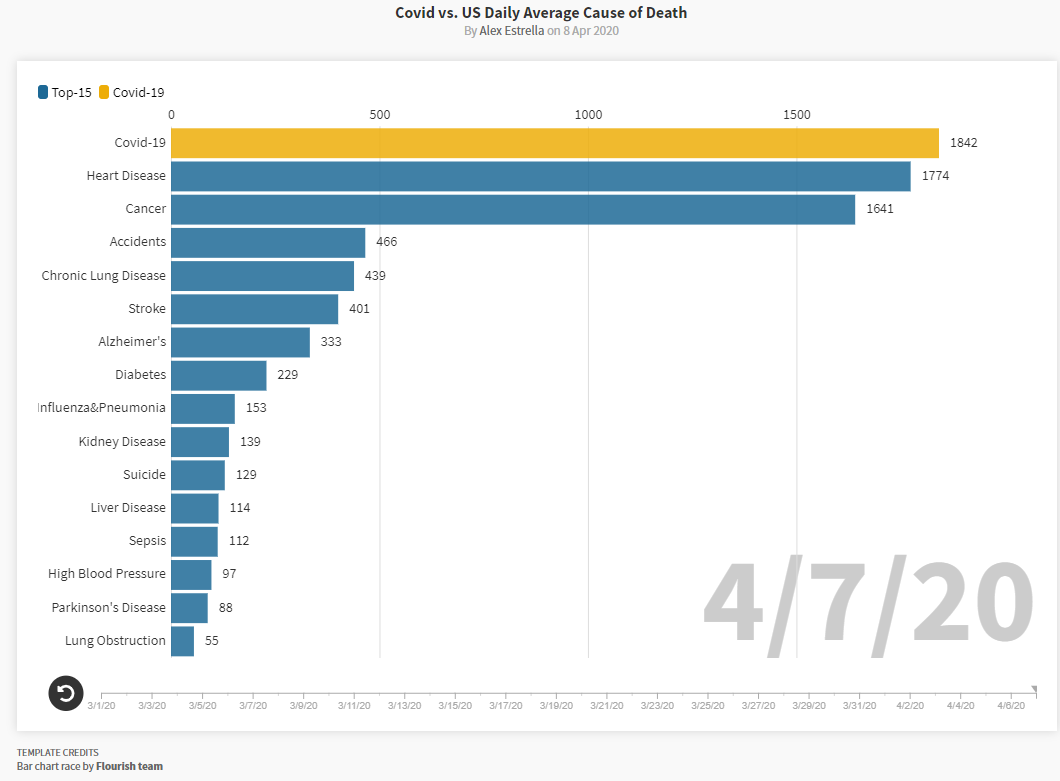
YouTube Video –Adley.TV: What We Should ALL Be Doing Right Now (COVID-19 Humor)
——————-
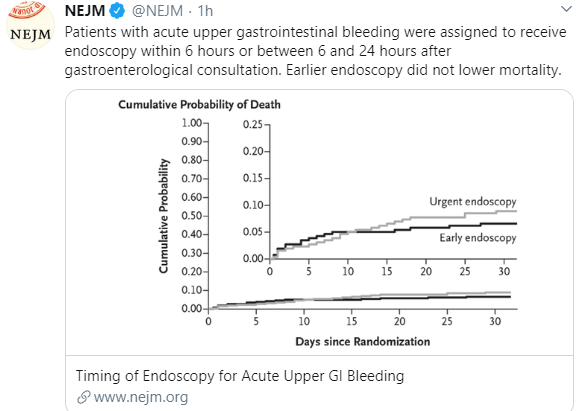
A recent study (JYW Lau et al. NEJM 2020; 382: 1299-1308, editorial by L Laine 1361-2) indicates that performing an upper endoscopy within the first 6 hours of presentation to the hospital is NOT associated with better outcomes.
516 patients who were predicted to be at high risk for further bleeding or death were randomly assigned to undergo endoscopy within 6 hours or between 6-24 hours. Key findings:
- 30-day mortality: 8.9% in the <6 hr group (<6G) compared to 6.6% in the 6-24 hr group (6-24G)
- Endoscopic treatment was administered to 60.1% of <6G compared to 48.4% in 6-24G
- Re-bleeding within 30 days in 10.9% of <6G compared to 7.8% in 6-24G
The editorial notes that guidelines recommend endoscopy be performed within 24 hours following hemodynamic resuscitation and attention to other coexisting conditions before endoscopy.
My take: This is good news for endoscopists -no need to rush to the endoscopy suite/operating room in the middle of the night!
Link NEJM: Two minute quick take on article
Related blog posts:
- #NASPGHAN19 Postgraduate Course (Part 1) | gutsandgrowth
- All bleeding stops (part 2)
- Hemospray for GI Bleeding
- Is a Continuous IV Proton Pump Inhibitor Really Necessary for GI Bleeders?
- How Many Times Have You Done This? | gutsandgrowth
- All bleeding stops | gutsandgrowth
- NASPGHAN Postgraduate Course 2014 -Endoscopy… | gutsandgrowth
- Watch the Bleeding Ulcer Stop! | gutsandgrowth
- Transfusion strategy in acute GI bleeding | gutsandgrowth