV infection, the best strategy for reducing HBV mortality and morbidity still relies of wide-scale use of the highly effective HBV vaccine.
In this prospective cohort study with 1124 ERCPs (n=857 patients), 92% were performed in 15 centers by a pediatric gastroenterologist. Key findings:
Common indications included choledocholithiasis (41%), improved drainage for chronic pancreatitis (14%), stricture (17%), plan for sphincterotomy (5%) and bile leak (3%)
Procedures were technically successful in 90.5%
Only 26 cases (2.3%) were completed in infants (<1 yr) and 35 cases (3.1%) in 1-3 yrs. In these age groups, technical success was much lower: 80% (all children 3 yrs of age or less). Similarly, technical success was 76% in those <10 Kg.
ASGE difficulty grades 1 & 2 had success rates of 94% compared to 86% for grades 3 & 4. (ASGE classification adds one level in those 3 years of age or younger). ASGE grade 1, 2, 3 & 4 accounted for 13%, 47%, 34%, and 5% respectively.
Adverse effects were reported in 9.5%, though most were mild. Three perforations and 5 bouts of cholangitis were reported; however, there were no deaths or serious morbidity reported.
Post-ERCP pancreatitis (PEP) prophylaxis was associated with a decreased odds of PEP (OR 2.1, P=<0.01); among specific PEP prophylaxis, only rectal indomethacin neared statistical significance (P=0.07)
My take: Well-trained pediatric gastroenterologists are capable of doing high-quality ERCPs. In very young children, technical success is more difficult and probably requires the highest skillset.
In this case report, the authors describe a 16 yo male with ulcerative colitis who on postoperative day 4 after colectomy developed an early onset of non-infectious enteritis. Treatment included corticosteroids “without significant improvement over 2 weeks. As his corticosteroid dose was tapered by 5 mg/day each week, ostomy output decreased, and abdominal pain and distension improved.” He continued to improve without further interventions. “6 weeks postoperatively, repeat upper endoscopy and ileoscopy demonstrated resolution of his duodenitis and ileitis grossly.”
“This is the first published case of a pediatric patient with PCE [postcolectomy enteritis], an entity previously only described in adults. PCE may be difficult to diagnose; in patients initially diagnosed with UC who develop small bowel inflammation following colectomy, the concern is often misdiagnosed Crohn’s disease.” The authors note that the “presentation is differentiated from Crohn’s disease based on timing [days to months after surgery], histology and diffuse pattern of mucosal involvement (3).”
My take: Rare cases PCE (a self-limited enteritis) occur and can be difficult to distinguish from Crohn’s disease. With PCE, if findings improve, this would suggest PCE whereas if symptoms persist, then this would suggest Crohn’s disease.
This case reminds me of the swimming test for a witch. Sinking to the bottom indicated that the accused was innocent while floating indicated a guilty verdict. Which is to say that we don’t have a great test to tell if someone has PCE at presentation.
(A) Initial ileoscopy image—diffuse inflammation characterized by erythema, exudate, and friability. (B) Initial ileal histopathology—severe active ileitis, erosion, and focal crypt irregularity (magnification 100×).
Repeat ileoscopy image– (C) normal mucosa. (D) Repeat ileal histopathology—nonspecific changes including patchy lamina propria lymphoplasma cell infiltrate, eosinophilia, and spotty glandular and intraepithelial lymphocytosis (magnification 100×).
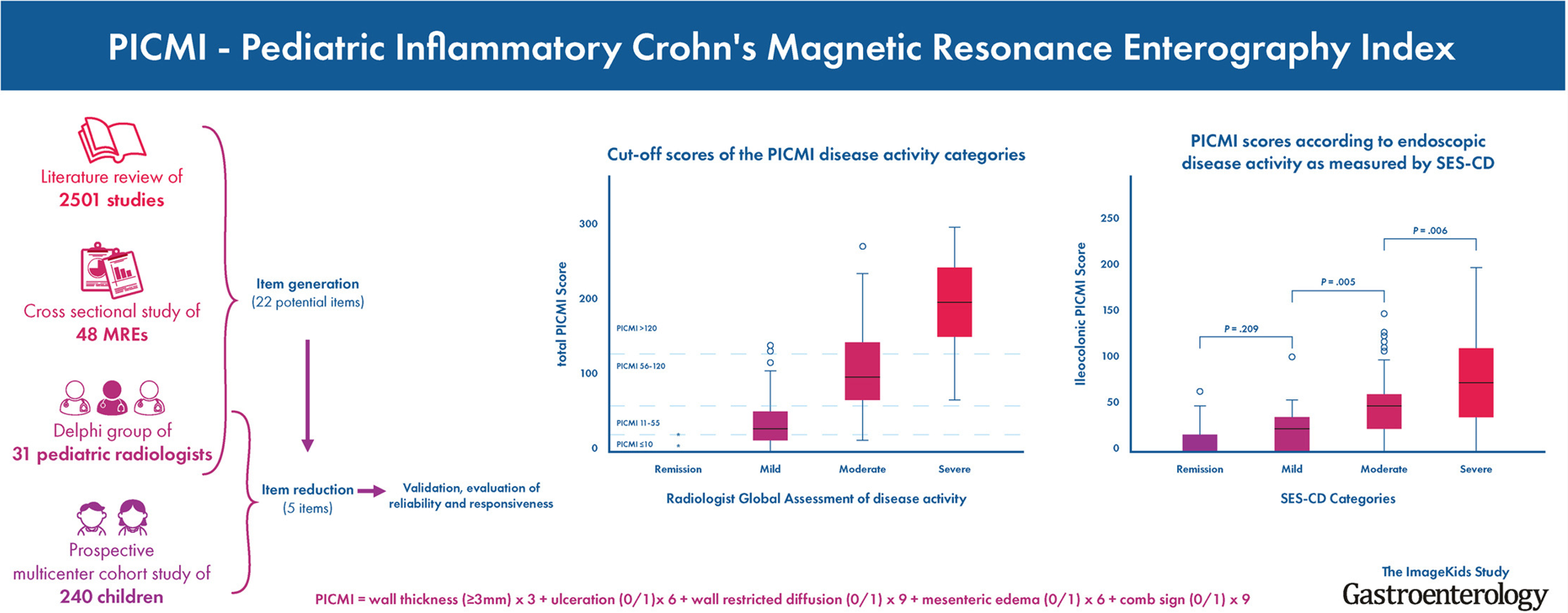
In the validation cohort of 81 MREs, the weighted global PICMI correlated well with the radiologist global assessment (r = 0.85; P < .001) and with the simple endoscopic score in a subsample with ileocolonic disease (r = 0.63; P < .001).
Interobserver and test-retest reliability were high (interclass correlation coefficients, 0.84 and 0.81, respectively; both P < .001)
Transmural healing was defined as PICMI ≤10 and response as a change of >20 points with excellent discriminative validity (area under the receiver operating characteristic curve = 0.96
My take: This study identifies a specific MRI index (PICMI) that is reliable for assessing the entire bowel in pediatric CD and does not require intravenous gadolinium or rectal enema. By using a standardized tool, similar to SEMA-CD for ileocolonoscopy, this will improve the usefulness of MREs.
Also noted: Link: Clinical support tool (sponsored by AGA) that provides individualized information on 2nd line therapy effectiveness (ustekinumab and vedolizumab) with regard to probability of achieving clinical remission, how quick to expect a response, and whether therapeutic drug monitoring is needed.
“Scientists were arguing about the causes of obesity, which affects more than 40 percent of U.S. adults and costs the health system about $173 billion each year. At the meeting’s closing session, John Speakman, a biologist, offered this conclusion on the subject: “There’s no consensus whatsoever about what the cause of it is. That’s not to say the researchers disagreed on everything. The three-day meeting was infused with an implicit understanding of what obesity is not: a personal failing.”
“No scientist spoke of any of the supposed fixes that fill diet books and store shelves, with the exception of the carbohydrate discussion. There wasn’t serious dialogue about cleanses, diet apps or intermittent fasting. No one suggested that supplements could help people lose weight or that metabolisms need boosting. The sole presenter on the gut microbiome argued that the human trials in obesity to date have mostly disappointed.”
“Researchers have repeatedly found fat shaming promotes weight gain and harms. At least some of obesity’s negative health consequences are thought to be driven by stigma and discrimination, which results in poorer health care. “
In the Practical Gastroenterology article, the article stresses that being overweight does not in itself confer bad health outcomes. “There is an abundance of epidemiological research showing that “obesity” is associated with longer survival with diabetes, cancer, and cardiovascular diseases than thinner people with the same diagnoses….The main assumption made in weight-centric healthcare that contributes to and perpetuates weight bias is that higher weight is synonymous with poorer health. While much research exists that correlates fatness with disease states, causation cannot be assumed. Often, these studies neglect to control for factors such as fitness level, activity, nutrient intake, weight cycling, socioeconomic status, and experienced or internalized weight bias…In all BMI categories, sedentary behavior was linked with mortality.”
Other key points:
“Weight cycling increases inflammation, and inflammation increases the risk of many diseases”
Moving away from using weight as a determinant of health and instead focusing on health behaviors “to achieve health rather than weight loss” may be a better model.
My take: In children and adults, these articles suggest that the best current approach is to focus on health behaviors (consuming healthy foods, and increasing activity) rather than weight and stop thinking of obesity as a personal failure.
In this case report, a 38 yo was incidentally discovered to have a purple liver while undergoing surgery for cholelithiasis. A diagnosis of Dubin-Johnson syndrome was made. It “is a benign autosomal-recessive liver disease with clinical manifestations of chronic or intermittent conjugated hyperbilirubinemia. It is caused by mutations in the ABCC2 gene leading to MRP2 [multidrug resistance-associated protein 2] dysfunction or deletion.”
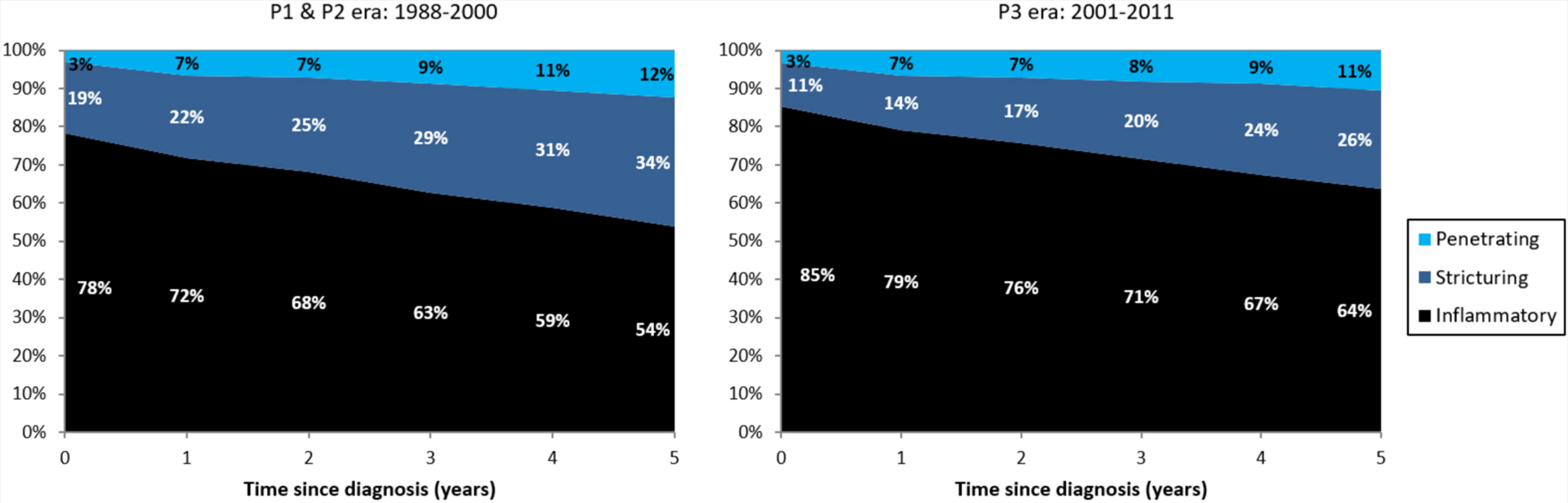
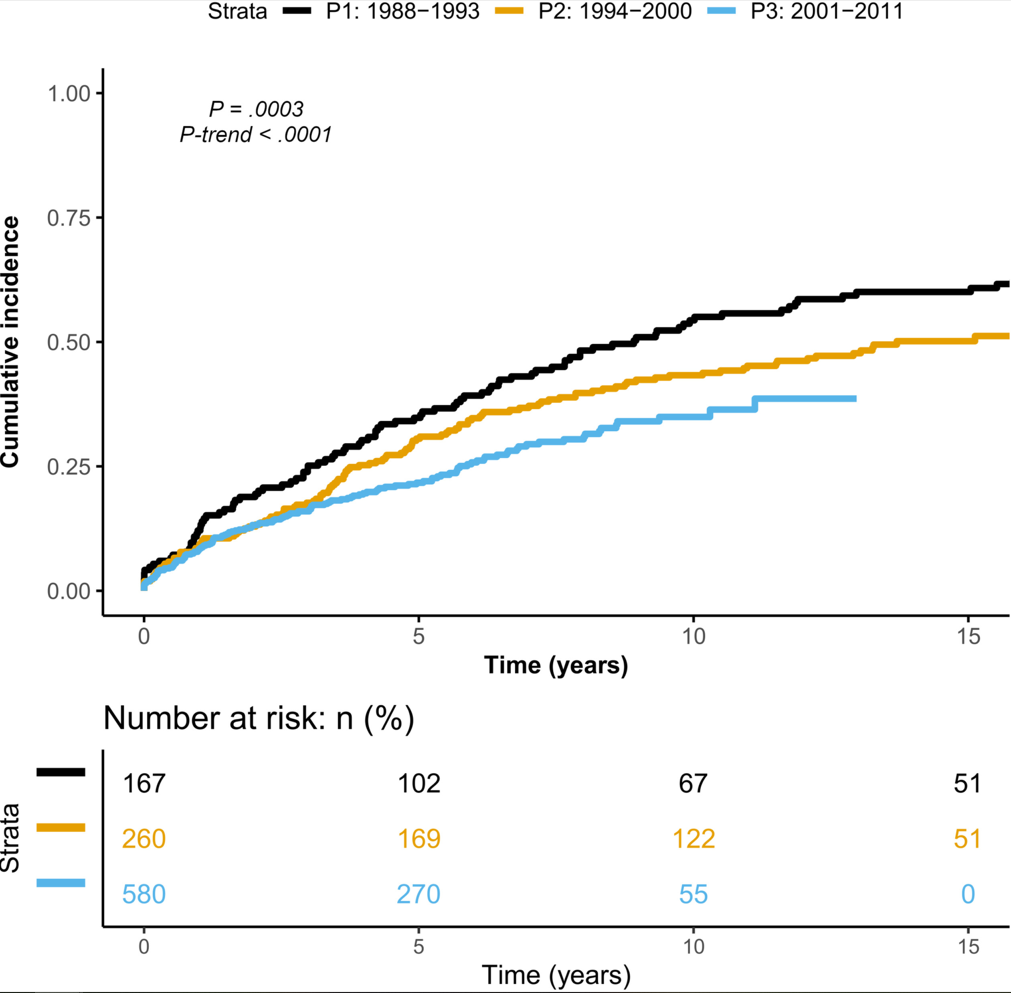
This retrospective study dating back to 1988 examined 1007 patients diagnosed with CD who were followed up for a median duration of 8.8 years.
Key findings:
The risk for intestinal resection at 5 years decreased significantly over time (P1, 35%; P2, 31%; and P3, 22%; P = .0003. This decrease in resections coincided with increased use of immunosuppressive (IS) and anti-TNF therapy: IS and anti-TNF exposure rate at 5 years increased from 33.9% (in P1) to 76.5% (in P3) and from 0% (in P1) to 50.5% (in P3).
The risk for progression from inflammatory to stricturing behavior decreased significantly over time (P1, 27%; P2, 28%; and P3, 20%)
LE Targownik et al. Clin Gastroenterol Hepatol 2022; 20: 2607-2618. Earlier Anti-TNF Initiation Leads to Long-term Lower Health Care Utilization in Crohn’s Disease but Not in Ulcerative Colitis
Methods: The authors “used health administrative data from Manitoba, Canada to identify all persons with a new diagnosis of inflammatory bowel disease (IBD) between 2001 and 2018 who received tumor necrosis factor antagonists (anti-TNF) therapy and had at least 1 year of post anti-TNF initiation follow-up.”
Key findings:
Among 742 persons with CD, early anti-TNF initiators had fewer IBD-specific and overall hospitalizations over the 5 years following the start of therapy
Incidence of resective surgery was also lower in earlier anti-TNF initiators with CD if the first year following initiation was excluded from the analysis.
In 318 cases of UC, there was no impact of the timing of anti-TNF therapy on the rates of hospitalization and surgery.
My take: These two studies show that use of biologic therapy is associated with better outcomes in Crohn’s disease including fewer intestinal resections and fewer hospitalizations. It appears that earlier use may alter the natural history in part by reducing the likelihood of stricturing disease. Interestingly, the RISK study showed a reduction in penetrating disease with early use of biologics but not a reduction in stricturing disease (Related blog post: CCFA: Updates in Inflammatory Bowel Disease 2017 (part 3))
This article has 91 authors! Using Delphi surveys, the authors recommend the following:
“EGID” was the preferred umbrella term for disorders of gastrointestinal (GI) tract eosinophilic inflammation in the absence of secondary causes
Involved GI tract segments will be named specifically and use an “Eo” abbreviation convention: eosinophilic gastritis (now abbreviated EoG), eosinophilic enteritis (EoN), and eosinophilic colitis (EoC)
For EoN, “it is desirable, but not required, to name specific locations of small bowel involvement, if these are known…The abbreviation for eosinophilic duodenitis should be “EoD”… for eosinophilic jejunitis should be “EoJ”….eosinophilic ileitis should be “EoI”
The term “eosinophilic gastroenteritis” is no longer preferred as the overall name (but can be used to indicate involvement of both the stomach and small bowel)
When >2 GI tract areas are involved, the name should reflect all of the involved areas