I am happy to say that this is the last nightcall that I will have this year!
Today, I’ve compiled some of my favorite posts from the past year. I started this blog a little more than 10 years ago. I am grateful for the encouragement/suggestions from many people to help make this blog better. Also, I want to wish everyone a Happy New Year.
This retrospective case-control study identified 93 patients out of 1032 with chronic HCV infection who had a relapse of detectable infection following treatment. Key findings:
12 patients (13%) spontaneously cleared HCV within 6 months after the documented relapse without additional therapy
The spontaneous clearers had low levels of HCV RNA (<4 log IU/mL in 11 of 12) and normal levels of alanine aminotransferase at the time of relapse. Low level RNA was identified in only 1 persistent relapser
There was no significant difference between the spontaneous clearance group and the SVR12 group in magnitude and breadth of HCV-specific T cell responses
The authors note that one limitation of the study was a false positive PCR assay –though this does not negate their message that retesting is important before retreatment
The relatively high relapse rate (9%) in this cohort is likely related to the use of first-generation DAA therapy
The timing of retesting in the 12 with spontaneous clearance was variable. 7 who had repeat testing at 3 months were all negative.
My take: In those with a low level virological relapse after DAA therapy for HCV, it is a good idea to repeat testing before consideration of further treatment.
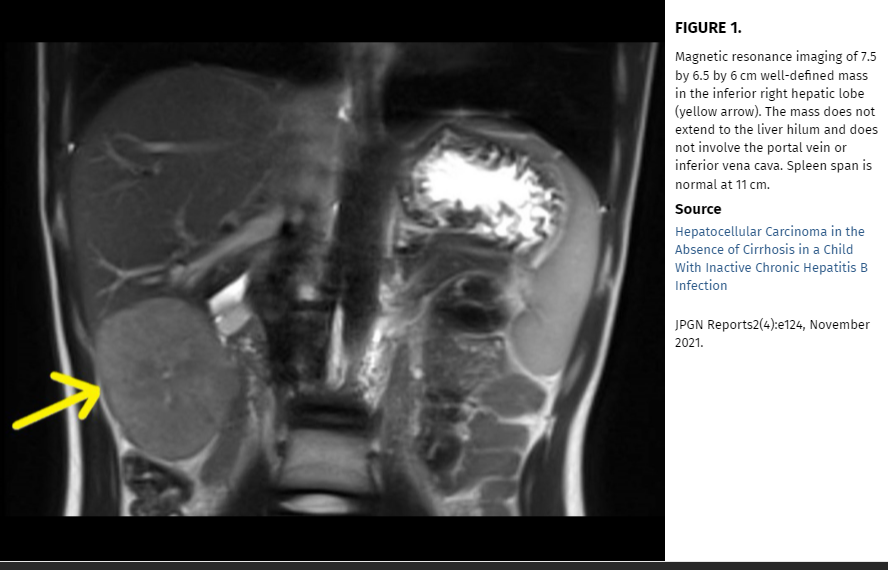
In this case study, the authors “describe an unusual case of a child with chronic hepatitis B infection who developed HCC in the absence of active hepatitis or cirrhosis.” Based on their case report, they advocate for “regular HCC surveillance for all children with chronic hepatitis B, regardless of presence or absence of hepatitis or cirrhosis.”
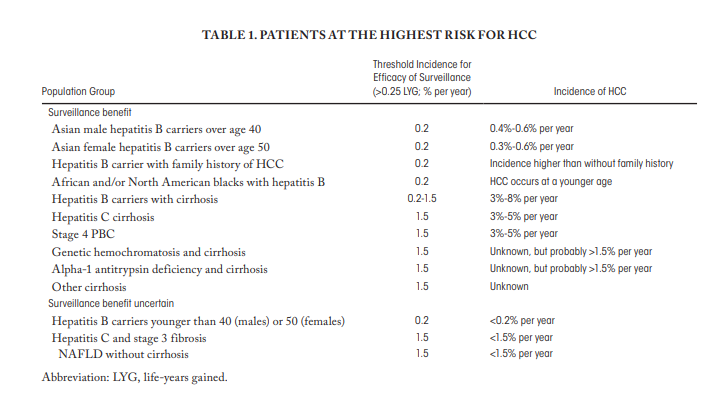
However, the authors suggestions to expand surveillance to all children with hepatitis B is NOT aligned with current expert opinion (by most experts). This potential recommendation deserves (deserved) more commentary in their discussion. The AASLD recommends offering surveillance when the risk of HCC is at least 1.5% per year and the incidence is greater than 0.2% per year, which includes patients with cirrhosis and some non-cirrhotic hepatitis B carriers [7]. In a study from Taiwan (blog post: HBV Vaccination Prevents Cancer), the authors showed the beneficial effects of vaccination: HCC incidence per 105 person-years was 0.92 in the unvaccinated cohort and 0.23 in the vaccinated birth cohorts. This study also showed how rare HCC cases are in children; thus, showing benefit of vaccination was impressive.
My take: This case report is helpful in emphasizing the risk of HCC in patients with HBV, even in those without significant risk factors. However, at this time most experts do not recommend surveillance in those with a low risk of developing HCC.
HBV Vaccination Prevents Cancer In Taiwan: HCC incidence per 105 person-years was 0.92 in the unvaccinated cohort and 0.23 in the vaccinated birth cohorts.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
Background: “Despite the progress made over the last 40 years the rate of indeterminate cases [of acute liver failure] remains ~30%”
Methods: The authors identified 41 children (<10 yrs) with DNA sample availability who were admitted to King’s College Hospital, London, with ALF of indeterminate etiology (2000-2018). In addition, trio exome sequencing was performed on 4 children admitted during 2019.
Key Findings:
Homozygous and compound heterozygous variants were identified in 8 out of 41 children (20%) and 4 out of 4 children (100%) in whom targeted and exome sequencing were carried out, respectively
The genes involved were NBAS (3 children); DLD (2 children); and CPT1A, FAH, LARS1, MPV17, NPC1, POLG, SUCLG1, and TWINK (1 each). Variants in NBAS and mitochondrial DNA maintenance genes were the most common findings.
My take: Genetic testing for underlying metabolic/metabolic disorders is important to further determine the reasons for ALF. Given the potential need for liver transplantation, obtaining these results quickly will be crucial. In addition, interpretation of the results in some cases will be difficult.
Patrick Reeves passed along the following helpful information about the NASPGHAN toolbox:
The NASPGHAN Fellows committee, working in close partnership with the NASPGHAN Technology and Training committees, has developed an App named, “The NASPGHAN Toolbox”.
The App is equipped with ready access to: clinical calculators, guidelines and algorithms, medication guides, patient education resources, and more. You can access the Toolbox via its URL (https://toolbox.naspghan.org/) on your phone or computer.
The NASPGHAN team hopes this will enhance your day-to-day patient care of children with gastrointestinal disorders.
Some highlights:
Under scores/calculators: Paris Classification, PUCAI, PCDAI, Mayo Score, PELD, MELD
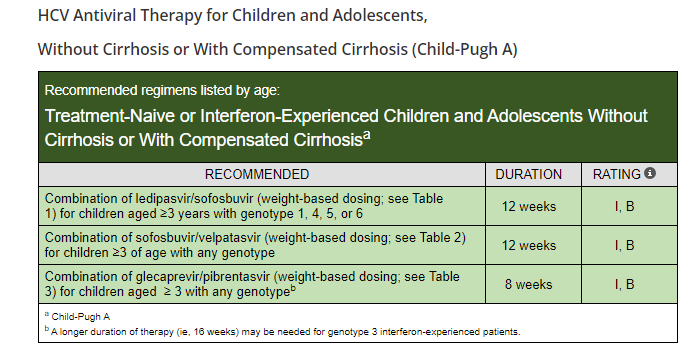
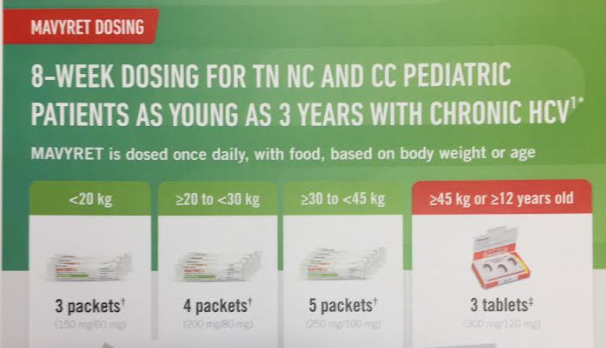
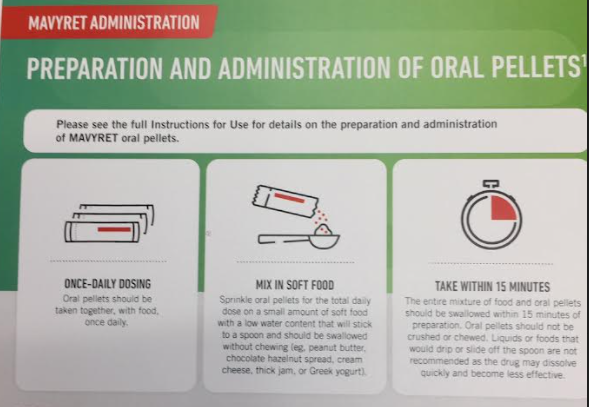
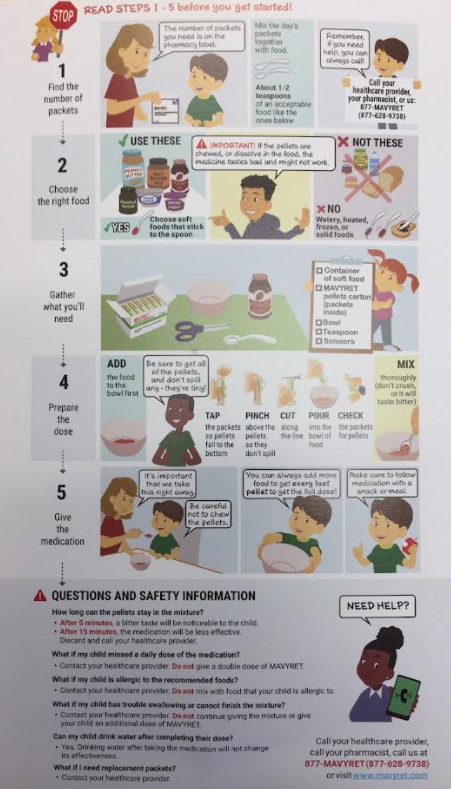
“The Food and Drug Administration (FDA) has approved Epclusa (sofosbuvir and velpatasvir) and Mavyret (glecaprevir and pibrentasvir) for treatment of chronic hepatitis C virus (HCV) infection in pediatric patients as young as 3 years. These products are the first all-oral, pan-genotypic (genotypes 1-6) HCV treatment regimens for pediatric patients 3 years and older…Both products are available as oral tablets and as newly approved oral pellets in dosing strengths suitable to accommodate the recommended weight-based dosing in pediatric patients.”
The following images are from Abbvie patient-provider handouts. I do not receive any funding from any pharmaceutical company but think these instructions are useful.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
In this retrospective study, the authors examined recurrent PSC (rPSC) in children who had undergone liver transplantation (LT) with 3 yrs of median followup. Key findings:
rPSC occurred in 36 children, representing 10% and 27% of the subjects at 2 years and 5 years following LT, respectively
Subjects with rPSC were younger at LT (12.9 vs. 16.2 years), had faster progression from PSC diagnosis to LT (2.5 vs. 4.1 years), and had higher alanine aminotransferase (112 vs. 66 IU/L) at LT (all P < 0.01)
After LT, rPSC subjects had more episodes of biopsy-proved acute rejection (mean 3 vs. 1; P < 0.001), and higher prevalence of steroid-refractory rejection (41% vs. 20%; P = 0.04)
My take: rPSC, not surprisingly, was associated with a more agressive, immunoreactive phenotype prior to LT characterized by younger age, faster progression to end-stage liver disease, higher prevalence of IBD and more frequent/difficult allograft rejection
Related blog posts:
PSC -Aspen 2021 Webinar This lecture highlights studies show lack of efficacy with vancomycin, ursodeoxycholic acid and vedolizumab. Also, there is potential utility of MMP-7 for distinguishing between PSC and AIH
This case series of 13 nondirected liver donors (ND-LLDs) (from 2012-2020) helps highlight this increasing trend of motivated donors who do not have a predetermined recipient. The Scientific Registry of Transplant Recipients documented 105 patients who underwent a living donor liver transplantation (LDLT) from ND-LLDs 2000-2019, with 39 in 2019 alone.
Key points:
While the article states that carefully selected ND-LLDs at high volume centers have excellent outcomes, the associated editorial (pg 1373-74) notes that there is a 0.2% living donor operative mortality. And, a significant number experience negative physical and socioeconomic effects of donation
The authors advocate more use of SPLIT livers to increase the donor pool (currently at 10 centers) to lower pediatric deaths on the waitlist
The authors note that the likelihood of receiving a LT is increased at high-volume pediatric centers (85%) compared to low-volume centers (41%). “Center expertise and volume is an important consideration…especially true for pediatric liver transplantation, which is relatively infrequent…551 [in 2019]” compared to 8345 adult liver transplants.
The commentary places some context regarding the donors.
70% had previously donated a kidney (“Repetitive donor disorder?”)
Yet, “in some sense, nondirected donors may be the best qualified donors, as they are free of coercion”
The authors advocate for a “safe, well-informed” process and for national guidelines to address risks and the components of evaluation, medical and psychosocial
My take: It is amazing how much some individuals are willing to sacrifice to help others, especially in age when some react so harshly to being asked to consider the needs of their community.
This study, using a rat animal model, demonstrated how gastro-resistant mixed micelles (MMs) could be used to overcome the limitations of current prophylactic vitamin K formulations which are associated with failures in newborns with unrecognized cholestatic liver diseases (1:2,500 live births).
Key findings:
Under cholestatic conditions, gastro-resistant formulations greatly improved vitamin K absorption.
Pathophysiology: “Our data provide an explanation why: unstabilized MMs will aggregate during gastric passage, once aggregated vitamin K will not be sufficiently resolubilized upon a subsequent pH increase”
My take: It is likely that these gastro-resistant MMs would be effective in pediatric patients. If proven in clinical trials, this would reduce bleeding events in infants and lower bleeding risks in those with chronic liver disease while obviating the need for parenteral Vitamin K.
There are over 130 different types of CDG with 41 that have liver involvement; 7 with a hepatopathy and 34 with in the context of multisystem disease.
Transferrin isoform analysis (Isoelectric focusing or high-performance liquid chromotography) detects about 50% of the CDGs; hence, genetic panel or exome sequencing is needed for diagnosis in many cases.
4 cases of MMF hepatoxicity are presented along with EM changes which revealed unequivocal mitochondrial abnormalities similar to those seen in primary and secondary mitochondrial disorders
MMF hepatotoxicity was confirmed in mouse study showing that MMF caused various stress changes in the mitochondria
Conclusion: Although MMF is safe for the majority of patients, MMF can cause mitochondrial stress, which may trigger more severe mitochondrial abnormalities in a small subset which can be evident with EM.
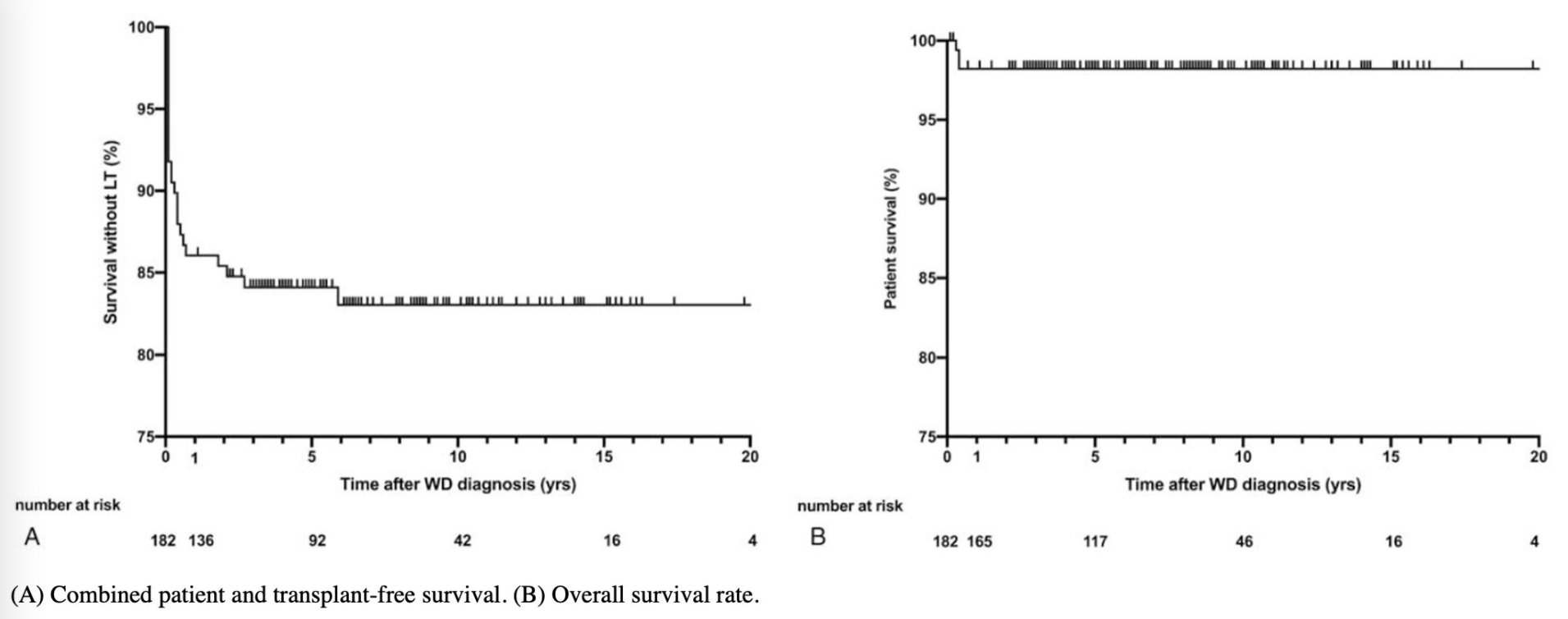
This study examined the clinical data from 182 pediatric patients. WD was diagnosed at a mean age of 10.7 years. Overall survival at 20 years of followup was 98% and patient and transplant-free survival was 84% at 20 years.