I am happy to say that this is the last nightcall that I will have this year!
Today, I’ve compiled some of my favorite posts from the past year. I started this blog a little more than 10 years ago. I am grateful for the encouragement/suggestions from many people to help make this blog better. Also, I want to wish everyone a Happy New Year.
Methods: A longitudinal cohort study was conducted among healthy children 0-10 years of age participating in The Applied Research Group for Kids study between June 2008 and August 2019 in Toronto, Canada.
Key findings:
Of 8943 children included, the mean (SD) age of infant cereal introduction was 5.7 (2.1) months
Children who were introduced to infant cereal at 4 vs 6 months had 0.17 greater body mass index z score (95% CI 0.06-0.28; P = .002) and greater odds of obesity (OR 1.82; 95% CI 1.18-2.80; P = .006) at 10 years of age.
Earlier cereal introduction was associated with a less-favorable eating behavior score at 18 months to 5 years of age (0.18 units higher; 95% CI 0.07-0.29; P = .001).
Limitation: This study did not randomize children into early vs late cereal introduction; thus, there may be unidentified confounders that contribute to weight gain in children offered cereal at a younger age.
My take: This study indicates that introduction of cereal at 6 months of age, rather than 4 months of age, may be beneficial in limiting excess weight gain.
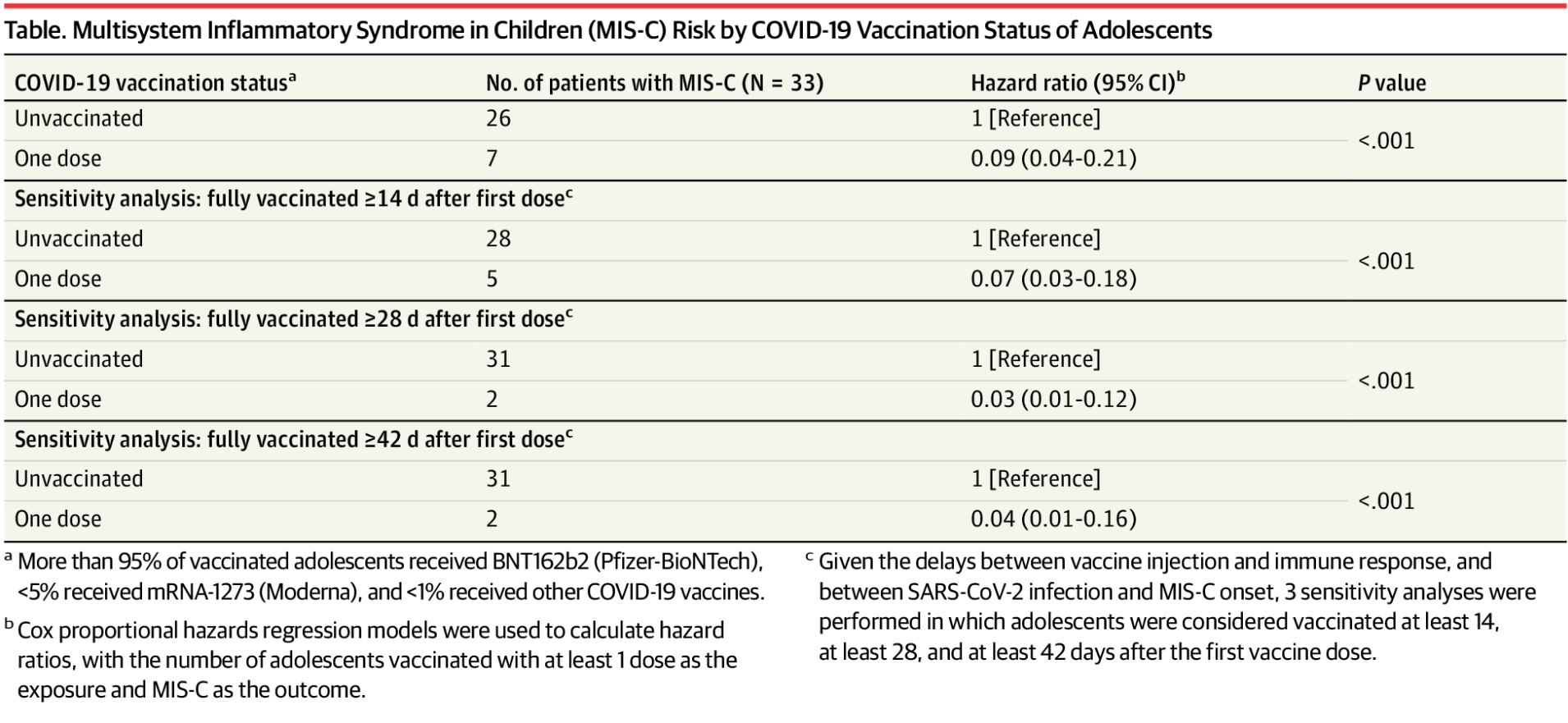
From September 1, 2021, to October 31, 2021, a total of 107 childrenwith MIS-C were hospitalized in France…33 (31%) were adolescents eligible for vaccination
Among those with MIS-C, 0 had been fully vaccinated, 7 had received 1 dose with a median (IQR) time between vaccine injection and MIS-C onset of 25 (17-37) days, and 26 had not been vaccinated. The HR for MIS-C was 0.09 (95% CI, 0.04-0.21; P < .001) after the first vaccine dose compared with unvaccinated adolescent. Because there were no MIS-C cases in those who were vaccinated, an HR cannot be calculated in this group.
The study had limitations, including the low number of patients, use of national data to calculate HR without considering regional variations, and inability to control for individual risks of MIS-C, such as sex, race and ethnicity, and comorbidities
My take: This study indicates that COCID-19 vaccination likely results in a marked decrease in the risk of MISC-C. This finding provides an additional reason favoring vaccination in adolescents in terms of risk-benefit calculation for immunization.
Background: “The OTSC (Ovesco Endoscopy AG, Tubingen, Germany) is a flexible, biocompatible nitinol clip that has multiple teeth oriented like a bear-claw, deployed via a band ligation–type mechanism. It is substantially larger than standard 2-tined hemostatic clips, allowing 1 OTSC to entrap far more tissue in a full-thickness bite. This unique design and its marked compressive force are purportedly capable of clinching even large vessels in excavated/fibrotic/near-perforating ulcers that are in complex anatomic locations. The bear-claw design allows not only for better tissue capture, but also adds higher site stability.”
53 patients (from cohort of 346) met the following criteria:
(2) laboratory evidence of high-volume blood loss (hemoglobin level ≤9 g/dL, or hemoglobin level decrease of ≥2 g/dL from baseline at admission)
(3) need for packed red blood cell (PRBC) transfusion (received 1 or more units PRBC)
In this study, the authors compared OTSC to standard treatment (hemoclips or multipolar electrocoagulation).
Key findings from study:
Immediate hemostasis was achieved in all patients.
The cumulative 30-day rebleeding rate was significantly lower in the OTSC group than in the standard group (4% vs 28.6%; P = .017), with most patients experiencing rebleeding within 4 days. All rebleeds occurred in patients with major stigmata of recent hemorrhage (SRH) and none with lesser SRH. SRH included active spurting bleeding, visible vessel, or clot.
The number of PRBC units transfused was also significantly higher in the standard versus OTSC group (0.68 vs 0.04 units; P = .03).
Severe complications were less frequent in OTSC (0 % vs. 14.3%)
Limitations: despite randomization, within the groups, major SRH with active arterial bleeding (Forrest 1A) was observed in a higher number of patients in the standard group (7 standard vs 2 OTSC) and study was conducted in specialized quaternary medical center with high expertise. In addition, “whether it should be used in all cases of NVUGIB or be reserved for patients with a high-risk for adverse outcome lesions12 remains to be addressed.”
The editorial reviewed two other studies supporting the superiority of OTSC: FLETRock and STING.
My take (from editorial): The data about improved outcomes in the OTSC compared with standard therapy are compelling. Training in OTSC application will be needed for more widespread adoption.
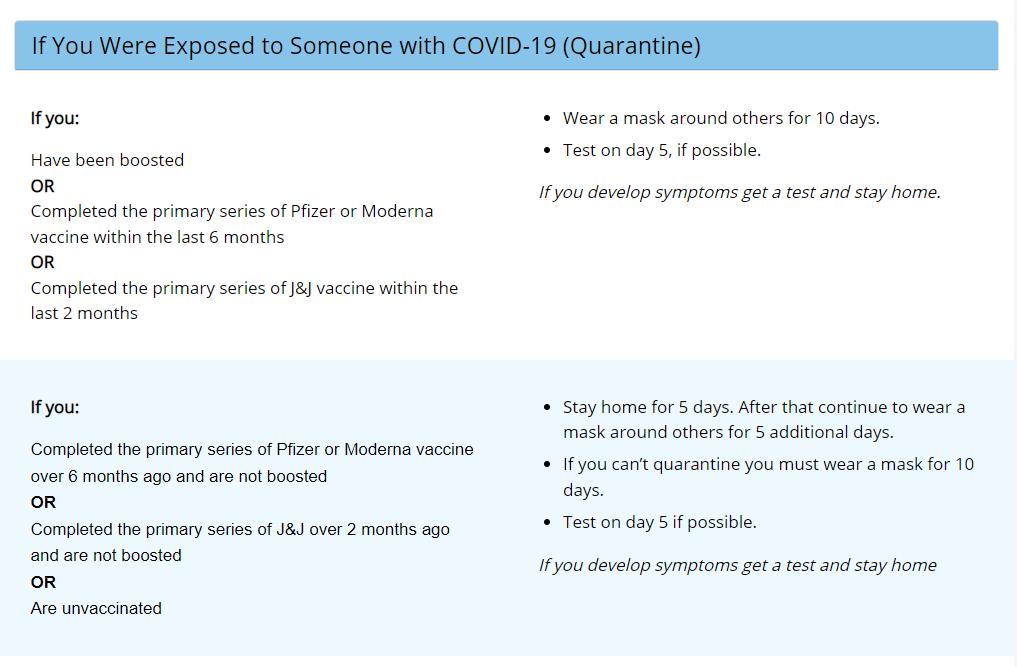
Healthcare workers with COVID-19 who are asymptomatic can return to work after 7 days with a negative test, and that isolation time can be cut further if there are staffing shortages.
Healthcare workers who have received all recommended COVID-19 vaccine doses, including a booster, do not need to quarantine at home following high-risk exposures.
This retrospective case-control study identified 93 patients out of 1032 with chronic HCV infection who had a relapse of detectable infection following treatment. Key findings:
12 patients (13%) spontaneously cleared HCV within 6 months after the documented relapse without additional therapy
The spontaneous clearers had low levels of HCV RNA (<4 log IU/mL in 11 of 12) and normal levels of alanine aminotransferase at the time of relapse. Low level RNA was identified in only 1 persistent relapser
There was no significant difference between the spontaneous clearance group and the SVR12 group in magnitude and breadth of HCV-specific T cell responses
The authors note that one limitation of the study was a false positive PCR assay –though this does not negate their message that retesting is important before retreatment
The relatively high relapse rate (9%) in this cohort is likely related to the use of first-generation DAA therapy
The timing of retesting in the 12 with spontaneous clearance was variable. 7 who had repeat testing at 3 months were all negative.
My take: In those with a low level virological relapse after DAA therapy for HCV, it is a good idea to repeat testing before consideration of further treatment.
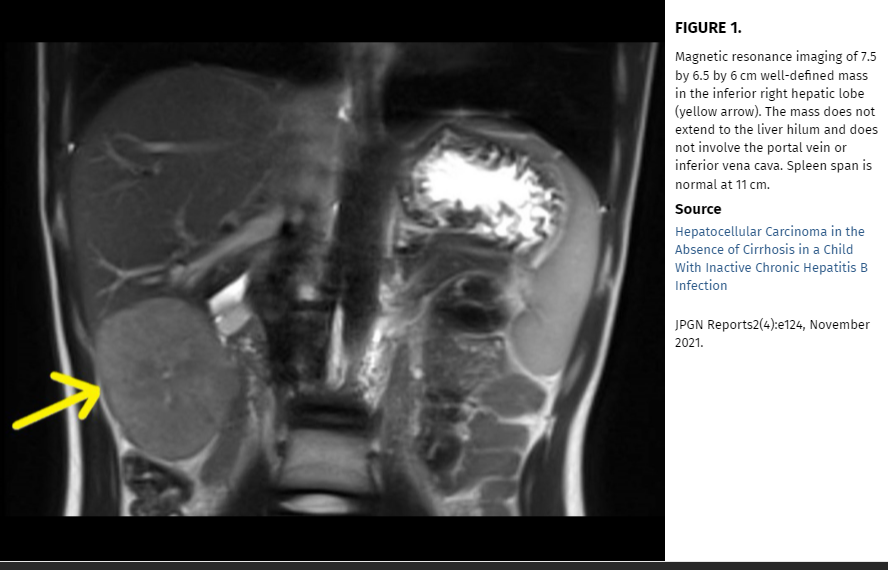
In this case study, the authors “describe an unusual case of a child with chronic hepatitis B infection who developed HCC in the absence of active hepatitis or cirrhosis.” Based on their case report, they advocate for “regular HCC surveillance for all children with chronic hepatitis B, regardless of presence or absence of hepatitis or cirrhosis.”
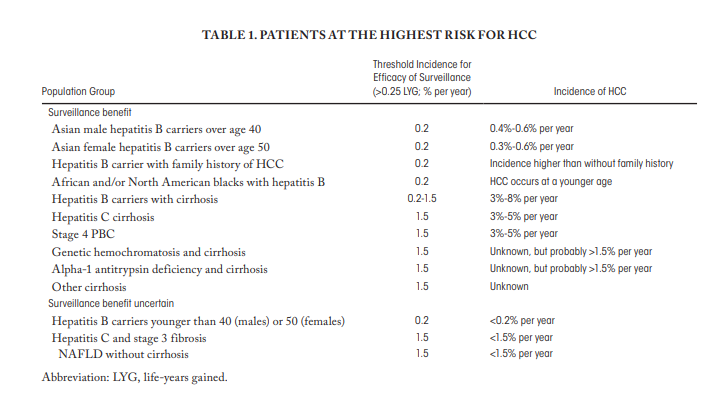
However, the authors suggestions to expand surveillance to all children with hepatitis B is NOT aligned with current expert opinion (by most experts). This potential recommendation deserves (deserved) more commentary in their discussion. The AASLD recommends offering surveillance when the risk of HCC is at least 1.5% per year and the incidence is greater than 0.2% per year, which includes patients with cirrhosis and some non-cirrhotic hepatitis B carriers [7]. In a study from Taiwan (blog post: HBV Vaccination Prevents Cancer), the authors showed the beneficial effects of vaccination: HCC incidence per 105 person-years was 0.92 in the unvaccinated cohort and 0.23 in the vaccinated birth cohorts. This study also showed how rare HCC cases are in children; thus, showing benefit of vaccination was impressive.
My take: This case report is helpful in emphasizing the risk of HCC in patients with HBV, even in those without significant risk factors. However, at this time most experts do not recommend surveillance in those with a low risk of developing HCC.
HBV Vaccination Prevents Cancer In Taiwan: HCC incidence per 105 person-years was 0.92 in the unvaccinated cohort and 0.23 in the vaccinated birth cohorts.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
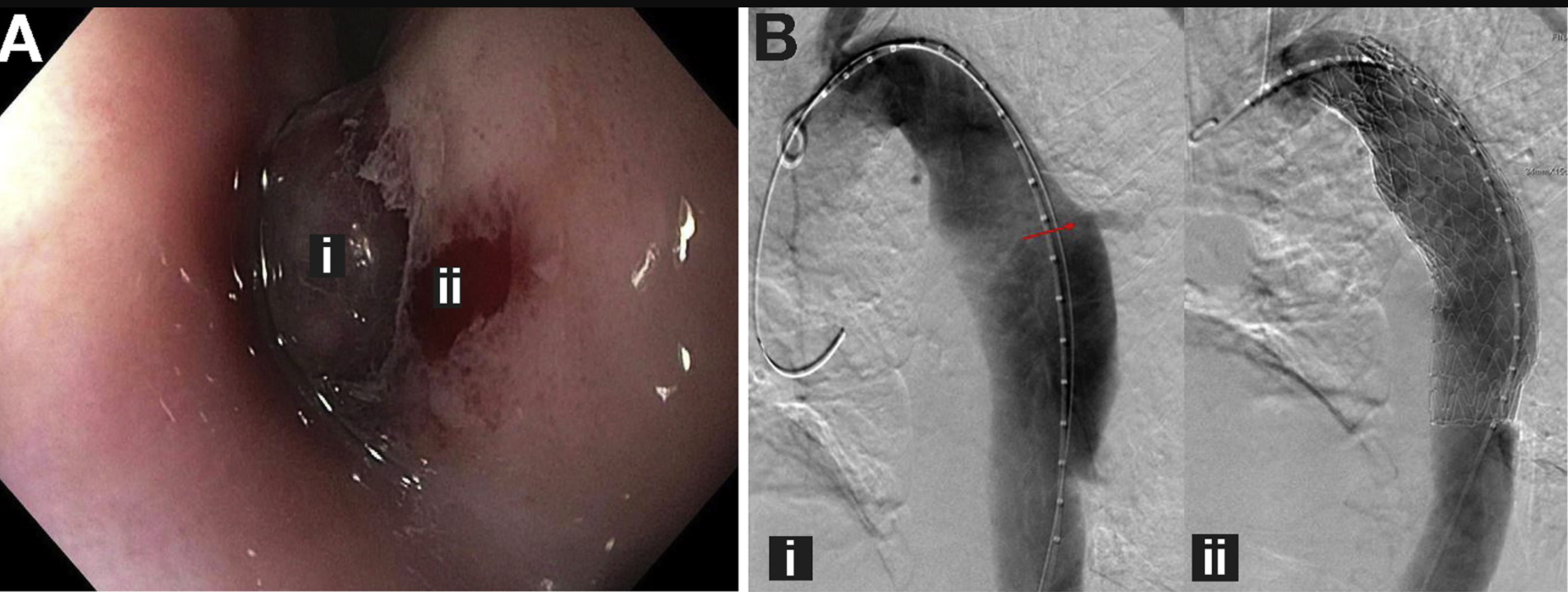
The authors recognized a “visible thoracic aorta eroding into the esophagus through a large transmural defect (FigureA) and a nonbleeding aortoesophageal fistula (FigureB) directly superior to the erosion in the middle third of the esophagus. This 76 year old patient had a known thoracic aortic aneurysm.
My take: This is an amazing case report because the patient survived. It is very easy to imagine the circumstance of massive exsanguination. In all patients with known cardiac repair and disease, it is important to consider the possibility of an major vessel fistula into the esophagus in those presenting with significant hematemesis and to consider how this could be managed.
In this prospective study of 50 patients with IBS (ROME III, all subtypes), with and without serologic reactivity to gluten (antigliadin IgG and IgA), and 25 healthy subjects (controls) were studied before and after 4 weeks of a GFD. Celiac disease (CD) was ruled out in patients and controls by negative tissue transglutaminase (tTG) IgA antibody and deamidated gliadin IgA or IgG antibodies and by the absence of mucosal atrophy in a duodenal biopsy specimen (Marsh 0 or 1). At least 4 and 2 biopsy specimens were obtained from the second and the first part of the duodenum, respectively.
Key findings:
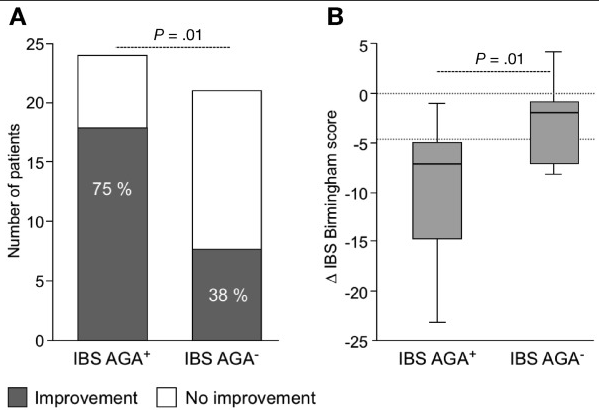
Compared with baseline, IBS symptoms improved in 18 of 24 patients (75%) with antigliadin IgG and IgA and in 8 of 21 patients (38%) without the antibodies
(A) Improvement in IBS symptoms (>4.5 points in the total Birmingham score) in antigliadin antibody (AGA)+ and AGA– patients after GFD. (B) Change in IBS symptoms after a gluten-free diet (GFD) compared with baseline in AGA+ and AGA– patients.
“A key trigger for symptom generation in IBS is diet, with more than 80% reporting food-related symptoms…It seems that wheat is a key component for symptom generation in IBS, as demonstrated by a study in 920 patients by Carroccio et al,8 which identified wheat sensitivity in 30% of patients”
The authors note that the Pinto-Sanchez population had a higher-than-expected rate of AGA positivity of 50% when previous studies have found rates of 7-18%.
My take: This prospective study indicates that a GFD is associated with clinical improvement in a significant number of individuals with IBS (with and without antigliadin antibodies) who did not report any gluten sensitivity or were not on a gluten-restricted diet before study entry. Based on a number of other studies, however, it seems that a low FODMAPs diet is likely to have a higher efficacy for patients with IBS.