
Here is her speech at CCFA Torch Gala dinner (~3:30): Chelly Dykes CCFA Gala
Related blog post: Premier Physician: Chelly Dykes
Bernadette and I have worked together for more than 26 years -pretty soon she will have me trained.

Here is her speech at CCFA Torch Gala dinner (~3:30): Chelly Dykes CCFA Gala
Related blog post: Premier Physician: Chelly Dykes
Z Wang et al. Clin Gastroenterol Hepatol 2023; 3188-3190. Therapeutic Drug Monitoring Can Guide the Intravenous-to-Subcutaneous Switch of Infliximab and Vedolizumab: A Simulation Study
The authors performed population pharmacokinetic (popPK) simulations to determine optimal dosing recommendations.
Key points:
My take: It is still important to see how switching from IV to SC route affects clinical outcomes in real-world cohorts. This study, though, does provide a good starting point when trying to provide the right dose frequency to achieve good therapeutic troughs.
Related blog posts:

Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
Previous work has established Guselkumab, a IL-23p19 subunit antagonist for Crohn’s disease (Guselkumab: Expanding the GALAXI of Treatments for Crohn’s Disease).
Peyrin-Biroulet et al now provide data showing its efficacy for ulcerative colitis (UC): Gastroenterol 2023; 165: 1443-1457. Open access! Guselkumab in Patients With Moderately to Severely Active Ulcerative Colitis: QUASAR Phase 2b Induction Study
Background/Methods: The QUASAR Phase 2b Induction Study evaluated the efficacy and safety of guselkumab, an interleukin-23p19 subunit antagonist, in patients with moderately to severely active ulcerative colitis (UC) with prior inadequate response and/or intolerance to corticosteroids, immunosuppressants, and/or advanced therapy. In this double-blind, placebo-controlled, dose-ranging, induction study, adult patients (n=313), with median disease duration of 7.5 years, were randomized (1:1:1) to receive intravenous guselkumab 200 or 400 mg or placebo at weeks 0/4/8.
Key findings:
My take: This is an era with rapidly expanding medical treatments for inflammatory bowel disease; it should help reduce the problem of individuals who are refractory to available treatments.

GI & Hepatology News, November 2023: FDA OKs two new treatments for UC
An excerpt:
In October, the FDA approved etrasimod (Velsipity, Pfizer) for moderate to severe active UC in adults. Etrasimod, an oral sphingosine-1-phosphate (S1P) receptor, binds with high affinity to receptors 1, 4, and 5. It is the second agent in the S1P class approved for UC. The other agent, ozanimod (Zeposia, Bristol-Myers Squibb), which was approved for moderate to severe active UC in May 2021, is an S1P receptor modulator that is selective for the S1P1 and S1P5 receptors located on endothelial cells and oligodendrocytes, respectively.
Etrasimod’s approval was based on safety and efficacy data from two randomized, double-blind, placebo-controlled phase 3 trials ― ELEVATE UC 52 trial, and ELEVATE UC 12 trial. The Lancet published full results from the two trials on March 2. Both trials enrolled patients with UC who had previously failed or were intolerant of at least one conventional, biologic, or Janus kinase (JAK) inhibitor therapy.
In ELEVATE UC 52, clinical remission at 12 weeks occurred in 27% of patients taking etrasimod, vs 7% of patients taking a placebo (20% difference; P ˂.001). At week 52, remission rates were 32% with active treatment, vs. 7% with placebo (26% difference;
P ˂ .001).
In ELEVATE UC 12, clinical remission was achieved among 26% of patients who received etrasimod, vs 15.0% of patients who received placebo (11% difference; P < .05).
The approved recommended dose is 2 mg once daily. The most common side effects of etrasimod are headache, elevated values on liver tests, worsening of UC, SARS-CoV-2 infection, dizziness, pyrexia, arthralgia, abdominal pain, and nausea
Reference: WJ Sandborn et al. The Lancet 2023; DOI:https://doi.org/10.1016/S0140-6736(23)00061-2. Open Access! Etrasimod as induction and maintenance therapy for ulcerative colitis (ELEVATE): two randomised, double-blind, placebo-controlled, phase 3 studies
My take: It is not exactly clear where etrasimod or ozanimod should be positioned for ulcerative colitis therapy as several other drug classes have much higher response rates.
Related blog posts:

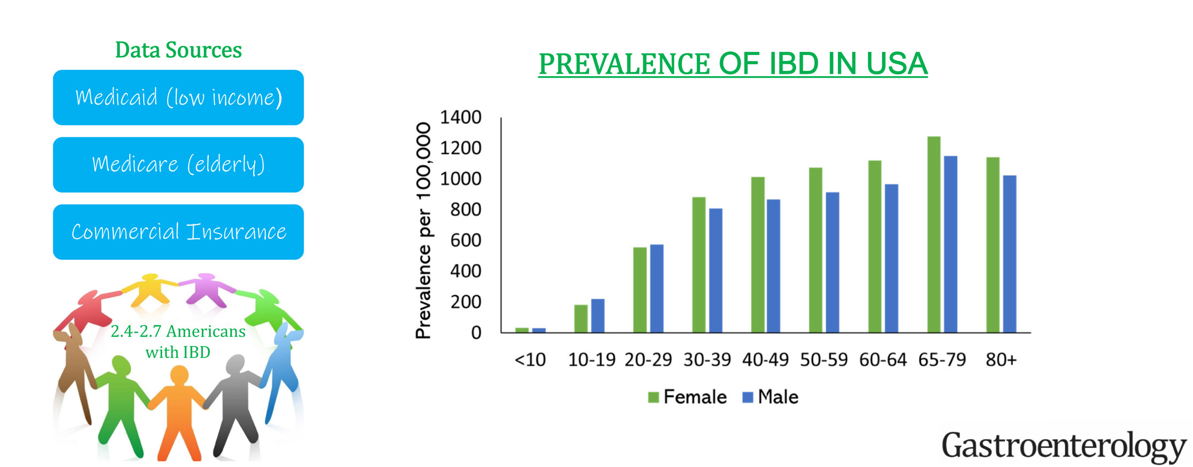
JD Lewis et al. Gastroenterology 2023 Nov;165(5):1197-1205.e2. doi: 10.1053/j.gastro.2023.07.003. Incidence, Prevalence, and Racial and Ethnic Distribution of Inflammatory Bowel Disease in the United States
This “INPUT” (INcidence, Prevalence, Treatment and OUTome in Patients with IBD) study used 4 different data sets to provide “the clearest depiction to date of IBD [epidemiology] in the U.S.
Key findings:
My take: The prevalence of IBD continues to increase and the U.S. has one of the highest rates in the world.
Related blog posts:
A Yu et al. Clin Gastroenterol Hepatol 2023; 21: 3115-3124. Open Access! Real-World Experience With Tofacitinib Dose De-Escalation in Patients With Moderate and Severe Ulcerative Colitis
On May 30, 2018, the US Food and Drug Administration (FDA) expanded the indication of tofacitinib (Xeljanz; Pfizer), an oral Janus kinase (JAK) inhibitor, for the treatment of adults with moderately to severely active ulcerative colitis. However, the optimal dosing remains unclear.
In this “real-world” study by Yu et al, a retrospective review of 162 patients was conducted (2012-2022). 52% continued 10 mg twice daily while 48% underwent dose de-escalation to 5 mg twice daily. The primary outcome was evidence of UC disease activity–related events: hospitalization/surgery, corticosteroid initiation, tofacitinib dose increase, or therapy switch.
Key findings:
Discussion Points:
My take (borrowed from authors): “Emphasis should be placed on clinical and endoscopic evidence of improvement before consideration of dose de-escalation to ensure the highest probability of treatment success.” This advice, though, may conflict with product labelling which states that “tofacitinib induction with 10 mg twice daily beyond 16 weeks is not recommended; in fact, it is recommended to stop after 16 weeks if adequate response has not been achieved.”
Related blog posts:

Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
V Solitano et al. Clin Gastroenterol Hepatol 2023; 21: 3019-3029. HLA-DQA1∗05 Genotype and Immunogenicity to Tumor Necrosis Factor-α Antagonists: A Systematic Review and Meta-analysis
Key findings:
My take:
Related blog posts:

The Good News:
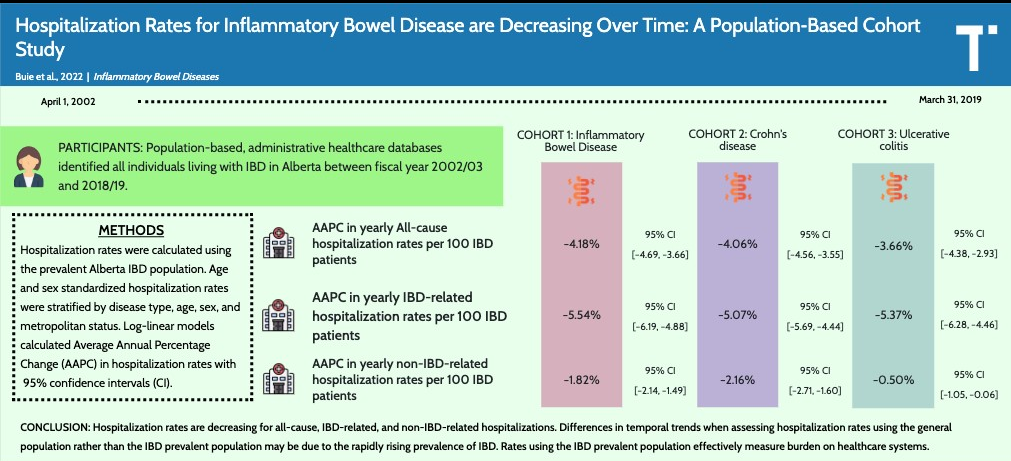
MJ Buie et al. Inflamm Bowel Dis 2023; 29: 1536-1545. Open Access! Hospitalization Rates for Inflammatory Bowel Disease Are Decreasing Over Time: A Population-based Cohort Study
This population-based administrative data cohort study provides annual IBD hospitalization rates in Alberta, Canada.
Key findings:
“The last 2 decades have seen the introduction of several advanced therapies with novel mechanisms of action.22 The introduction of these therapies has been accompanied by changes in management strategies that include earlier introduction of advanced therapies based on risk stratification, treat-to-target, and monitoring strategies.5,23–26 These advancements include risk stratification, allowing for earlier introduction of advanced therapies; proactive clinical management algorithms to monitor disease activity; and therapeutic drug monitoring allowing for continued concentration-based dosing.23–26The net effect of these medical advances shifted IBD management from the hospital to the outpatient setting.27“
The Bad News:
DK Choi et al. Inflamm Bowel Dis 2023; 29: 1658-1661. Delays in Therapy Associated With Current Prior Authorization Process for the Treatment of Inflammatory Bowel Disease
This retrospective study of 1693 prior authorizations (PAs) from 2020-2021. Key findings:
Median Days to Determination by Insurance Level:
My take: The PA process usually results in few denials (if pursued) but does result in significant delays in therapy. At the same time, these newer therapies have been associated with improvement in hospitalizations rates.
Related blog posts:
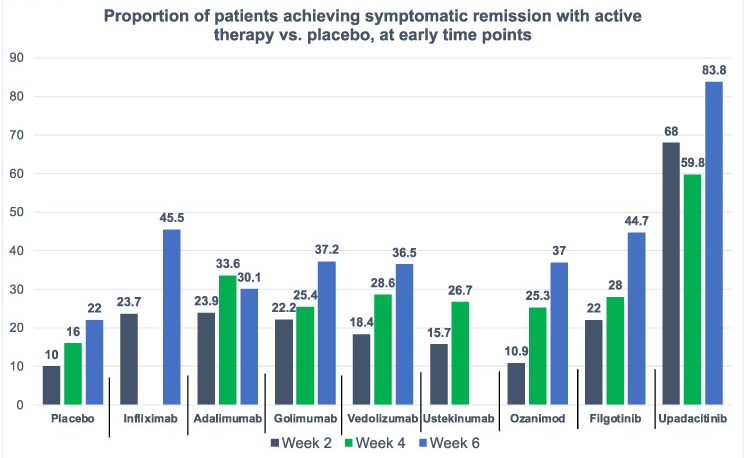
D Ahuja et al. Am J Gastroenterol 2023; Open Access! Comparative Speed of Early Symptomatic Remission With Advanced Therapies for Moderate-to-Severe Ulcerative Colitis: A Systematic Review and Network Meta-Analysis Thanks to Ben Gold for this article.
Key findings:
This study has a number of limitations including the following:
My take: This study indicates an impressive early symptomatic response to upadacitinib compared to other agents for ulcerative colitis.
Related blog posts:
FA Hanna et al. JPGN 2023; 77: 505-511. Thiopurines Maintenance Therapy in Children With Ulcerative Colitis: A Multicenter Retrospective Study
In this retrospective study with 133 children (2008-2019), typical dosing of thiopurines: azathioprine 2-2.5 mg/kg/day and 6-mercaptopurine 1.5 mg/kg/day. Patients with previous or concomitant treatment with 5-ASA were allowed in the study. 62% (n=83) of the cohort had pancolitis. Key Findings:
In their discussion, the authors make several points regarding efficacy and safety of thiopurines.
My take: In the U.S., it appears that thiopurine monotherapy, and even combination therapy, in pediatrics with IBD is used infrequently. Anti-TNF therapy with therapeutic drug monitoring is used routinely in patients if a 5-ASA is ineffective or not a good option. This article is a reminder that thiopurines are still a reasonable option. This would have been a good opportunity for a commentary in JPGN to add some context to this article regarding the role of these agents.
AGA guidelines for moderate-to-severe ulcerative colitis: “In adult outpatients with moderate to severe UC in remission, AGA makes no recommendation in favor of or against using biologic monotherapy or tofacitinib rather than thiopurine monotherapy for maintenance of remission.”
Related blog posts:


