Here are some notes and a few slides from NASPGHAN’s plenary session. There could be errors of transcription in my notes.
Benjamin Gold, NASPGHAN president and part of our GI group, GI Care For Kids, welcomed everyone to the meeting.
Link to NASPGHAN_Annual_Meeting_Program 2019
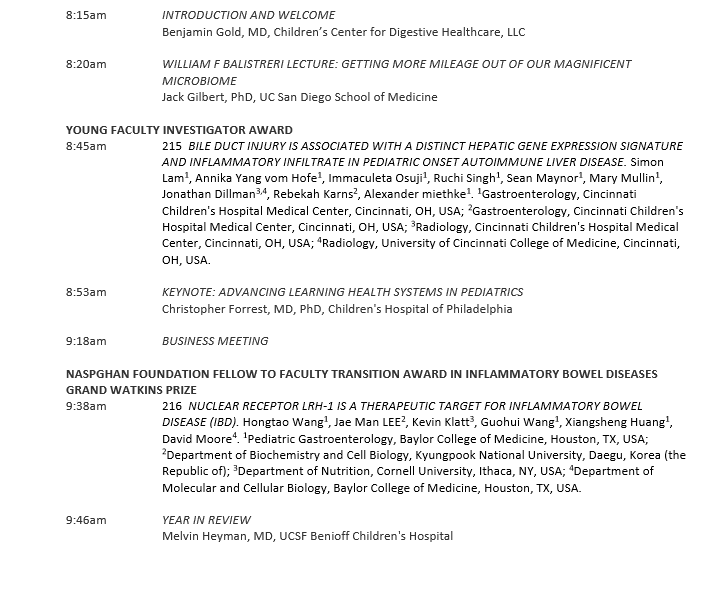
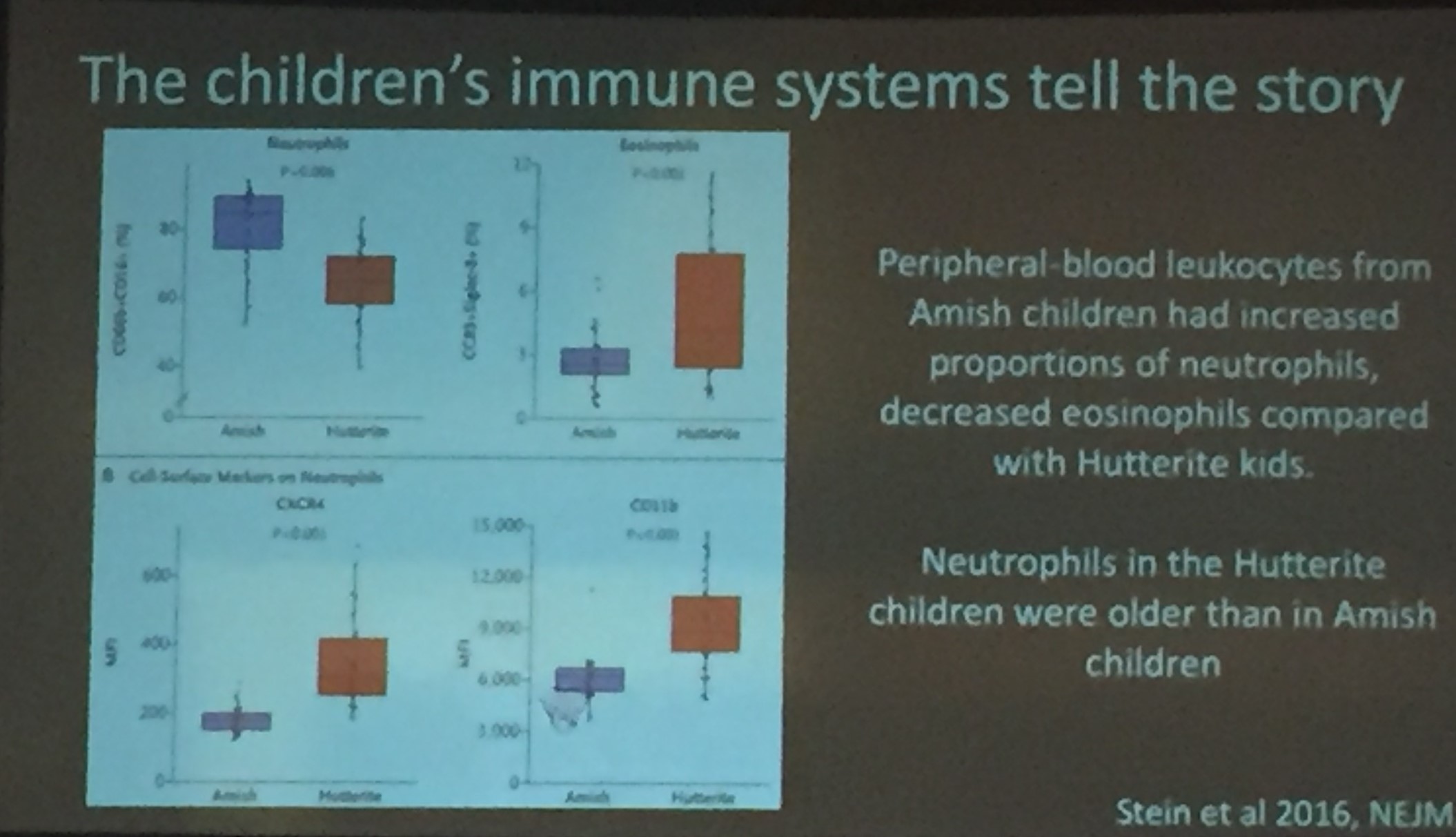
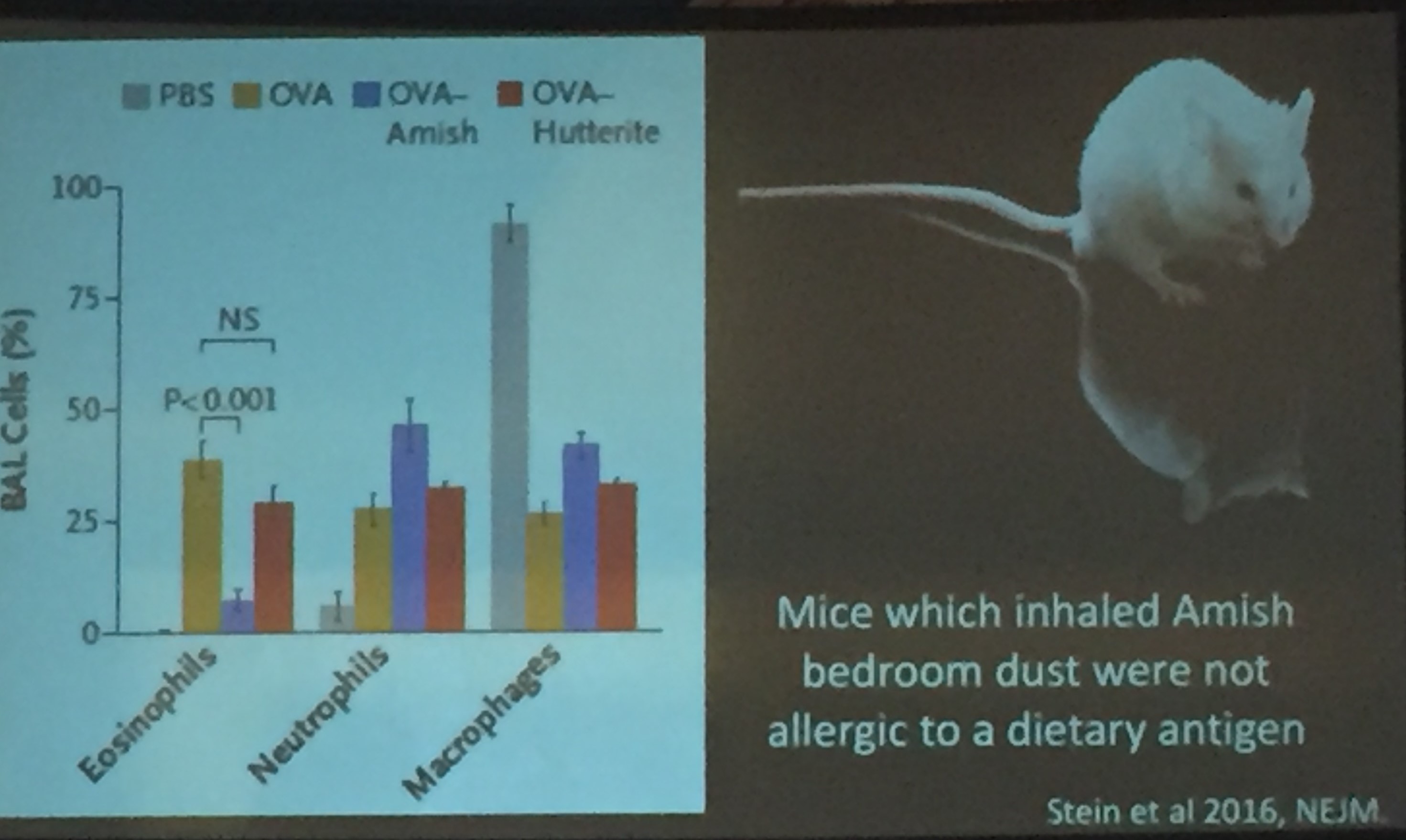
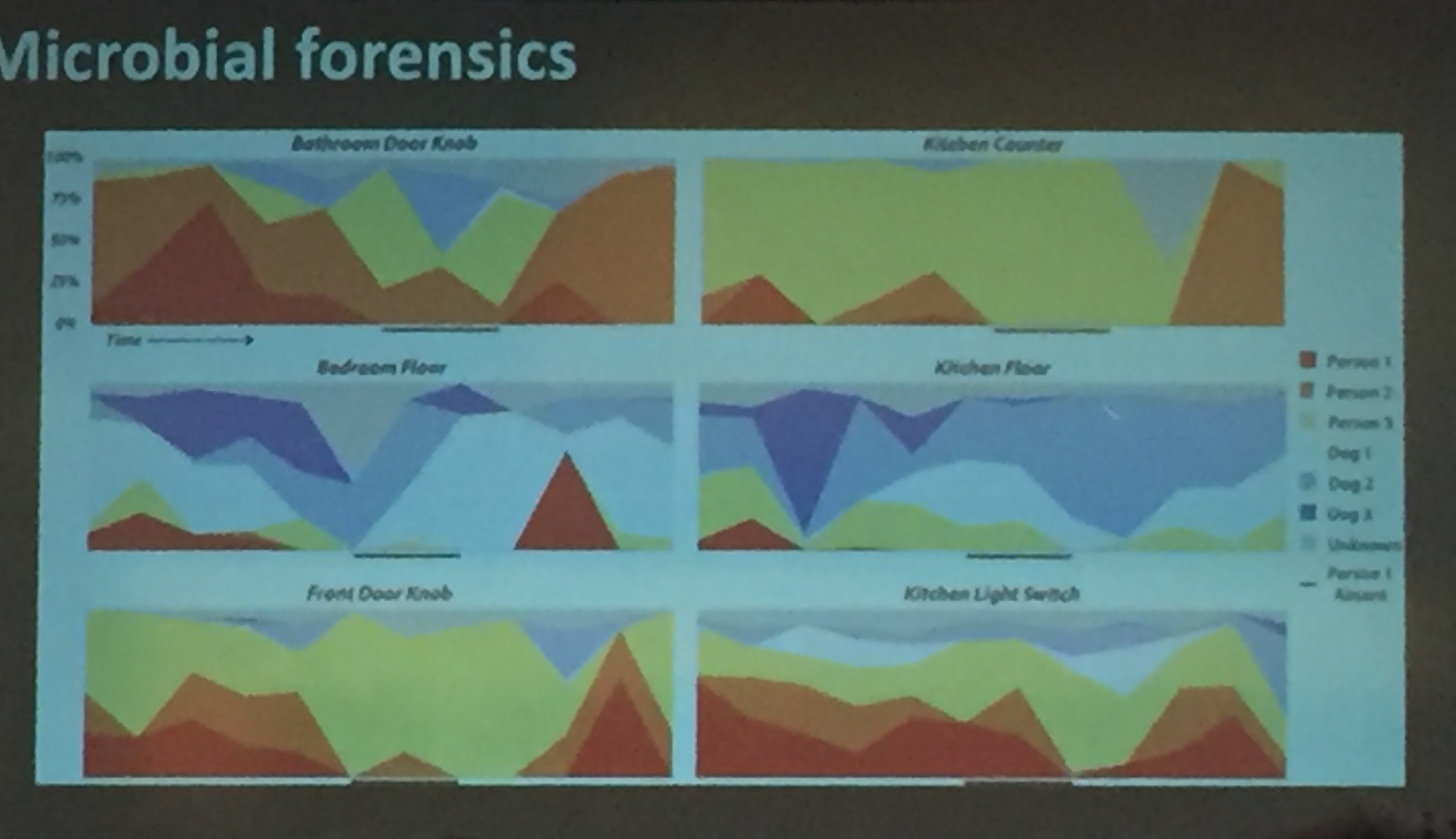
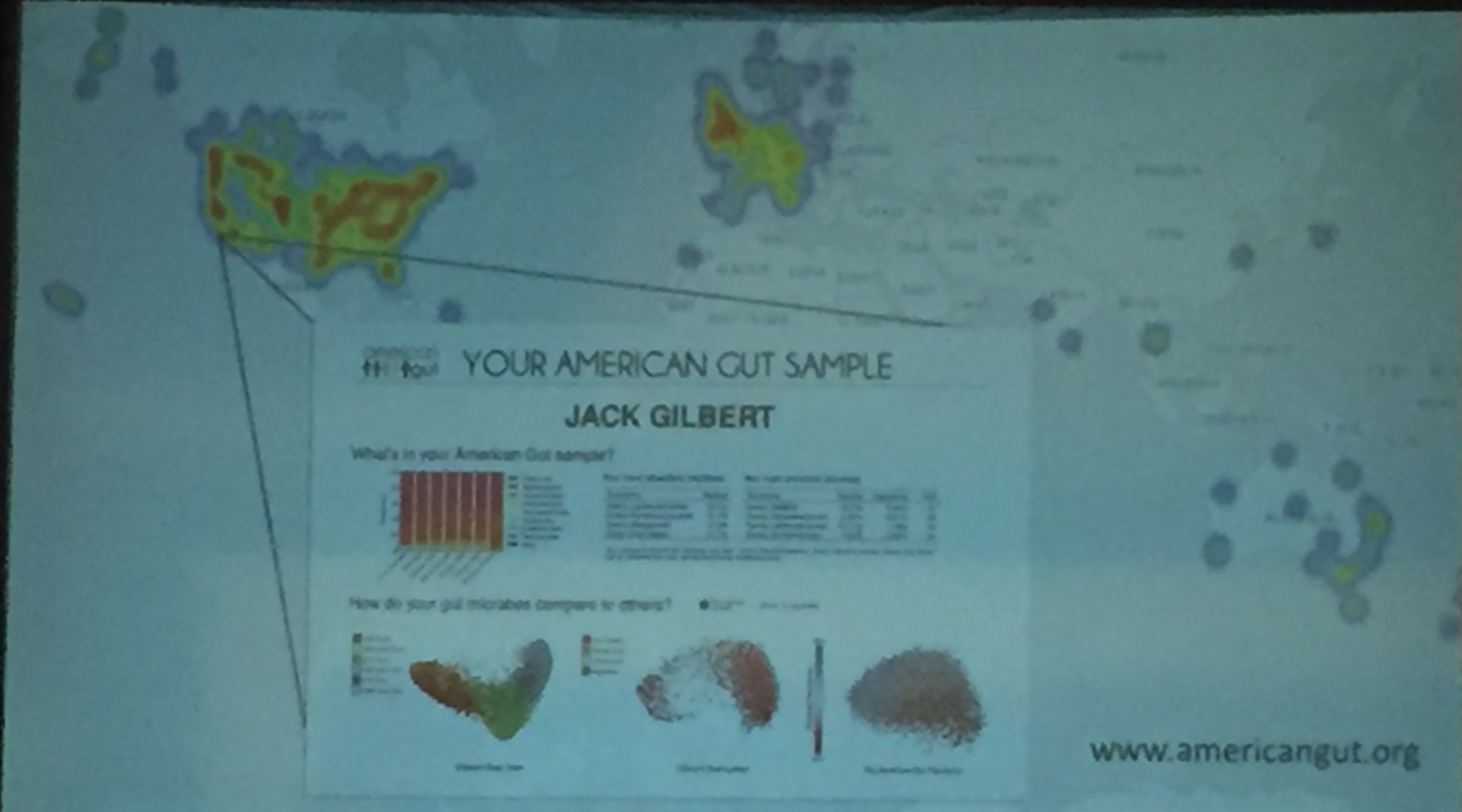
The first speaker, Jack Gilbert, gave the William F Balistreri lecture. Dr. Gilbert has written a book on the topic of our ‘magnificent microbiome,’ Dirt is Good. Here are a few slides:
Related study (not discussed in the talk): A recent study (R Vasapolli et al. Gastroenterology 2019; 157: 1081-91) provided data from 21 healthy adults. Using biopsies from panendoscopy and saliva/fecal samples, the authors found that the fecal microbiome is not representative of the mucosal microbiome. In addition, each GI region had a different bacterial community.
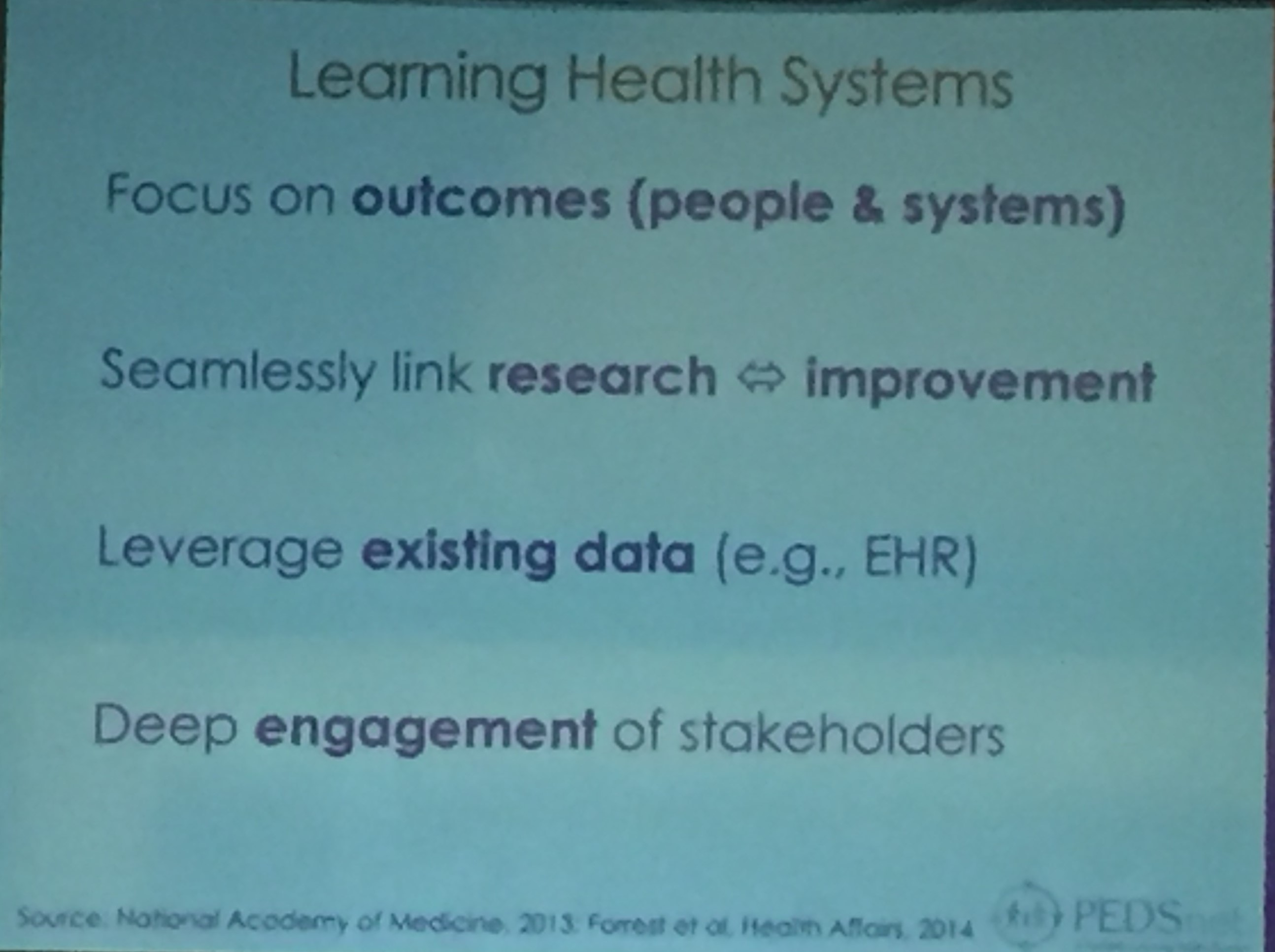
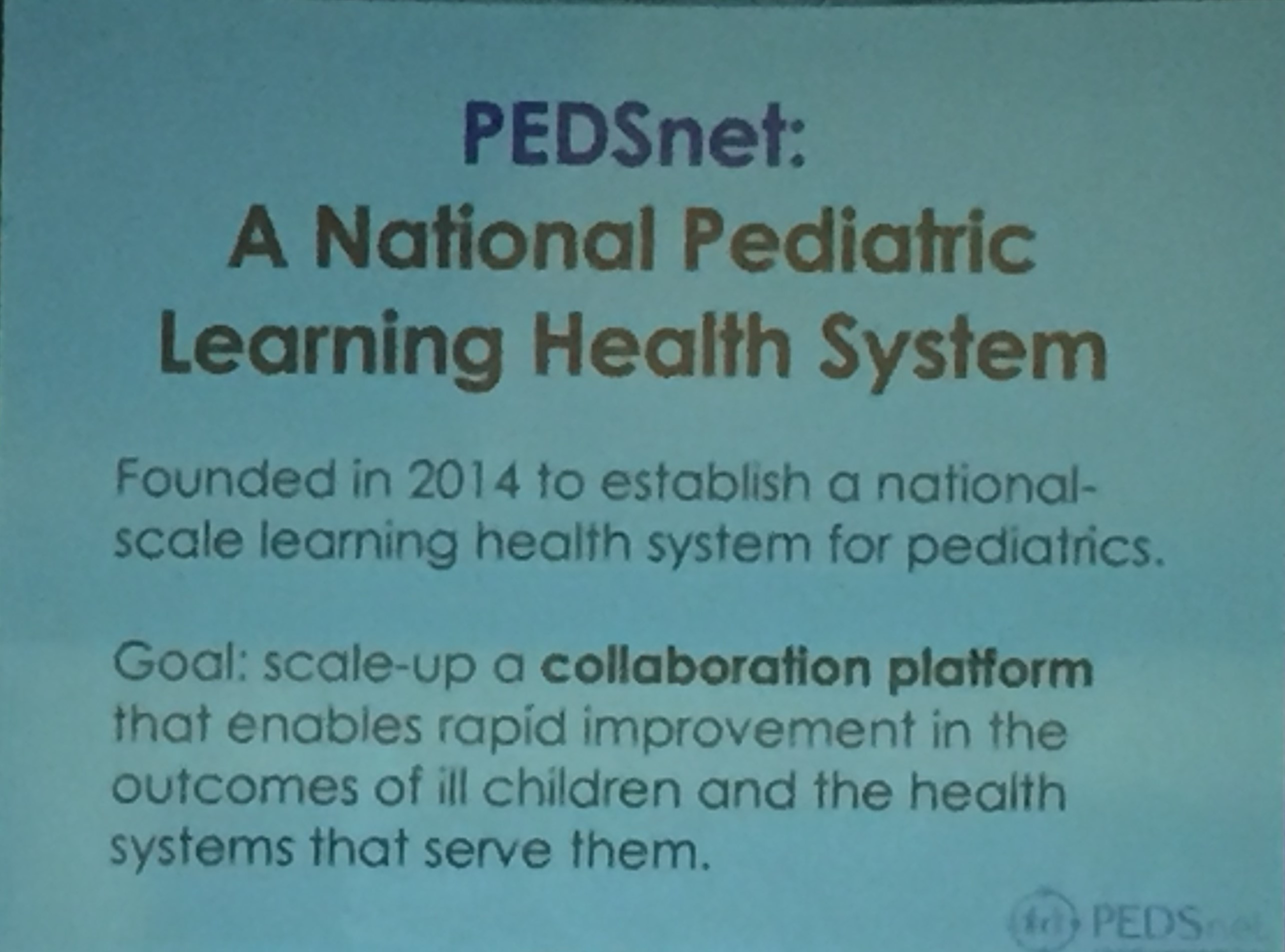
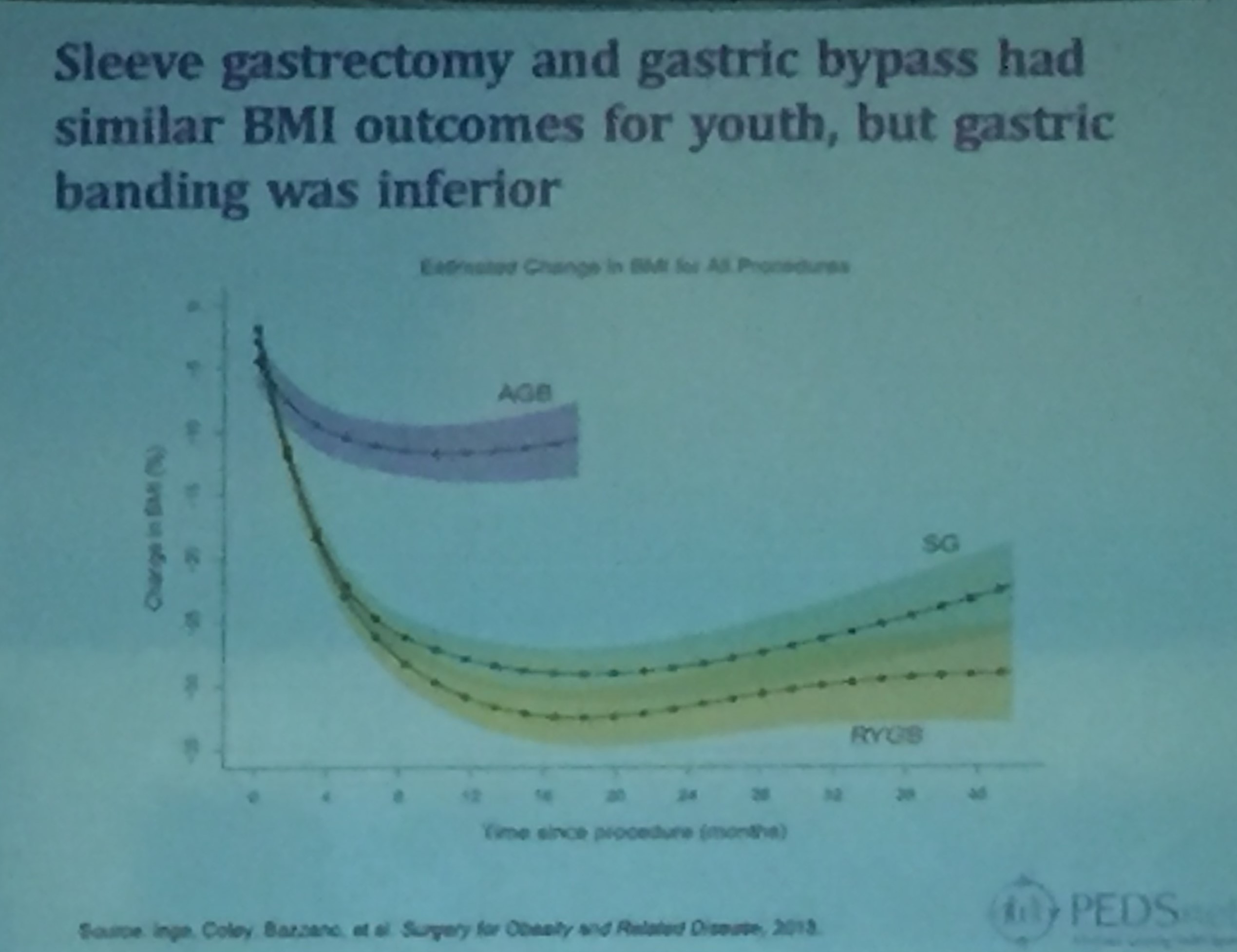
Christopher Forrest gave the keynote lecture on pediatric learning health systems. By collating data from large pediatric health systems, the researchers can determine more quickly how effective treatments are in all pediatric specialties.
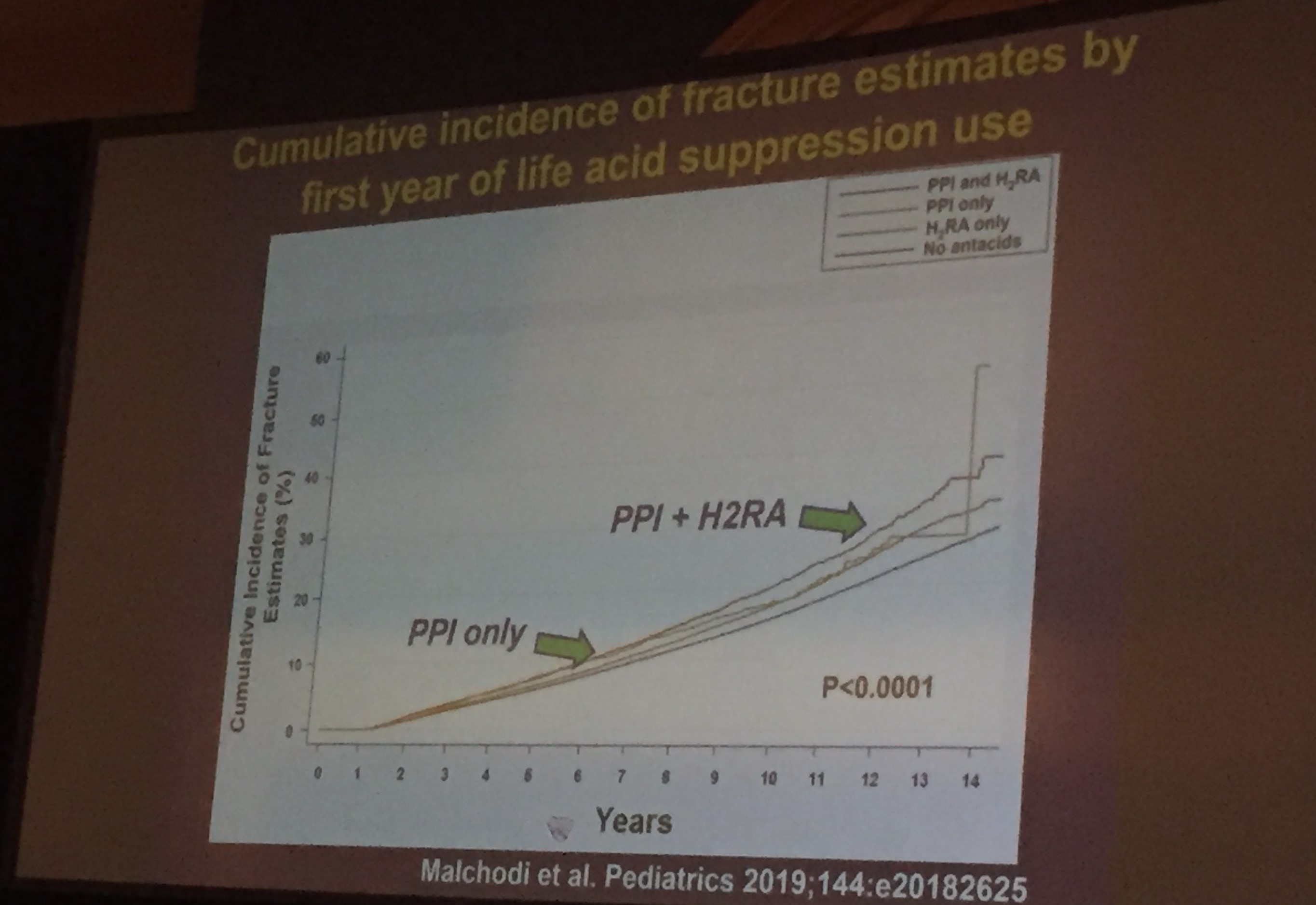
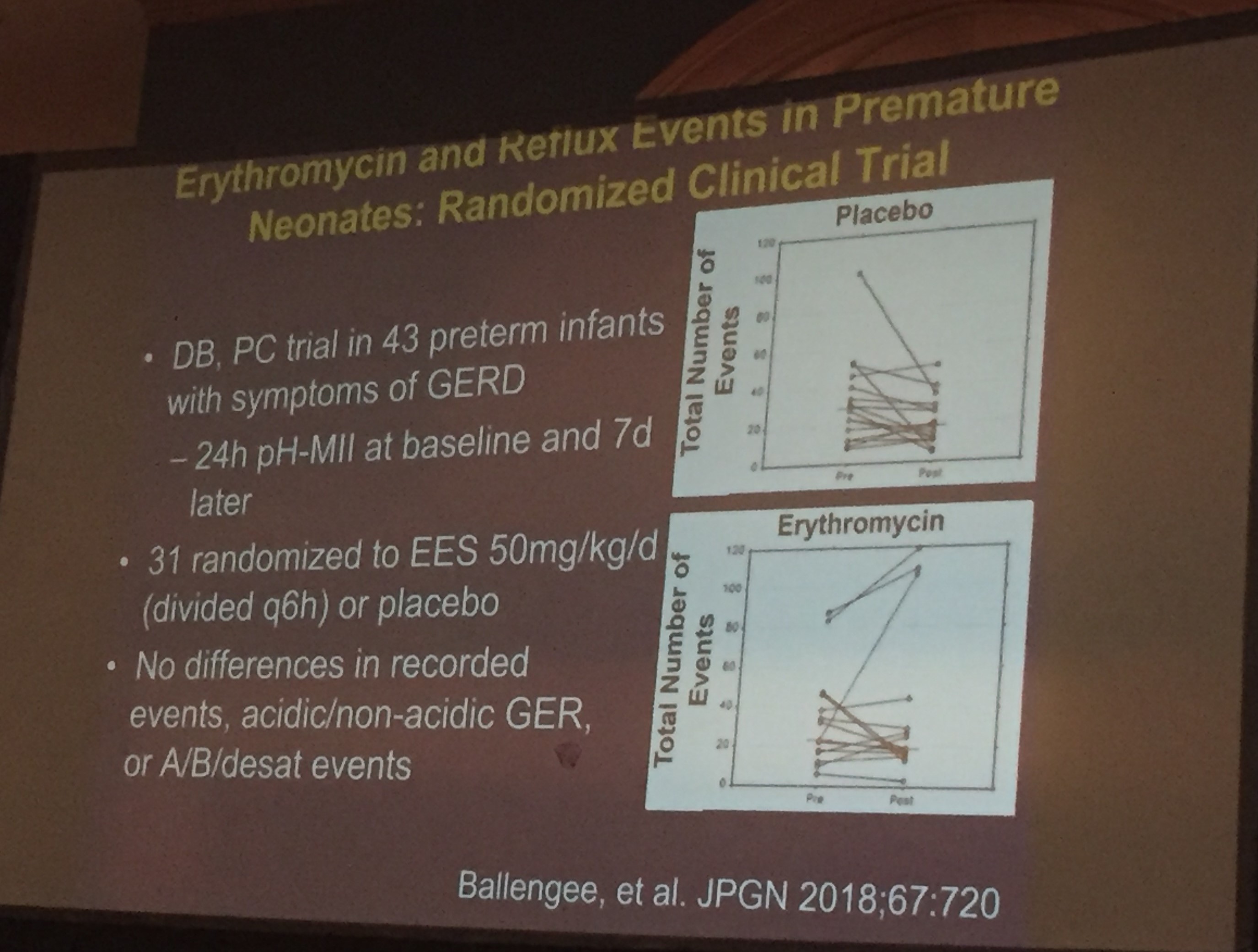
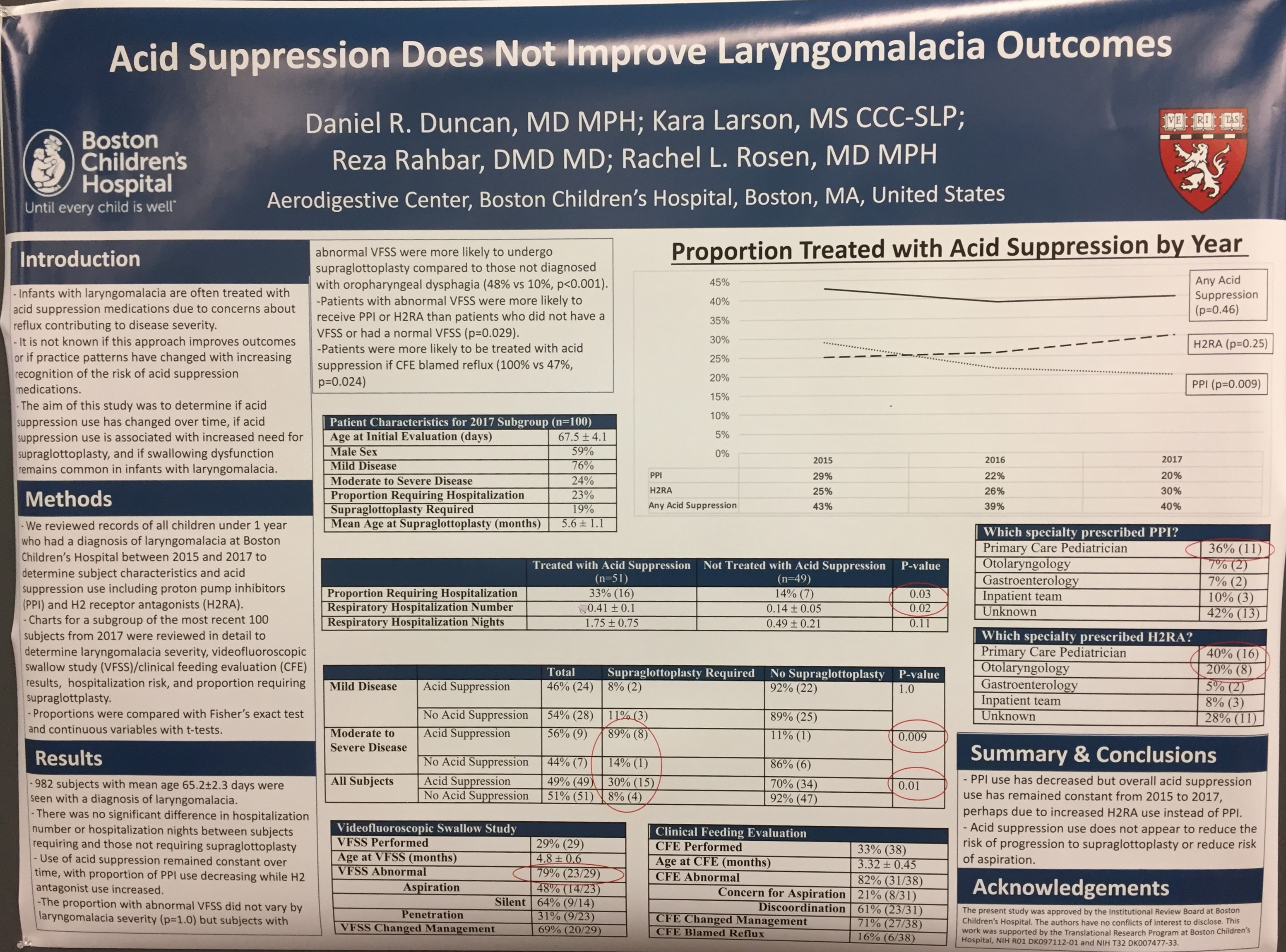
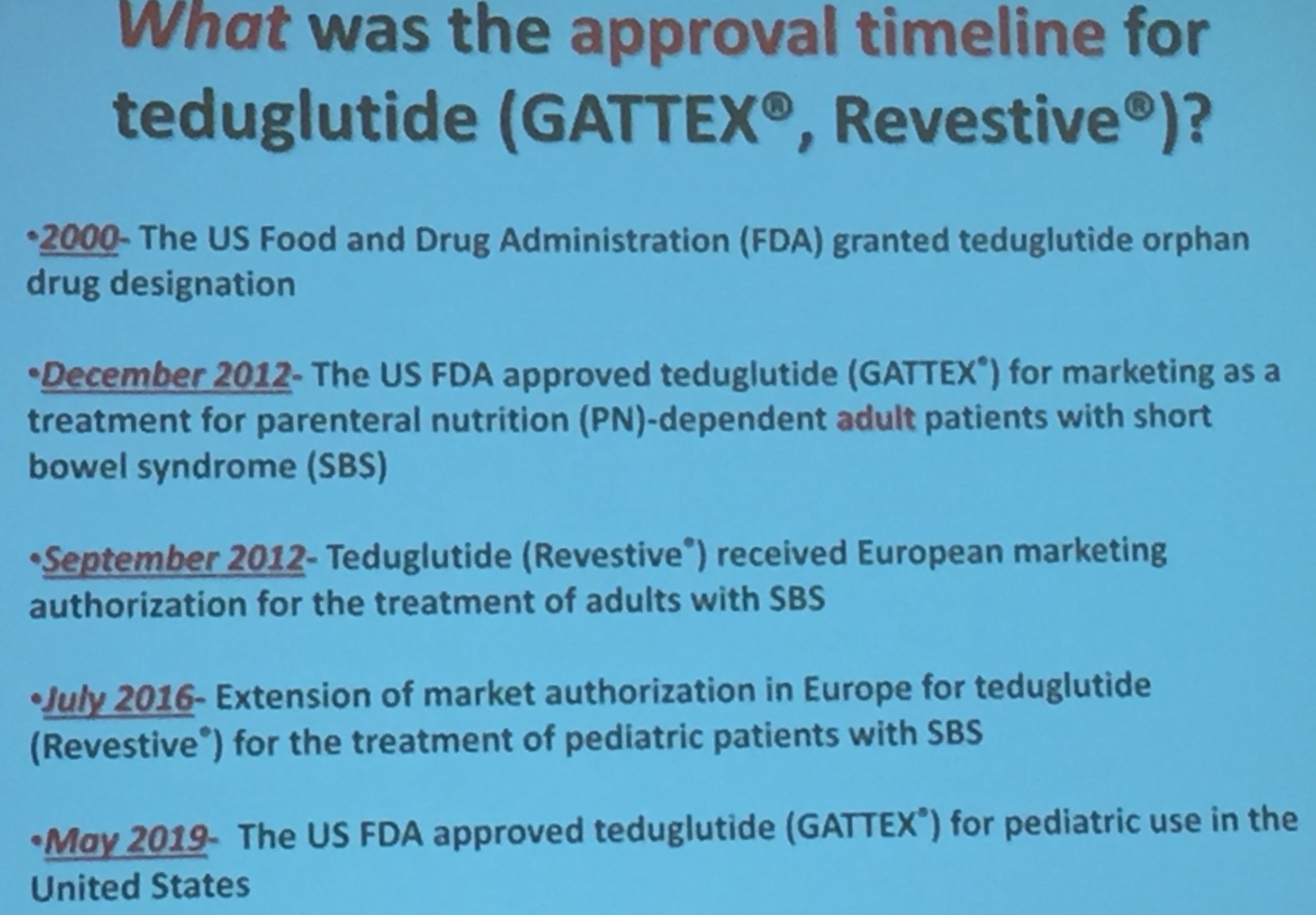
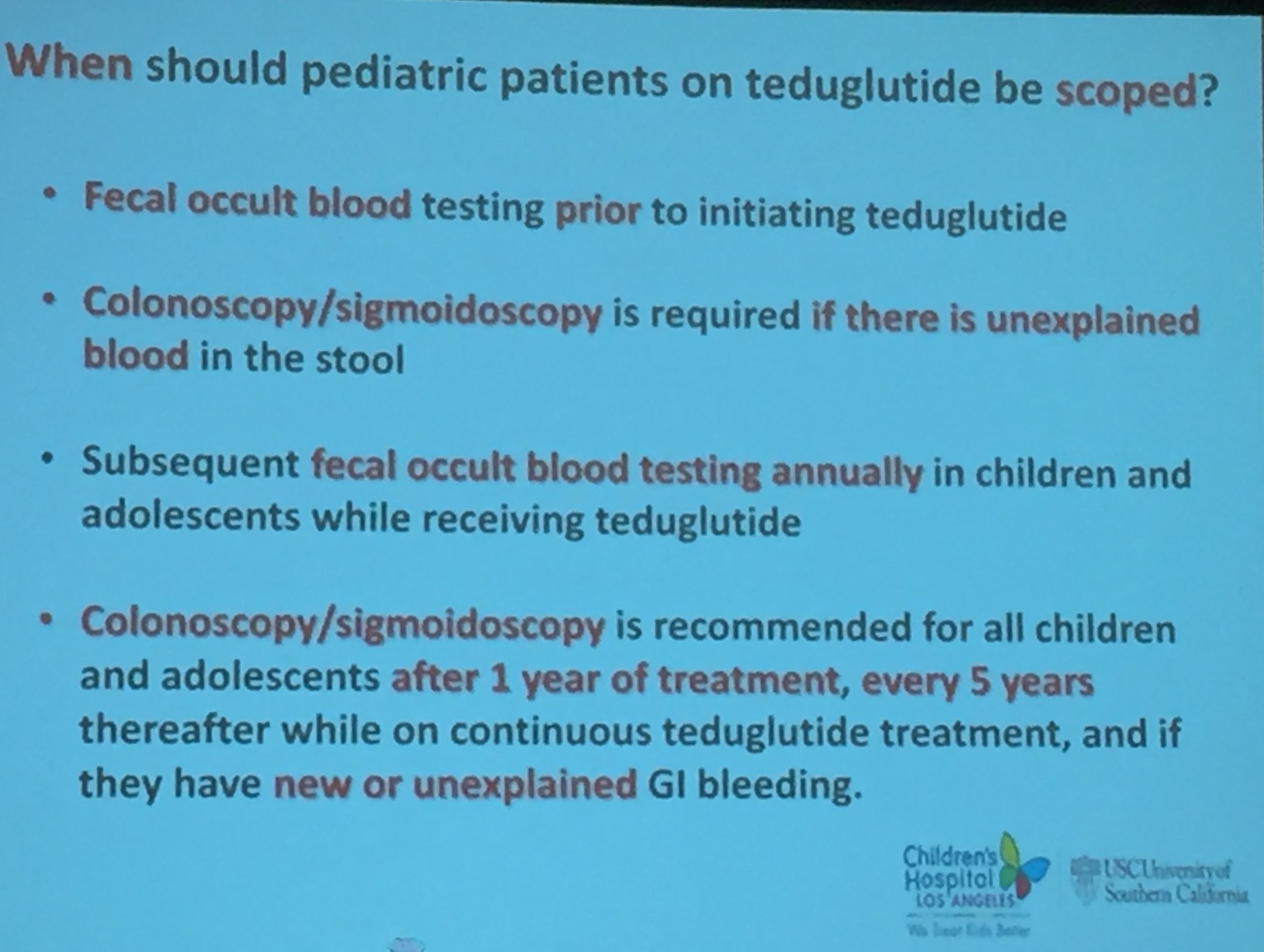
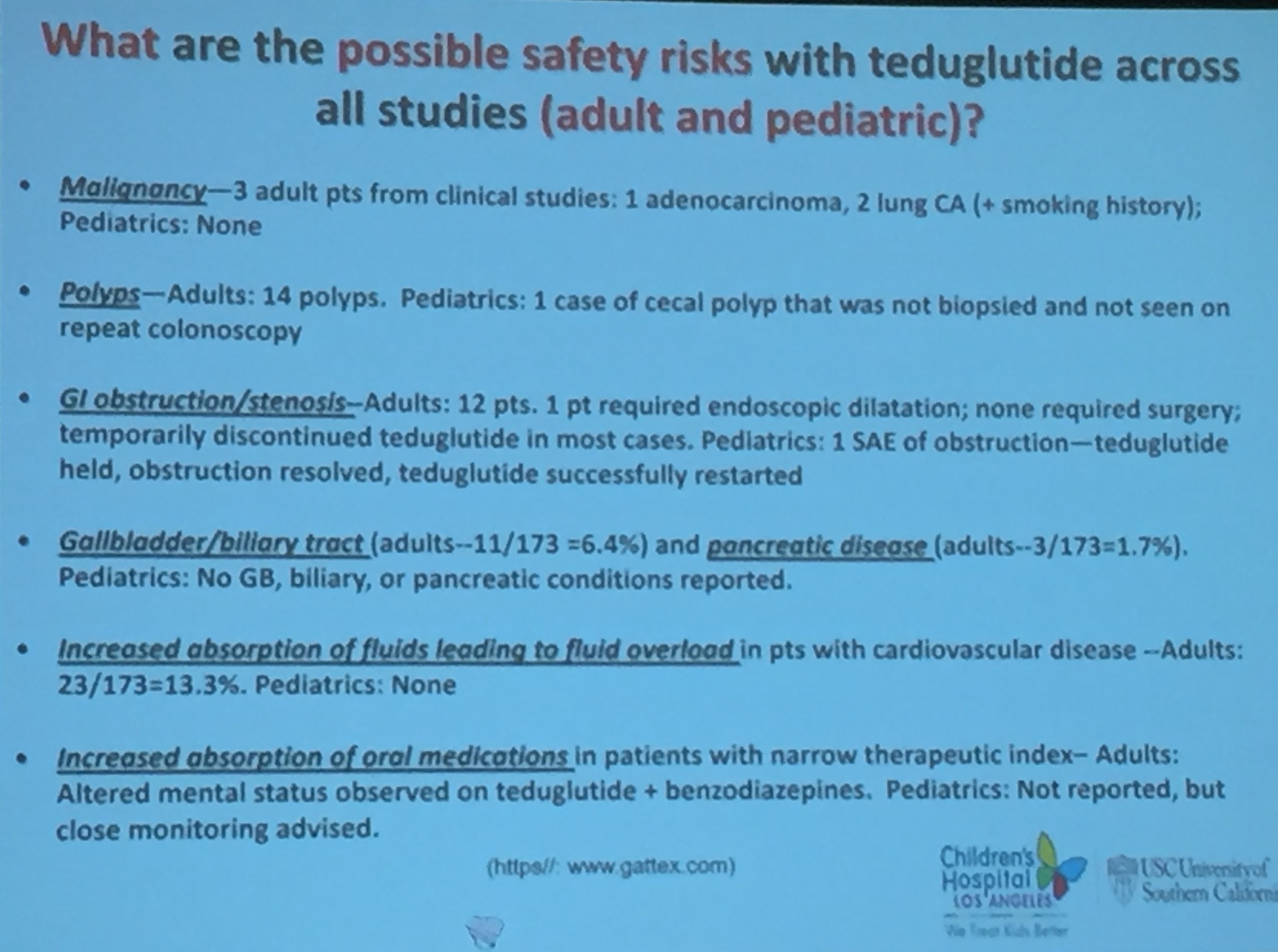
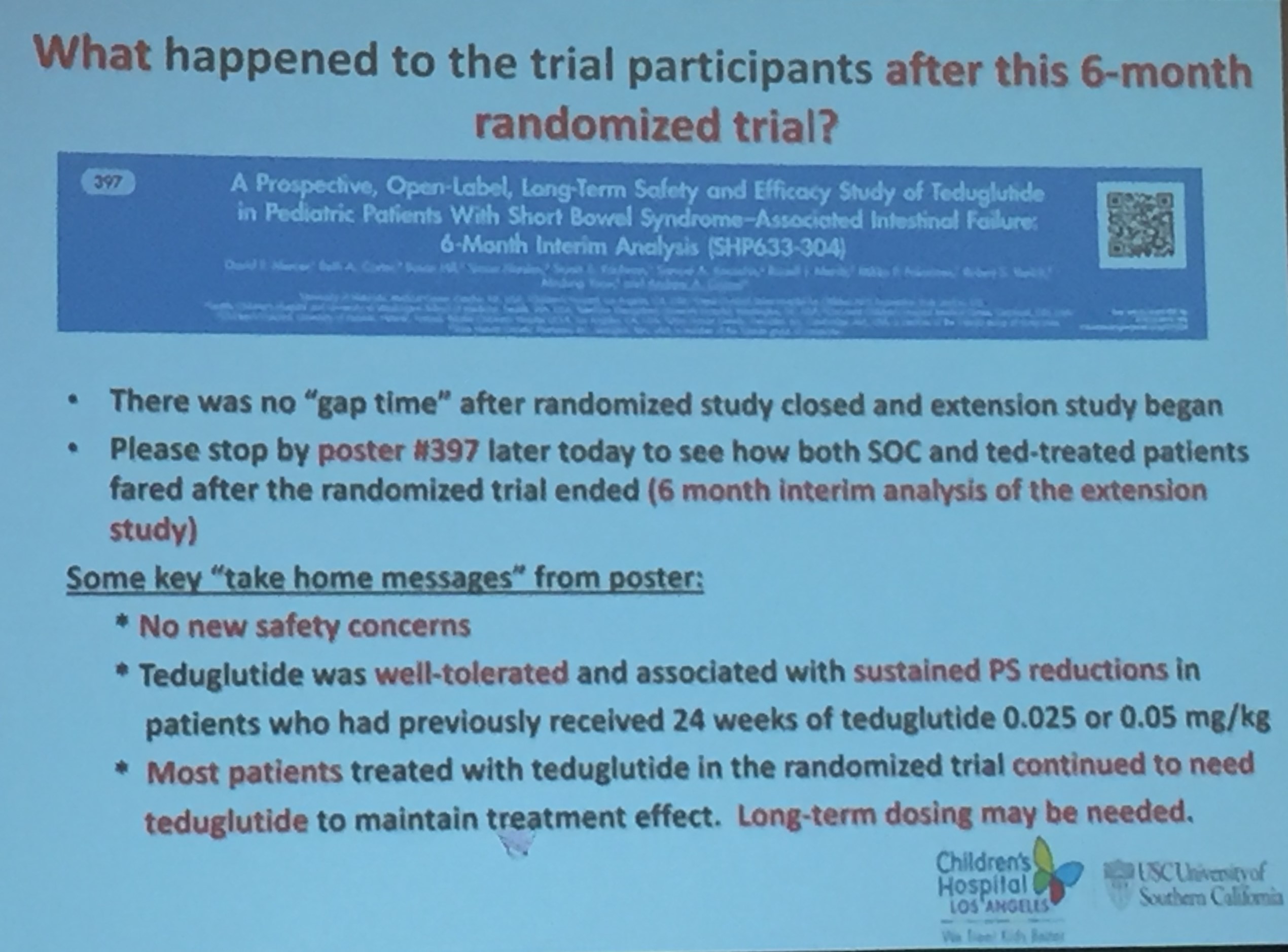
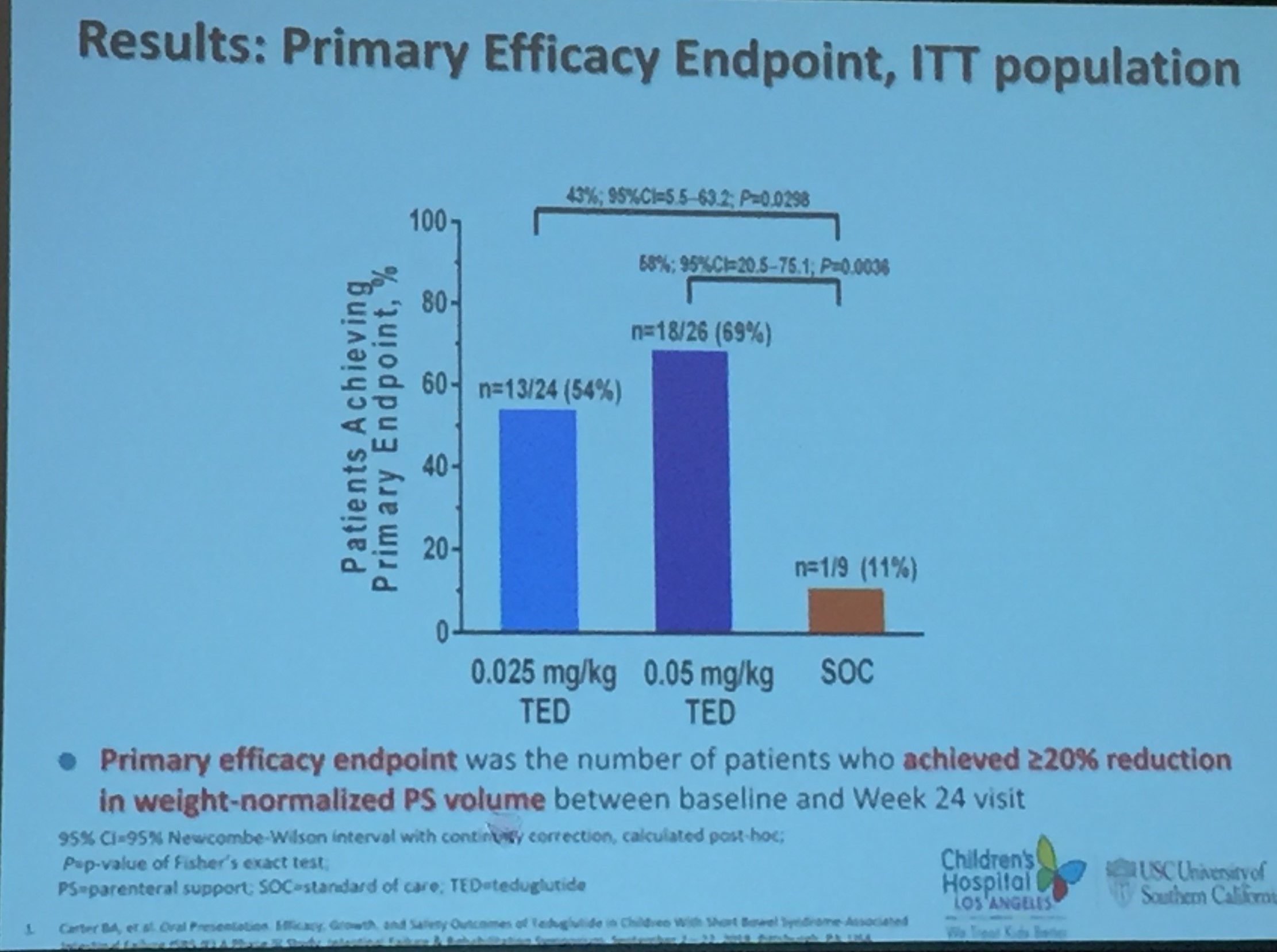
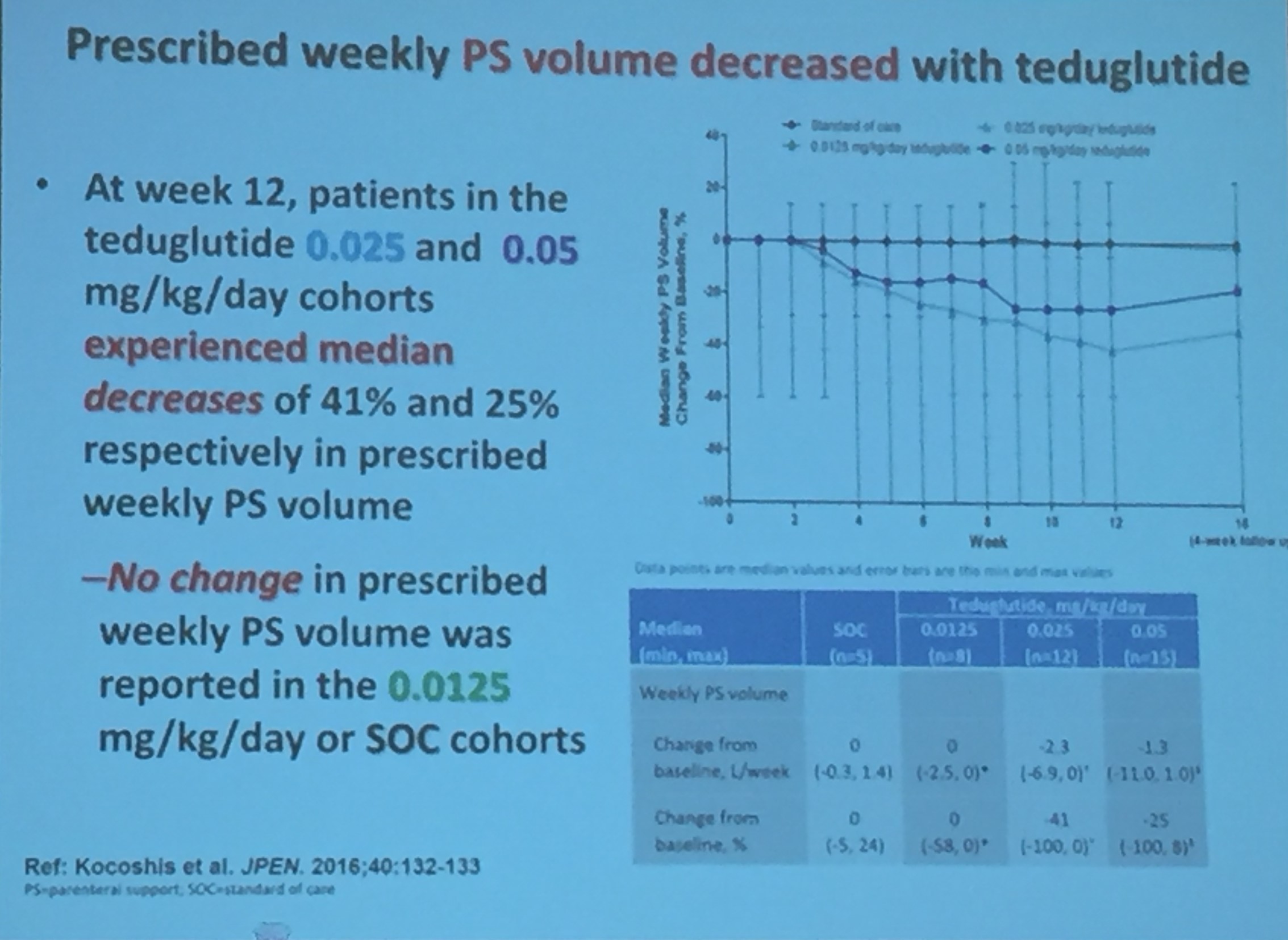
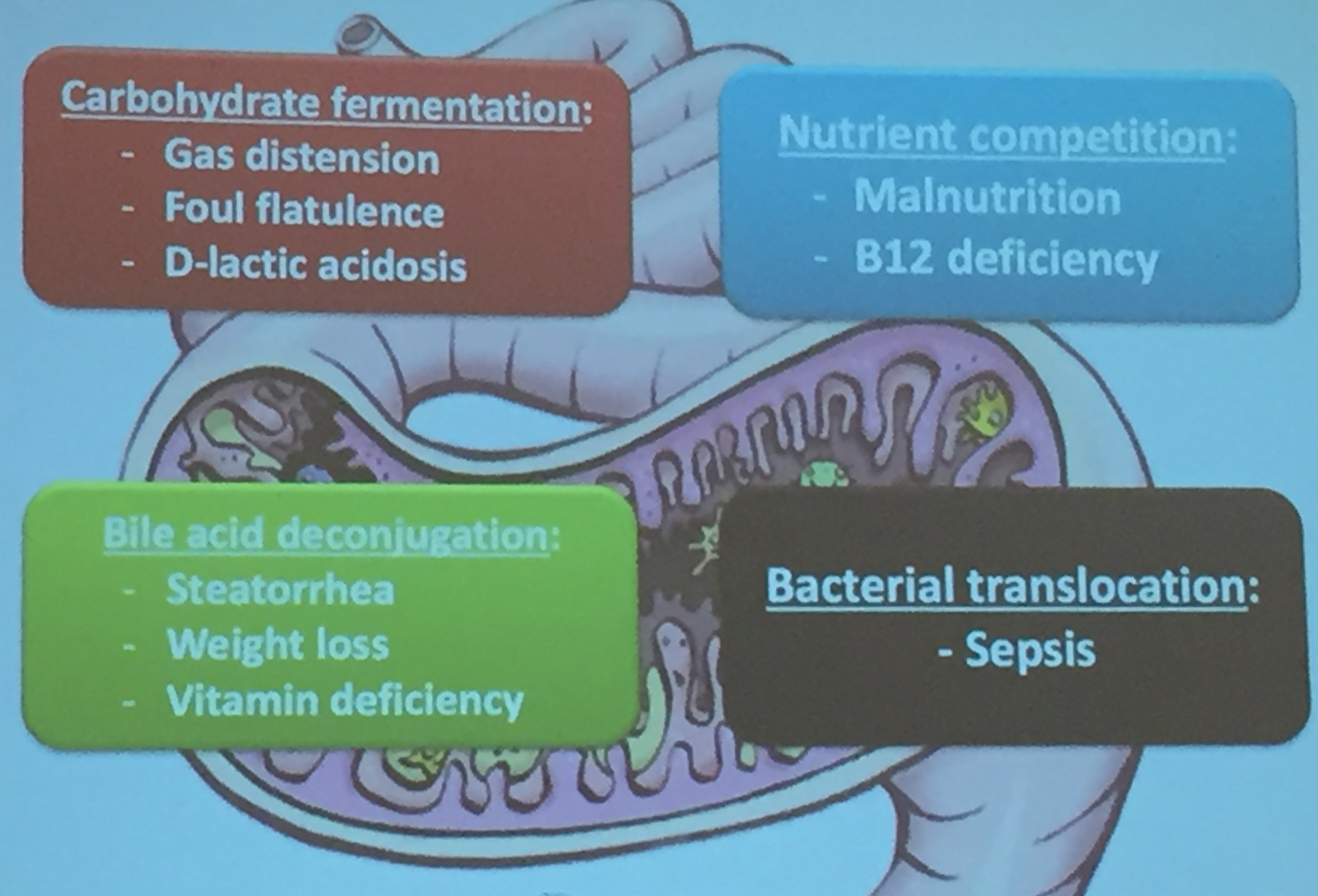
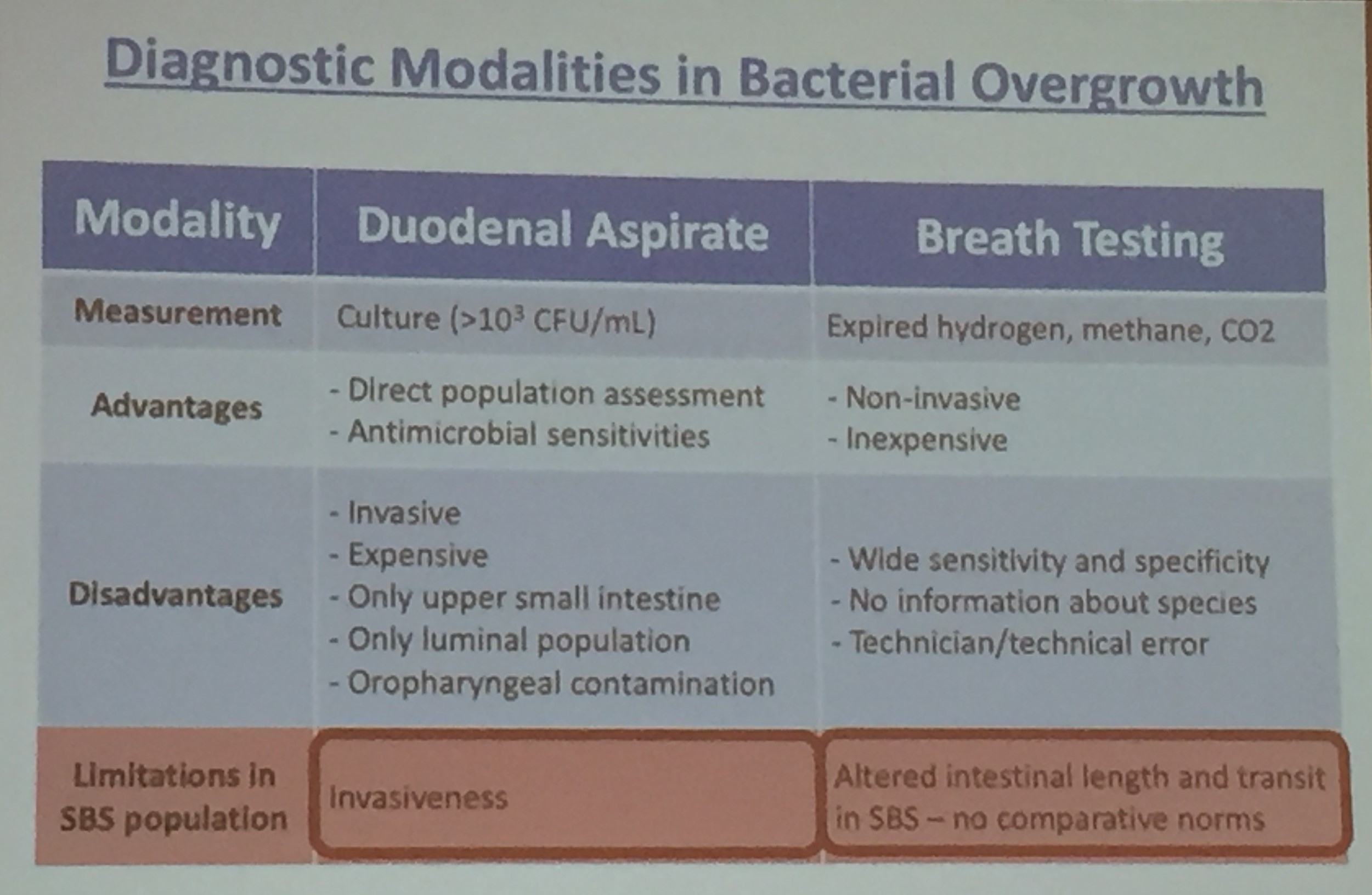
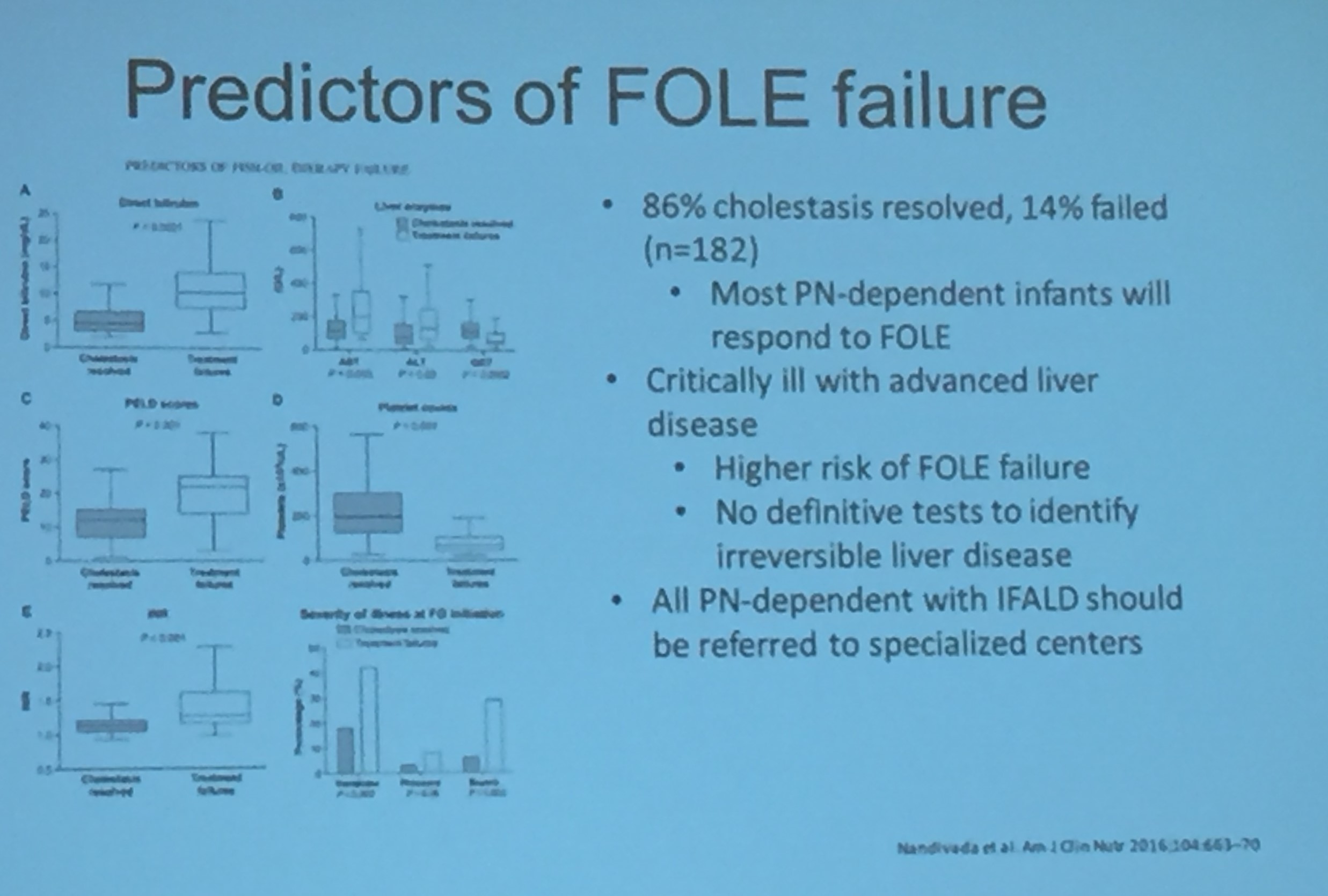
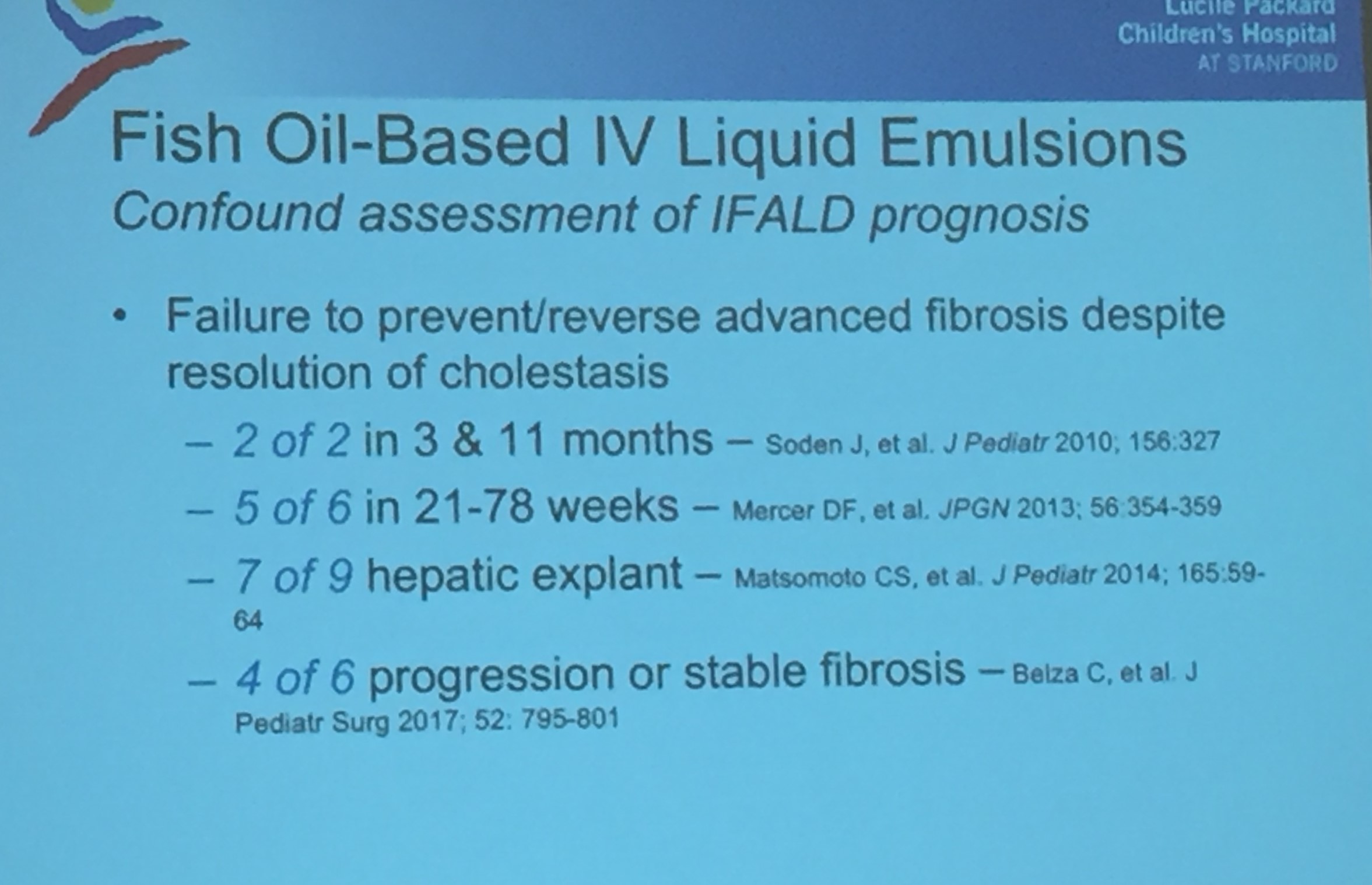
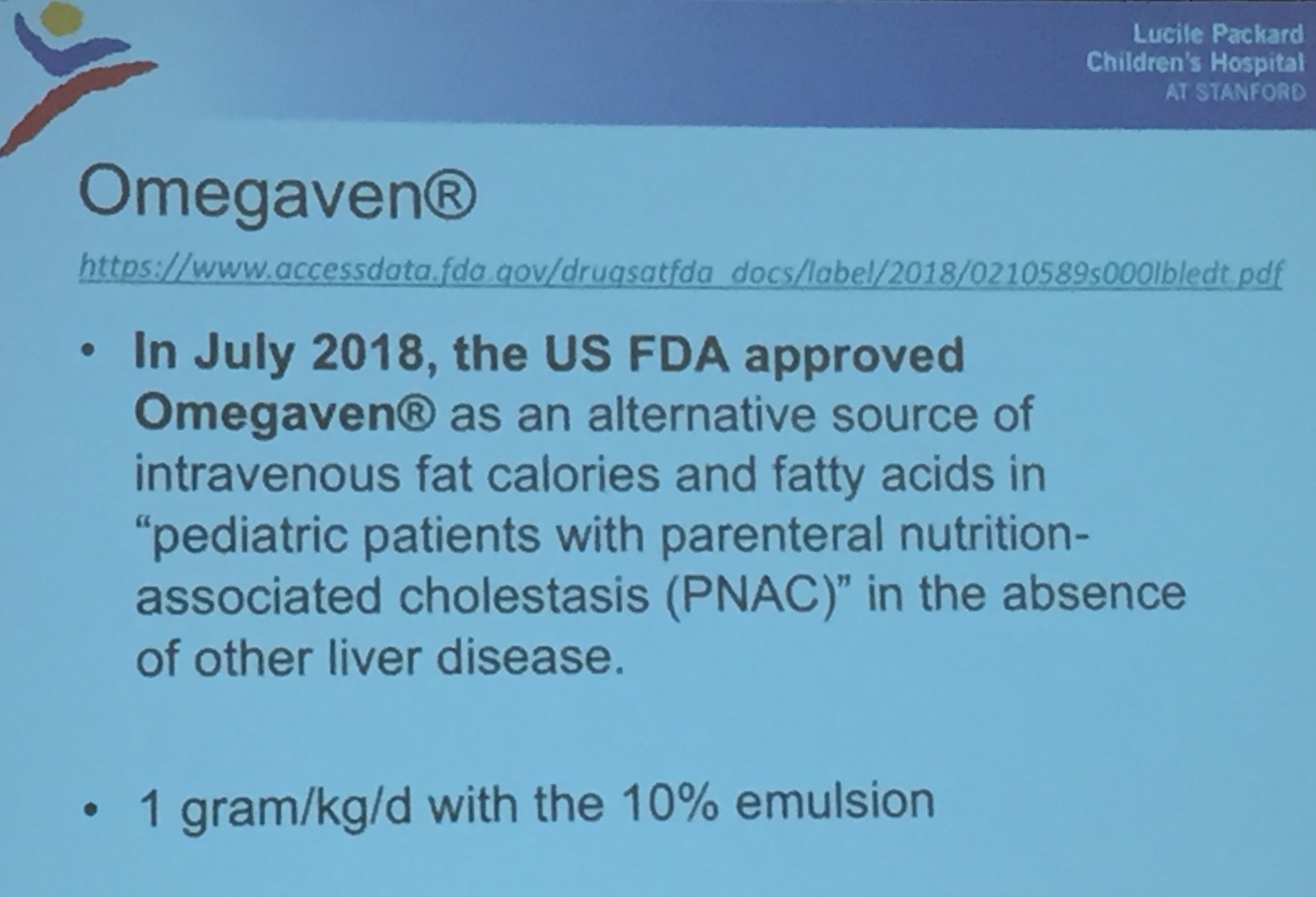
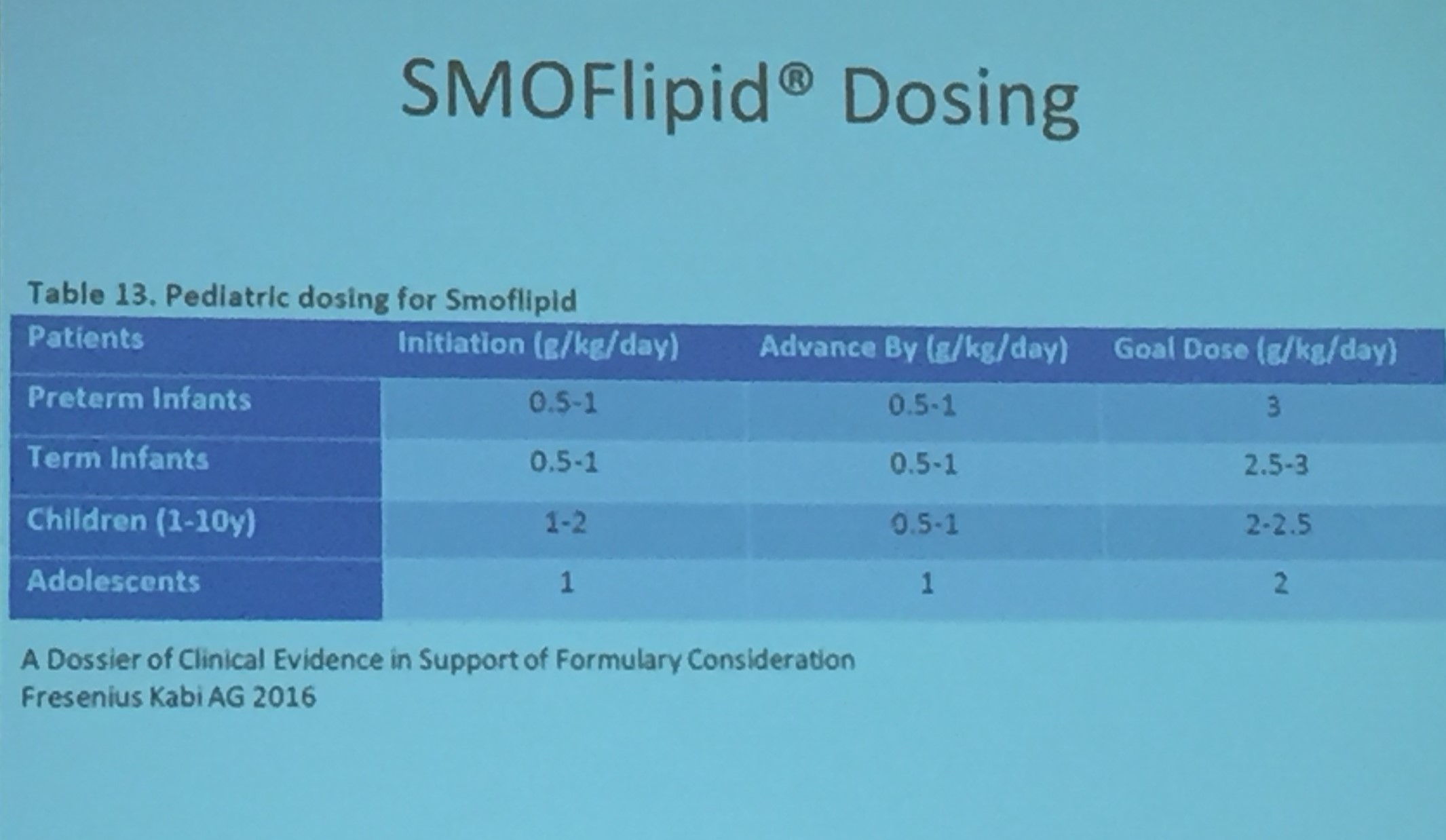
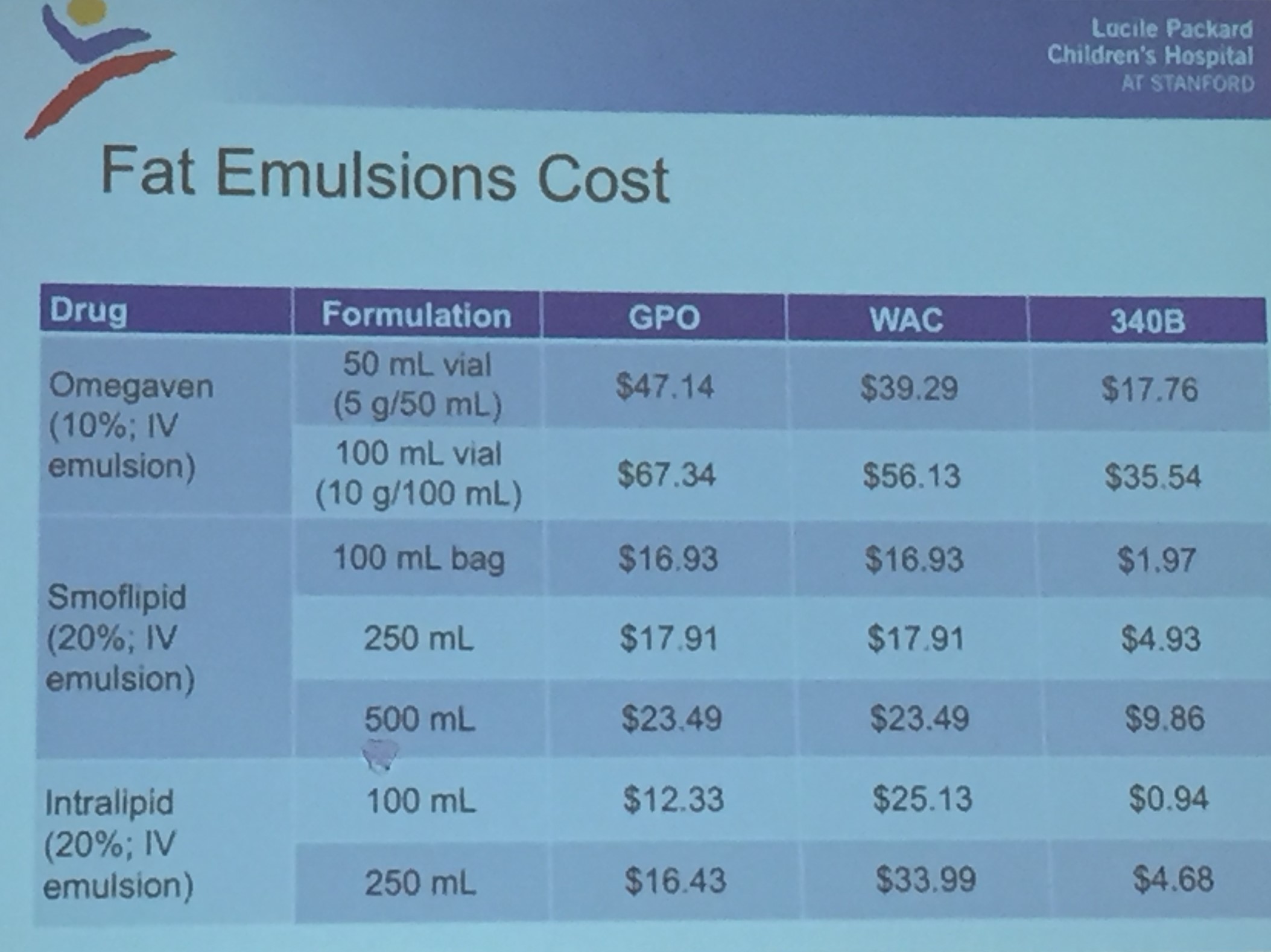
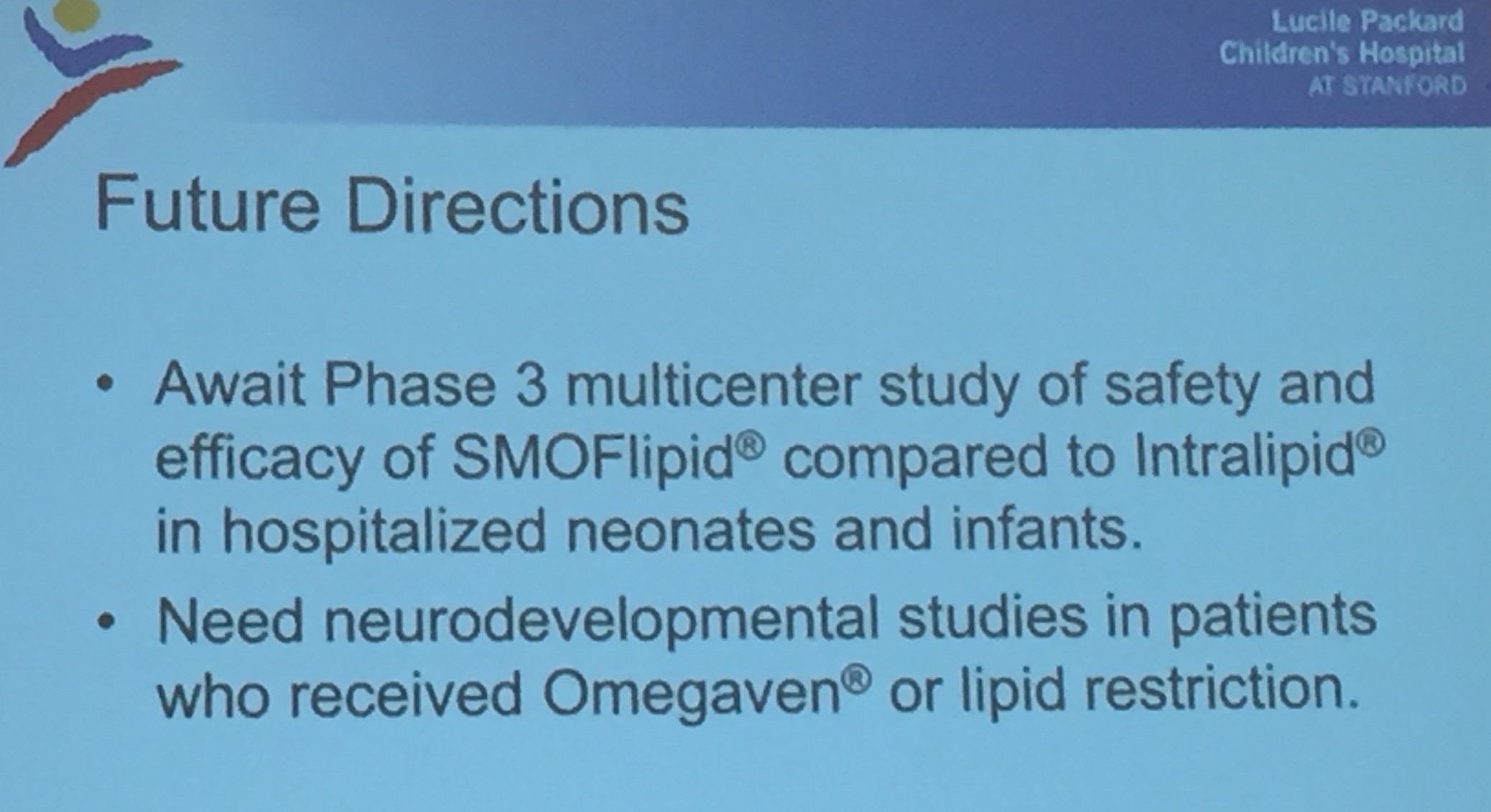
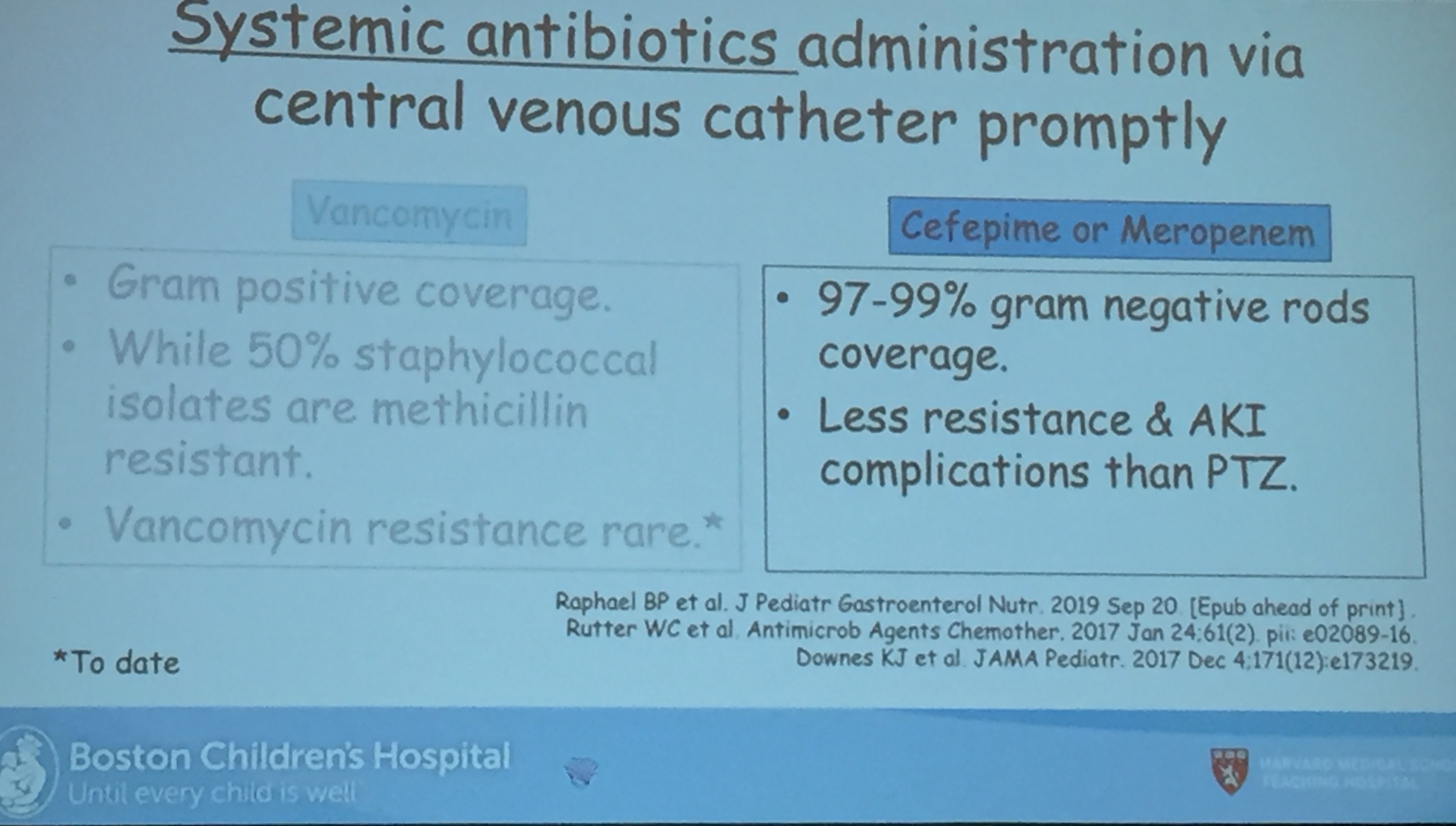
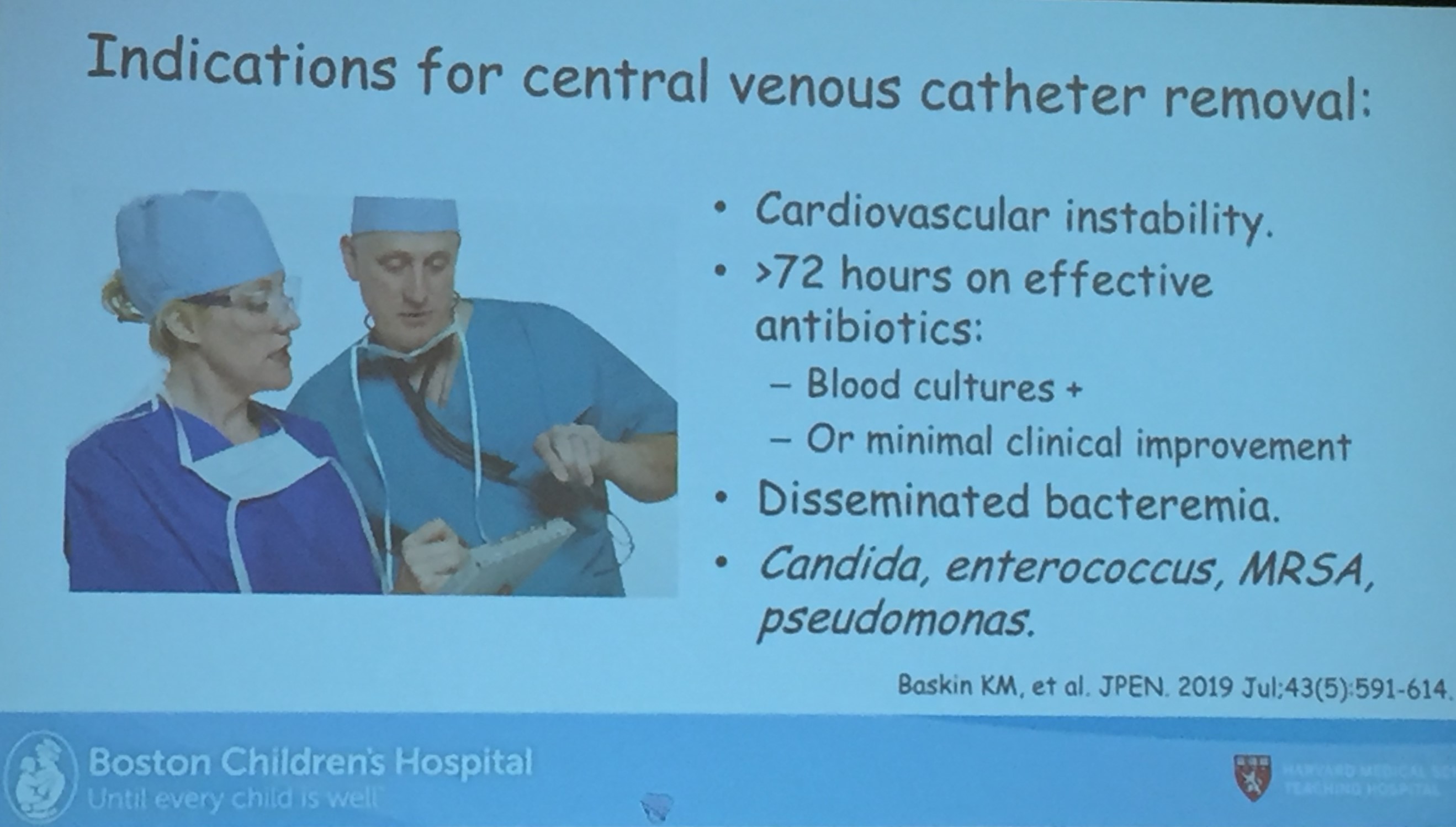
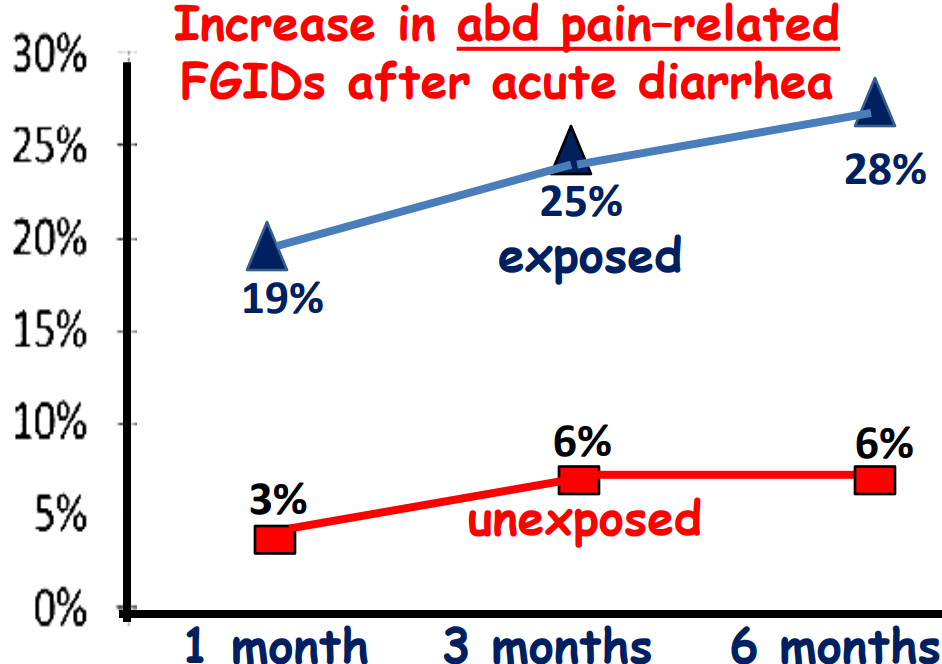
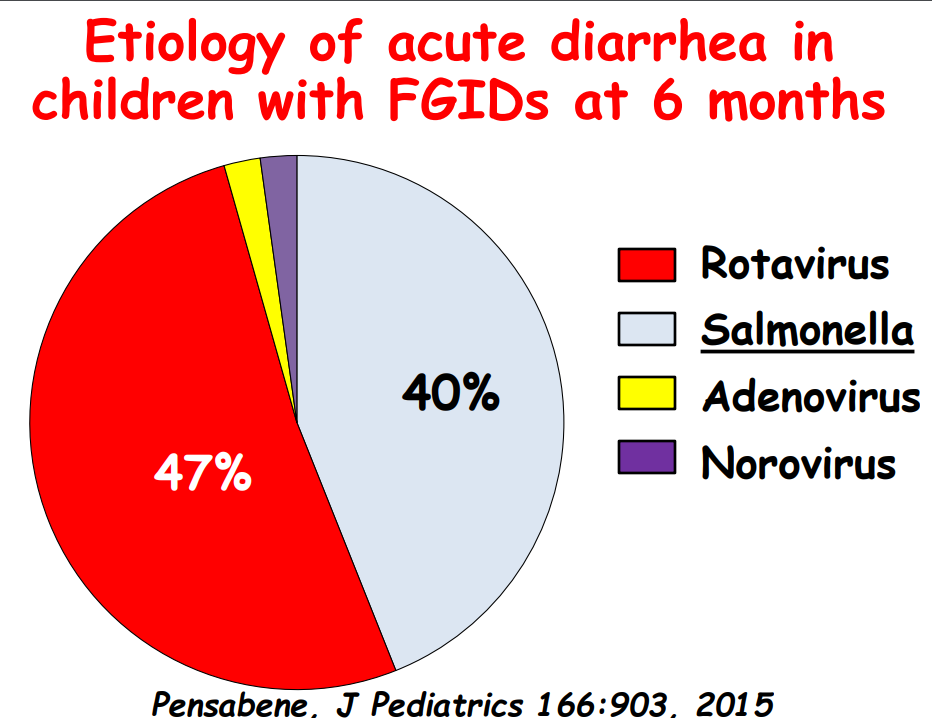
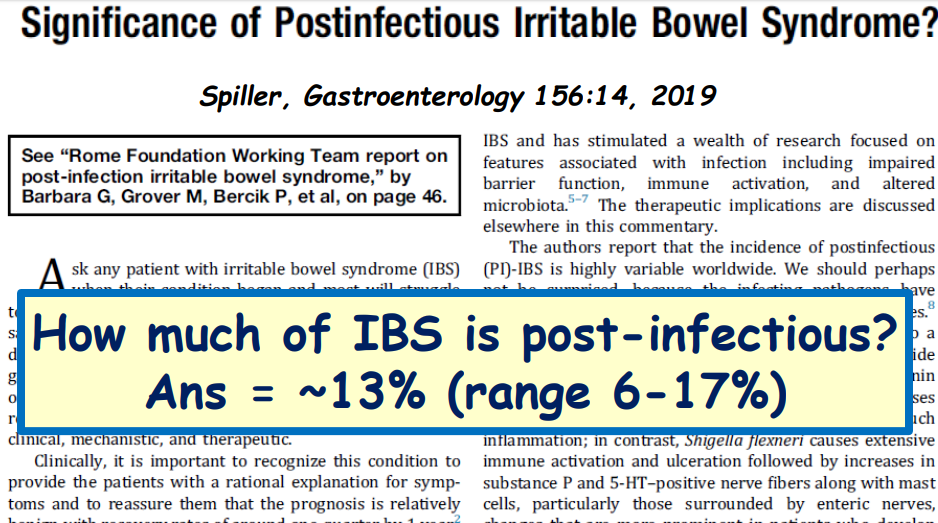
Melvin Heyman, editor of JPGN, provided a good year in review. I only capture a few images.