C Podkul 8/14/23 Propublica (open access!): The Hidden Fee Costing Doctors Millions Every Year
An excerpt:
A powerful lobbyist convinced a federal agency that doctors can be forced to pay fees on money that health insurers owe them. Big companies rake in profits while doctors are saddled with yet another cost in a burdensome health care system…
In August 2017, a federal agency with sweeping powers over the health care industry posted a notice informing insurance companies that they weren’t allowed to charge physicians a fee when the companies paid the doctors for their work. Six months later, that statement disappeared without explanation.
The vanishing notice was the result of a behind-the-scenes campaign by the insurance industry and its middlemen that has largely escaped public notice — but that has had massive financial consequences that have rippled through the health care universe. The insurers’ invisible victory has tightened the financial vise on doctors and hospitals, nurtured a thriving industry of middlemen and allowed health insurers to do something no other industry does: Take one last cut even as it pays its bills.
Insurers now routinely require doctors to kick back as much as 5% if they want to be paid electronically. Even when physicians ask to be paid by check, doctors say, insurers often resume the electronic payments — and the fees — against their wishes...
Dr. Alex Shteynshlyuger, a urologist who runs his own clinic in New York City, made it his mission to take on both the insurers and the federal bureaucracy. He began filing voluminous public records requests with CMS.
My take: This article shows another layer of a broken health care system where the ‘frauds are legal.’
Related blog posts:
- “Health Insurance Is Broken” | gutsandgrowth
- Healthcare: “Where the Frauds Are Legal”
- No One Would Design U.S. Healthcare System This Way
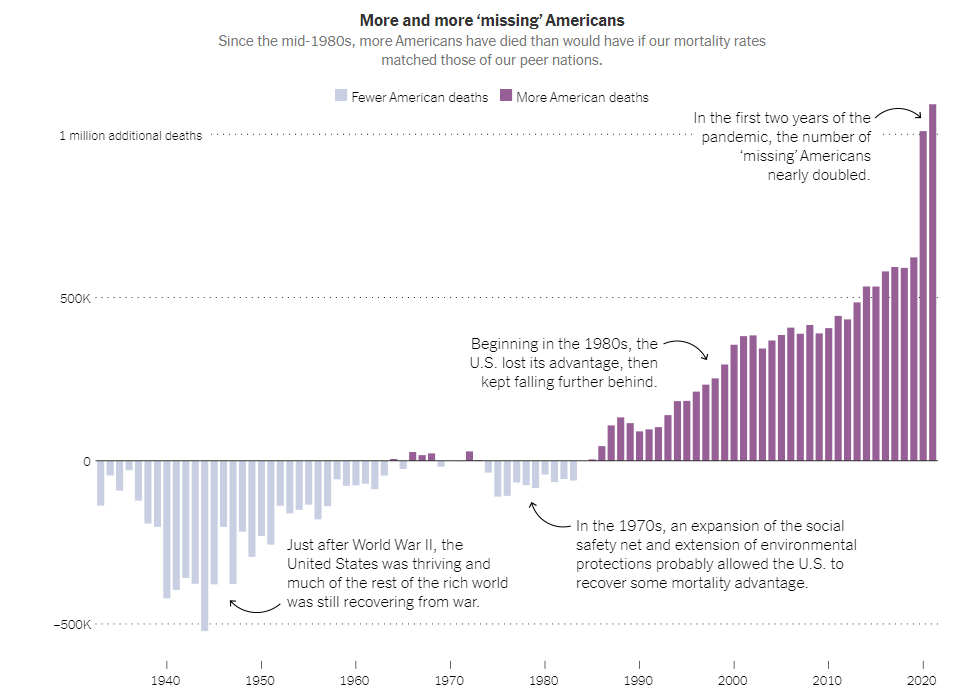
- NY Times: America can afford a world-class health system. Why don’t we have one?
- We are Last in Health Care Among High Income Countries