In this prospective study using the CCFA IBD Partners cohort, the authors examined fatigue symptoms with questionnaires (FACIT-F and MDI) at 3 timepoints over a 1 year period. There was likely a strong selection bias among participants (mean disease duration was 18 years) who chose to complete theses questionnaires. Key findings:
Persistent fatigue (at baseline and at 6 months) was the most common pattern, affecting two-thirds (65.8%) of patients
The strongest predictor of incident fatigue was sleep disturbance at baseline (odds ratio, 2.91.
Only 12.3% of those with fatigue at baseline had symptom resolution by 6 months. Resolution was more likely in patients with a diagnosis of ulcerative colitis, quiescent disease, and an absence of significant psychological comorbidity
My take: In those with fatigue, it is often persistent.
The authors retrospectively studied 7447 patients with dermatological conditions such as erythema nodosum (EN), pyoderma gangrenosum, Sweet’s syndrome, and aphthous stomatitis which can occur with inflammatory bowel disease (IBD) and are considered dermatological extraintestinal manifestations (D-EIMs).
Key findings:
131 (1.8%) subsequent IBD diagnoses in patients with D-EIMs compared with 65 (0.2%) in those without D-EIMs
Median time to IBD diagnosis was 205 days (IQR, 44-661 days) in those with D-EIMs
My take: The absolute risk if IBD is low in patients with D-EIMs but still increased 6-fold. This would probably be a good population to screen for IBD with a biomarker (eg. calprotectin)
J Shah et al. Inflamm Bowel Dis 2021; 27: 1832-1838. Ocular Manifestations of Inflammatory Bowel Disease Nice review: “ocular manifestations of IBD include keratopathy, episcleritis, scleritis, and uveitis and are among the most common extraintestinal manifestations.” Urgent referral to ophthalmology needed if deep eye pain that can awaken from sleep (?scleritis), if photosensitivity/blurry vision/headache (?anterior uveitis), or if floaters/decreased vision (?posterior uveitis)
This prospective cohort (2016-2018, n=417, mean age 13.7 y) examined the frequency of functional disorders (based on questionnaire) in children with celiac disease (CD) who were receiving a strict gluten free diet (GFD) for at least one year.
Key findings:
Functional abdominal pain disorders (FAPDs) had a higher prevalence s among patients with CD (11.5%) than controls (6.7%) (P < .05)
Irritable bowel syndrome (IBS) and functional constipation (FC) defined by the Rome IV criteria were more prevalent in patients with CD (7.2% for IBS and 19.9% for FC) than controls (3.2% for IBS and 10.5% for FC) (P < .05 and P < .001, respectively)
Younger age (P < .05) and a higher level of anti–transglutaminase IgA at diagnosis (P < .04) were associated with FAPDs (in particular for IBS) irrespective of GFD duration
A GFD did help with abdominal pain: After starting a GFD, 80% of children with celiac disease had resolution of stomach pain, whereas 9% started to complain of symptoms after starting a GFD
In the discussion, the authors speculate on the reasons for ongoing pain including inadvertent gluten exposure, intestinal inflammation/visceral hyperalgesia, altered microbiome, and refractory CD.
My take: Persistent stomach pain in CD is a common occurrence, even in those trying to adhere to a strict GFD.
“The AAP recommends COVID-19 vaccination for all children and adolescents 5 years of age and older who do not have contraindications using a COVID-19 vaccine authorized for use for their age.”
“Children with previous infection or disease with SARS-CoV-2 should receive COVID-19 vaccination, according to CDC guidelines.”
“Given the importance of routine vaccination and the need for rapid uptake of COVID-19 vaccines, the AAP supports coadministration of routine childhood and adolescent immunizations with COVID-19 vaccines (or vaccination in the days before or after).”
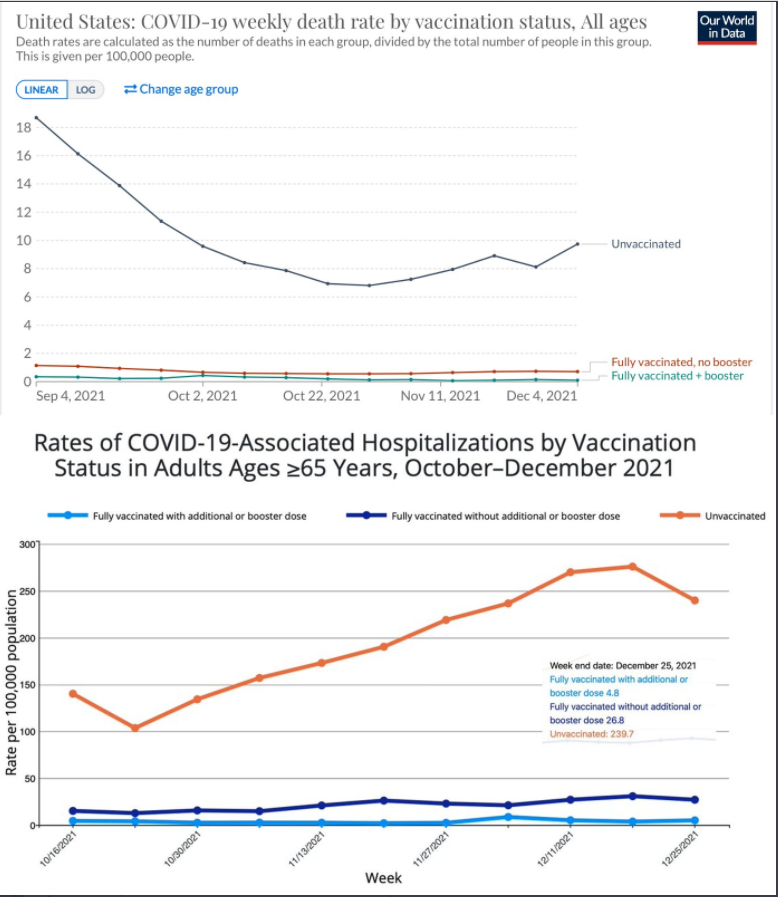
Also, more data on vaccine effectiveness from Eric Topol’s Twitter feed):
Vaccines reducing Covid deaths by 99% and hospitalizations by 98% with vaccination and a booster
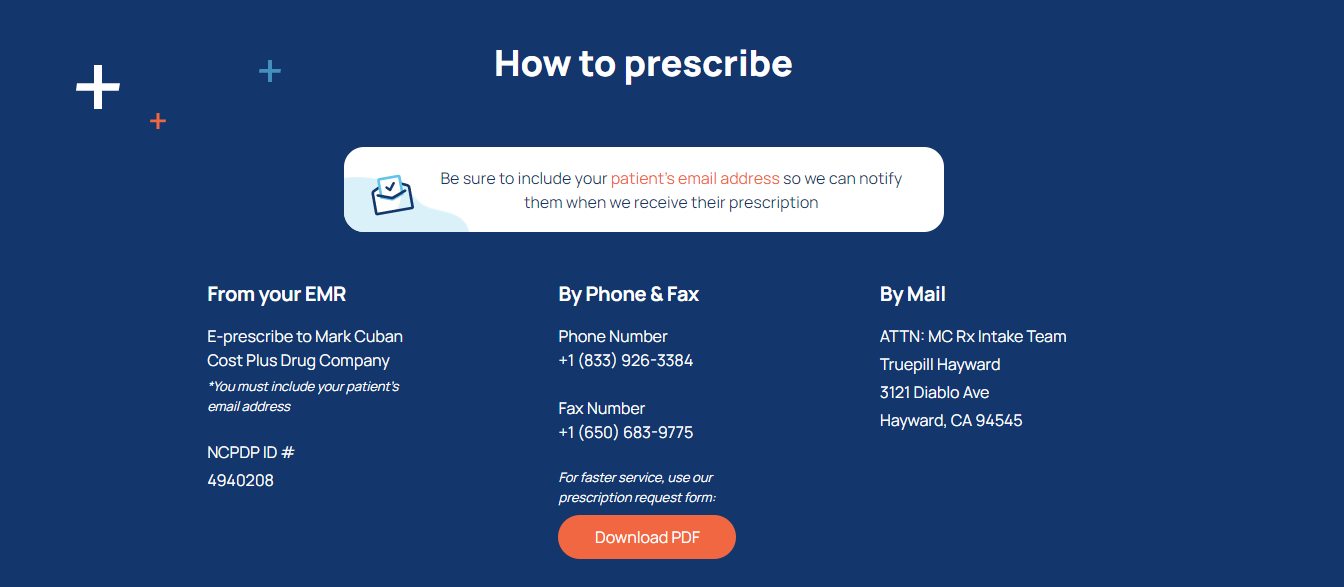
For the past few years, when someone would ask me what I would do if I were incredibly wealthy, I would say that I wanted to start a pharmaceutical company to provide reasonably-priced medications. A good example of the problems with drug pricing was discussed earlier in the week on a prior blog post regarding insulin (Insulin: “Poster Child For Everything That’s Wrong” with U.S Drug Costs). Fortunately, I no longer need to be a billionaire:
The Mark Cuban Cost Plus Drug Company announced the opening of its online pharmacy Wednesday. The pharmacy says it will bypass health care industry “middlemen” and help consumers avoid high drug prices by charging manufacturers’ prices plus a flat 15% markup and pharmacist fee…
The pharmacy doesn’t accept health insurance but says prices will still be lower than what people would typically pay at a pharmacy….
The website currently offers 100 generic drugs to treat a variety of illnesses, including diabetes, asthma and heart conditions.
One drug for diabetes patients, metformin, sells for $3.90 for a 30-day supply, compared to a retail price of $20, the pharmacy said. A 30-count of imatinib, which is used to treat leukemia and other cancers, goes for as low as $17.10 at Cuban’s pharmacy compared with $2,502.60 at other pharmacies.
Mesalamine (Generic for Canasa) $36.90 (retail $959.07)
Mesalamine (Generic for Apriso) $36.60 (retail $122.57) ***this is only for 30 pills
Methotrexate 2.5 mg (30 capsules) $13.80
Omeprazole 40 mg capsules $4.50
Pantoprazole is priced at $4.50 (40 mg tablets) (retail $71.40)
GoodRx website also has low prices on many of these medications as well; however, some of these prices at the Mark Cuban pharmacy are terrific. For example, the cost of mesalamine suppositories at GoodRx are about three times as much.
My take: I need to talk to our Epic champion to connect our EMR to this pharmacy service.
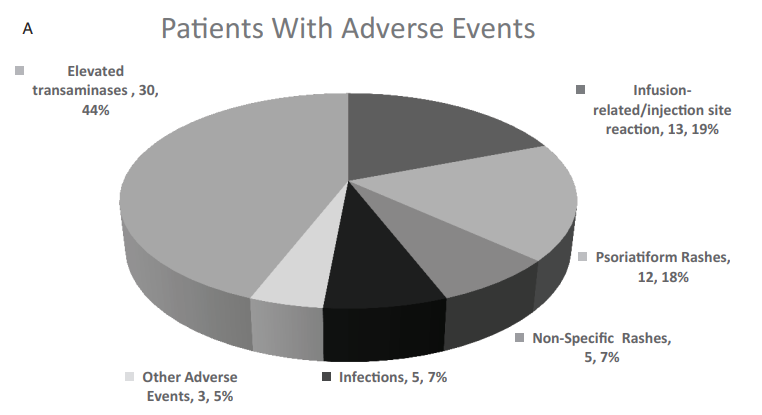
Higher trough concentrations (TCs) (>10 mcg/mL) of anti-TNFa were not associated with higher rate of anti-TNFa-related adverse events in 135 patients & >1500 TC measurements
Out of the 30 patients who presented with elevated transaminases, 27 (90%) patients had normalized transaminases values by the end of the follow-up
Adverse events were noted in 68 of 135 patients (see below)
Forty-eight studies were included in the meta-analysis comprising 6963 patients. Key findings:
Biologic therapy in IBD pregnancies was associated with a pooled prevalence of 8% for early pregnancy loss, 9% for preterm birth, 0% for stillbirth, 8% for low birth weight, and 1% for congenital malformations.
These rates are comparable with those published in the general population.
Importantly, studies with newer biologics (eg. vedolizumab, ustekinumab) had small sample sizes. In addition, ongoing prospective multicenter registries are ongoing.
Endoscopic recurrence was 46% at 2 years (median time to recurrence: 10 months).
Histologic recurrence was present in 44% in endoscopic remission
At diagnosis and surgery, over a quarter met the criteria for growth failure.. Following surgery, height, weight and BMI z scores improved significantly both at 1 year and last followup
This multicenter, retrospective observational cohort study (2014-2017) studied the outcomes of 722 adults (n=454 vedolizumab (VDZ), n=268 TNF agents (165 IFX, 103 ADA). Key findings:
VDZ-treated patients were more likely to achieve clinical remission (hazard ratio [HR], 1.651; 95% confidence interval [CI], 1.229-2.217), steroid-free clinical remission (HR, 1.828; 95% CI, 1.135-2.944), and steroid-free deep remission (HR, 2.819; 95% CI, 1.496-5.310) than those treated with TNF antagonists
Safety: Overall, there were no statistically significant differences in the risk of serious adverse events (HR, 0.899; 95% CI, 0.502-1.612) or serious infections (HR, 1.235; 95% CI, 0.608-2.511) between VDZ-treated and TNF-antagonist−treated patients.
In TNF-antagonist−naïve patients, VDZ was less likely to be associated with serious adverse events than TNF antagonists (HR, 0.192; 95% CI, 0.049-0.754). Thus, among UC patients with no prior TNF exposure, there was nearly an 80% reduction in any serious adverse event (this difference could be related, at least in part, to patient selection/disease severity)
In TNF-exposed patients, VDZ was associated with a significant increased risk for serious infections (HR, 4.295).
The authors note that the clinical remission results are similar to a previous head-to-head study of VDZ vs ADA in which VDZ had OR 1.568 for achieving clinical remission. It should be noted that the potential conflict of interest list of the 36 authors is extensive.
My take: This article supports VDZ as a first-line option for UC and strengthens the argument that it should be the first biologic for most patients with UC.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
Fortune Dec 2021-Jan 2022: Insulin’s Deadly Cost Thanks to Stan Cohen for sharing article.
Some excerpts/key points:
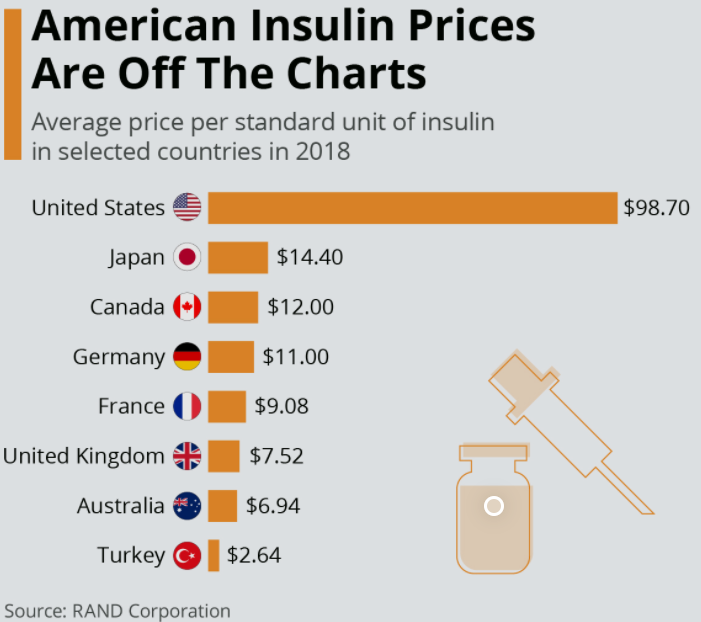
“Insulin in the U.S. costs on average some 800% more than in other developed economies. And yes, people die for lack of it, sometimes within days or even hours of missing their dose. No one knows how many; data suggests that in the U.S. it’s at least a few every day. Far more may suffer other ravages of diabetes—blindness, heart attacks, loss of limbs.” In addition, 40% of Americans who have died from COVID-19 were diabetics.
“Manufacturer’s compete not by cutting prices but by raising them.” This is often due to pharmacy benefit managers (PBMs), the middleman between manufacturer’s and insurers. PBMs negotiate drug prices and establish formularies. PBMs make more money if they able to discount higher rebates on the list cost; hence, to influence PBMs to choose their products, manufacturer’s are incentivized to raise drug costs, even if the average price is unchanged. Higher list prices affect those least able to cover the costs, namely those without insurance as well as many with high deductibles.
List price for Humalog (Eli Lilly) more than doubled from 2013 to 2018, Lantus (Sanofi) more than quadrupled from 2005 to 2016
Some patients have obtained insulin in Canada where costs for a vial could be more than 10-fold less (though this is illegal). There are also more than 12,000 GoFundMe.com listings with “insulin” in the title.
For the insulin market, some recent changes include the emergence of GLP-1 analogs for Type 2 diabetes (~90% of diabetes in U.S.). Trulicity is now Eli Lilly’s bestselling medication. In addition, the FDA recently approved Semglee, an interchangeable biosimilar for Lantus which is reducing costs.
My take: “The story of insulin is a poster child for everything that’s wrong with a free-market approach to drug availability,” says Arthur Caplan…”It’s almost inexcusable morally.”
Day-to-day, I find I am focused (?inundated) on problems that are literally right in front of me. Every once in a while, it is important to look more broadly and try to consider/address the larger issues.
Along those lines, I would recommend a series of important articles on adolescent nutrition published by The Lancet. Thanks to William Balistreri for sharing these references.
This is an introduction to the series of articles. “Given these increasingly transnational dimensions of the ultra-processed food industry, it is timely for WHO, the Food and Agriculture Organization of the UN, and their partners to revisit calls for global regulatory frameworks to assist governments in taking action. Given the speed of nutritional change, there is perhaps no greater immediate threat to the health of adolescents. Equally, tackling adolescent nutrition presents an unparalleled opportunity to interrupt intergenerational cycles of malnutrition and respond to the urgent challenges of planetary change”
The review highlights how nutrition in youth/adolescence influences weight, height, BMI as well as the timing of puberty, neurodevelopment, cardiorespiratory fitness, immune function, body composition and bone mass
Adolescents are “growing up at a time of momentous shift—ie, rapid urbanisation, climate change, food systems shifting towards foods with an increased caloric and decreased nutritional value, the COVID-19 pandemic, and growing socioeconomic inequality. The consequences of these changing contexts have profound impacts on adolescent nutrition and development”
“Adolescents have a lot to say about why they eat what they eat, and the factors that might motivate them to change. Adolescents must be active partners in shaping local and global actions that support healthy eating patterns. Efforts to improve food environments and ultimately adolescent food choice should harness widely shared adolescent values and desire for social interaction around food”
The article reviews in depth information from prior surveys including India’s Comprehensive National Nutrition Survey and the Global School-based Student Health Surveys. However, they note that nationally representative detailed dietary intake data are still scarce
Food choices by adolescents in modern communities is more heavily influenced by convenience and autonomy; in more traditional communities, family and community priorities often supersede individual considerations of adolescents
In the setting of the pandemic, more families (worldwide) are being pushed into food insecurity and shifting towards lower-cost, less nutritious non-perishable foods.
“Even in less food-insecure contexts, social isolation is resulting in negative trends among some adolescents, such as reported weight gain, poor eating habits, and stress eating”
“Adolescence (10–24 years of age) is “characterised by transition, exploration, and openness to change [good and bad], offering opportunities for radical shifts in diet, physical activity, and other risks for non-communicable diseases. This same novelty-seeking and openness to change also makes adolescents a vulnerable group to commercial exploitation and other unhealthy influences, with lifelong and intergenerational consequences”
“Despite micronutrient deficiencies and food insecurity persisting in many places, and overweight and obesity rapidly increasing, adolescents have been largely overlooked in global nutritional policy frameworks. Targets should be established for adolescent nutrition in its global tracking and accountability mechanism”
“Greater government fiscal and policy action to both restrict the availability of highly processed foods and enhance healthy and diverse adolescent diets is urgently needed”
Nutrition education needs to be leveraged in schools: “knowledge of dietary diversity, food environment, and practical skills; use opportunity of school curricula to support nutrition and food preparation; improving choice architecture”
Social media has become a huge influence on dietary choices, body image, and psychological well being, both through advertising and marketing to adolescents and subsequent peer interactions
My take: If we truly hope to improve population health, improving diet choices cannot remain the province of only the well-educated wealthy. Adolescence offers a chance to change health trajectories before habits are more rigid and before the development of fixed health consequences.
This study utilized the Swedish nationwide health registry (2002-2017; n = 5767 with IBD) and controls from the general population (n= 58,418). One reason for this study is the increased frequency and changing patterns of immunosuppressive medications that are being used in pediatric IBD. Key findings:
672 serious infections (38.6/1000 person-years) occurred among the children with IBD compared with 778 serious infections in the control group (4.0/1000 person years; adjusted HR 9.46 ). HRs were increased for children with ulcerative colitis 8.48, Crohn’s disease 9.30, and IBD unclassified 12.1
Particularly high HRs were also seen in the first year of diagnosis with HR of 12.1 and n children with IBD undergoing surgery, HR 17.1. This 17-fold risk translates to an average of 6 per 100 children having a serious infection among those with operations.
340 of the 672 serious infections were gastrointestinal, including 34 due to Clostridium difficile
20 opportunistic infections were identified during 19,000 person-years
Potential risk factors for infection, besides medications, include malnutrition, chronic inflammation, impaired response to vaccination, and dysregulation of immune responses. A limitation of this study is ascertainment bias as families/patients with underlying disease may be more likely to seek medical attention for otherwise self-limited infections.
My take: This report confirms and quantitates daily clinical practice: children with IBD are more frequently hospitalized due to infections.