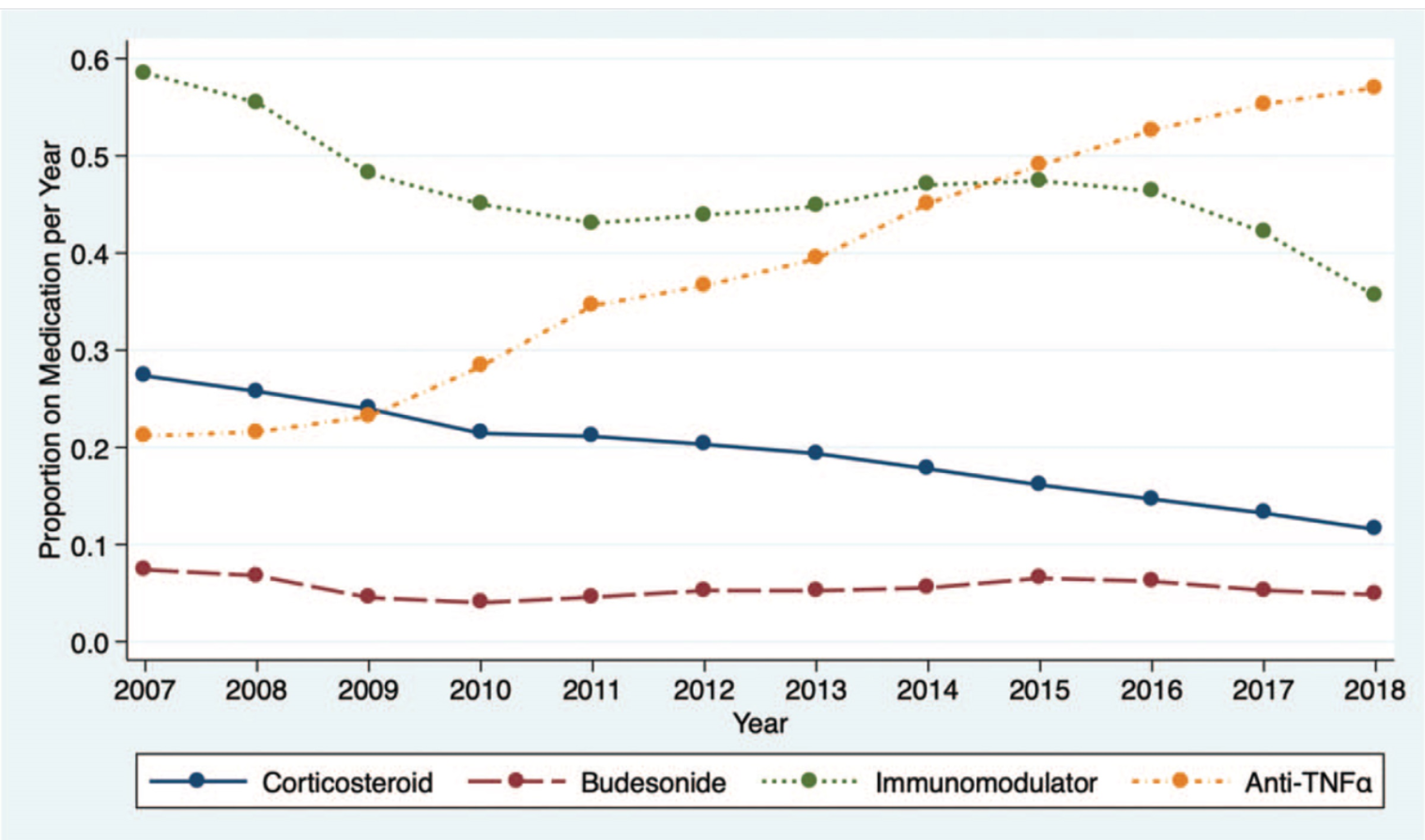
In this study of 27,321 patients enrolled in the ImproveCareNow (ICN) learning health system, key findings:
Corticosteroid use decreased from 28% (2007) to 12% (2018)
Black patients received corticosteroids more commonly than white patients. This disparity improved as corticosteroid use decreased in both groups
Anti-tumor necrosis factor-alpha medication use <120 days after diagnosis was associated with a reduction in corticosteroid use
As corticosteroid use decreased, steroid-sparing therapy use increased and height and weight z scores improved, particularly among children with Crohn disease
27 centers (31%) had a significant reduction in steroid use, 5 (6%) had a significant increase, and 45 (52%) had variability in steroid use. 9 centers (11%) had <2 years of data.
My take: These findings are expected but nice to see. Patients in the ICN are using less steroids and growing better. Given the variation in care among centers, there is more work needed.
The panel agreed that reactive TDM should be used for all biologics for both primary nonresponse and secondary loss of response
It was recommended that treatment discontinuation should not be considered for infliximab or adalimumab until a drug concentration of at least 10–15 mg/mL was achieved
Consensus was also achieved regarding the utility of proactive TDM for anti–tumor necrosis factor therapy. It was recommended to perform proactive TDM after induction and at least once during maintenance.
More data are needed with regard to proactive TDM for biologics other than anti-TNF agents
There are no differences in interpreting TDM between originator biologics and biosimilars
When considering switching within drug class in case of secondary loss of response to a first anti-TNF drug because of the development of antidrug antibodies, an immunomodulator should be added to a subsequent anti-TNF therapy
Low-titer antidrug antibodies can be overcome by treatment optimization (dose escalation, dose interval shortening, and/or addition of an immunomodulator)
My take: This article should help support the practice of proactive TDM and discourage stopping anti-TNF agents until an adequate therapeutic level is achieved.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
A recent study (MT Dolinger et al. Inflamm Bowel Dis 2021; 27: 1210-1214) and the associated editorial (D Geem, S Kugathasan. Inflamm Bowel Dis 2021; 27: 1361-1362) describe the use of multiple therapies (biologics and small molecule therapy) to target refractory pediatric inflammatory bowel disease. Since the term “combination therapy” is already in broad use for those receiving a biologic agent and an immunomodulator, I plan to refer to these new combinations as ‘dual immunotherapy’ for IBD.
Dolinger et al (Dual Biologic and Small Molecule Therapy for the Treatment of Refractory Pediatric Inflammatory Bowel Disease) described 16 children with dual immunotherapy. Nine (56%) were treated with vedolizumab/tofacitinib, 4 (25%) with ustekinumab/vedolizumab, and 3 (19%) with ustekinumab/tofacitinib. Twelve (75%; 7 ulcerative colitis/IBD-unspecified, 5 Crohn’s disease ) achieved steroid-free remission at 6 months. One patient on 30 mg of vedolizumab/tofacitinib and prednisone daily developed septic arthritis and a deep vein thrombosis.
Except for “anti-TNF medications (infliximab and adalimumab), no other biologic therapies are FDA-approved for children with IBD”
“Clinical disease remission is achieved in only 40-60% of patients on anti-TNF medications”
With ustekinumab, “limited pediatric data reveal that in patients who have failed at least 1 biologic therapy, 38.6-58% achieve clinical remission by week 52…[And] vedolizumab …demonstrated steroid-free remission in 20% by week 22 in a single-center prospective observational cohort study.”
The response to dual immunotherapy is most likely due to the synergistic effects of two medications rather than the start of a new medication. The authors note a prior study which showed a positive experience of adding ustekinumab in 5 children who developed severe paradoxical psoriasis with infliximab and in another subset of pediatric patients, there was improvement with combination vedolizumab/infliximab (Paediatr Drugs 2020; 22: 409-416)
My take (borrowed from editorial): “Given the phenotypic heterogeneity of pediatric IBD and the multiple inflammatory immune pathways implicated in its pathogenesis, the approach of biologic monotherapy–may not be suitable for all patients…patients may require specific combinations…to quell multiple arms of their dysregulated immune response.” More trials are needed to determine the safety of these regimens (especially with regard to malignancy and infections).
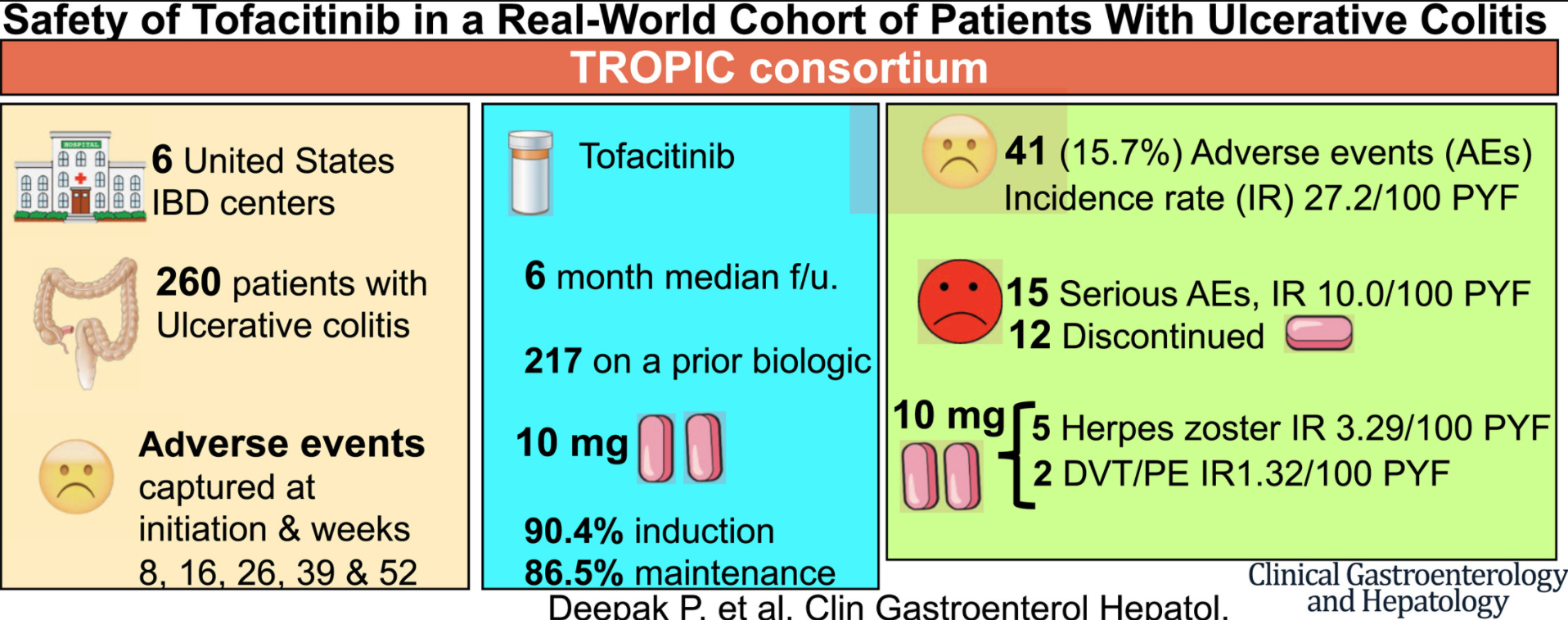
This study described a ‘real-world’ experience with tofacitinib for Ulcerative Colitis in 260 adults; five patients developed HZ infection and 2 developed VTE (all receiving 10 mg tofacitinib, twice per day).
Methods: Patients with CD after ileocolonic resection with ileocolonic anastomosis were assigned randomly to groups given weekly 25,000 IU oral vitamin D (n = 72) or placebo (n = 71) for 26 weeks, at 17 hospitals in The Netherlands and Belgium, from February 2014 through June 2017
Key finding: The cumulative rate of clinical recurrence did not differ significantly between the groups (18.1% in the vitamin D group vs 18.3% in the placebo group; P = .91). Though, the Vit D group achieved higher levels at week 26 (81 vs 43 of 25-OH Vit D)
In an observational prospective longitudinal study of with newly diagnosed Crohn’s disease in 156 adults followed for nearly 1.5 years, Yanai et al found that 52 patients (33.3%) had an indolent course of CD, 29 (18.5%) required hospitalizations, and 75 (48%) were recommended to start steroid, immunomodulator, or biologic therapies. An “indolent course” indicated a lack of needing steroids, immunomodulators, anti-TNF agents, hospitalization or surgery. Key findings:
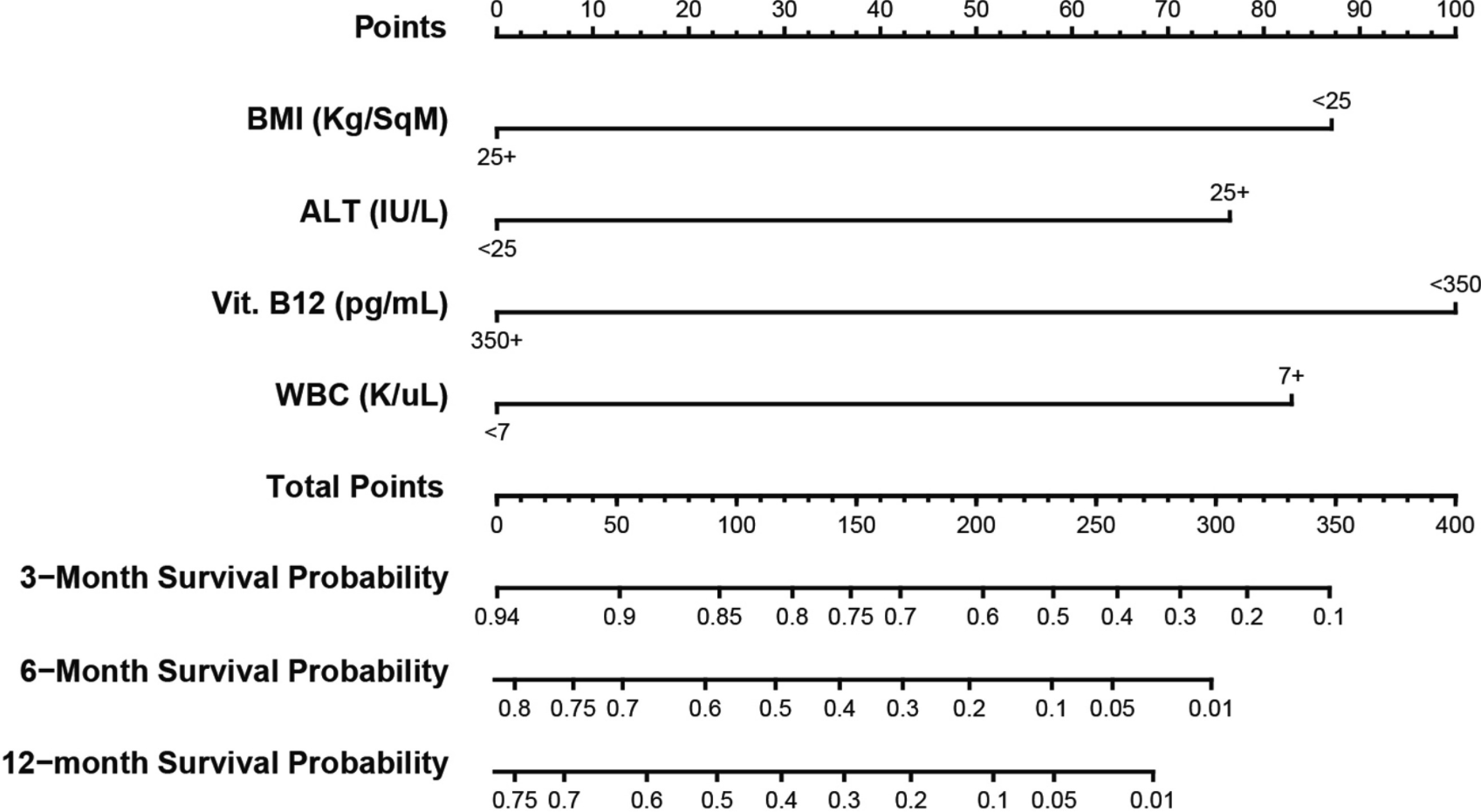
There were 4 factors associated with complicated course in treatment-naïve patients: body mass index <25 kg/m2 (hazard ratio [HR], 2.45; 95% CI, 1.07–5.43; P = .033), serum level of vitamin B12 <350 pg/mL (HR, 2.78; 95% CI, 1.21–6.41; P = .016), white blood cells ≥7 × 103/μL (HR, 2.419; 95% CI, 1.026–5.703; P = .044), and serum level of ALT ≥25 IU/L (HR, 2.680; 95% CI, 1.186–6.058; P = .018).
This model discriminated between patients with vs without a complicated course of disease with 90% and 89% accuracy at 6 and 12 months after diagnosis, respectively. A validation cohort demonstrated a discriminatory ability of 79% at 3 months after diagnosis, and a nomogram was constructed (see below)
Points on the nomogram are based on: BMI <25 kg/m2 = 87 or ≥25 kg/m2 = 0, WBC <7 × 103/μL = 0 or ≥7 × 103/μL = 83, vitamin B12 <350 pg/mL = 100 or ≥350 pg/mL = 0, and ALT <25 IU/L = 0 or ≥25 IU/L = 76. The sum score for all variables corresponds with the probability of having an indolent course of disease at different time points after diagnosis.
My take: In this study, low BMI, low Vit B12, high wbc, and high ALT were associated with a more complicated course. These particularly risk factors do not seem intuitive to me. These findings need to be looked at in the pediatric age group, which likely has a lower rate of an indolent course.
In this retrospective study of 270 consecutive adult patients with acute severe ulcerative colitis (ASUC) (2002-2017), the cumulative risk of colectomy was 12.3% (95% CI, 8.6–16.8). Key findings:
Based on multivariate analysis, previous treatment with TNF antagonists or thiopurines (hazard ratio [HR], 3.86), Clostridioides difficile infection (HR, 3.73), serum level of C-reactive proteinabove 3.0 mg/dL (HR, 3.06), and serum level of albumin below 3.0 g/dL (HR, 2.67) were associated with increased risk of colectomy
The cumulative risks of colectomy within 1 y in patients with scores of 0, 1, 2, 3, or 4 were 0.0%, 9.4% (95% CI, 4.3%–16.7%), 10.6% (95% CI, 5.6%–17.4%), 51.2% (95% CI, 26.6%–71.3%), and 100%. Negative predictive values ranged from 87% (95% CI, 82%–91%) to 92% (95% CI, 88%–95.0%). Findings from the validation cohort were consistent with findings from the derivation cohort.
My take: These findings confirm other studies in patients with ulcerative colitis which have shown that each of these criteria were predictors of severe disease.
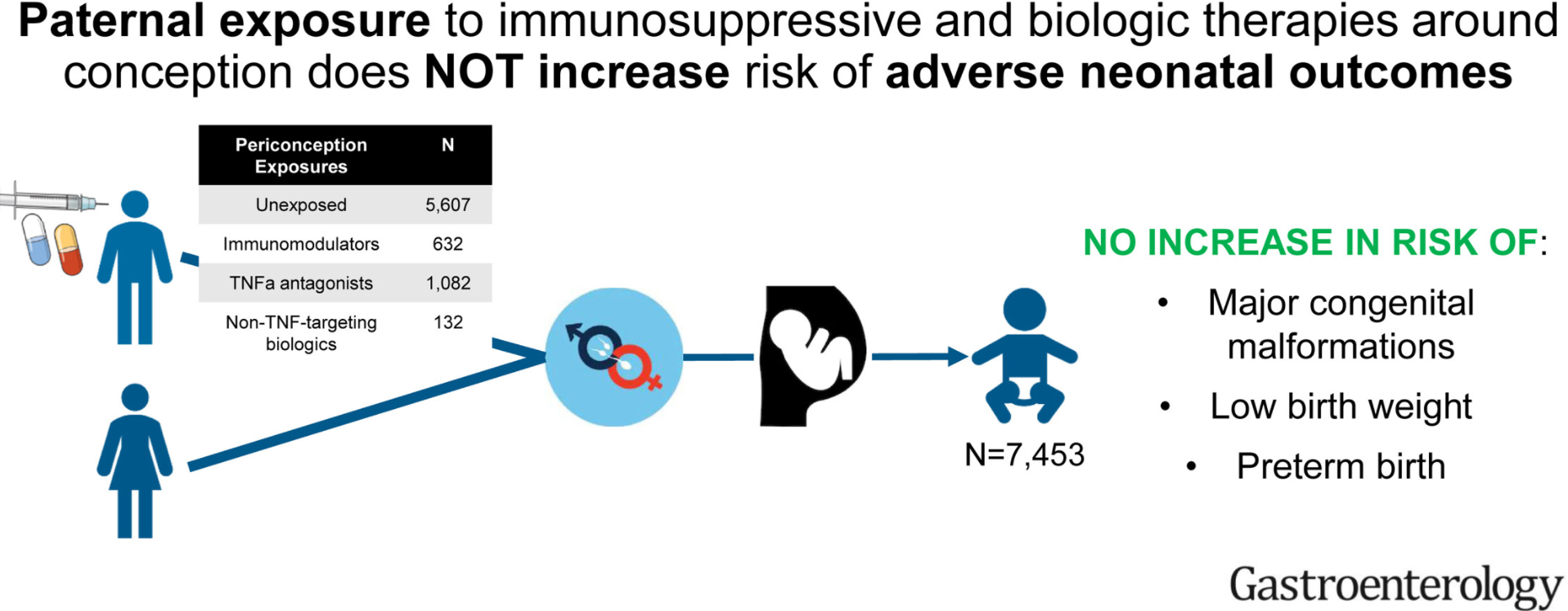
Methods: The investigators used a deidentified administrative claims database (OptumLabs Data Warehouse) with a total of 7453 expectant fathers with immune-mediated diseases.
Key findings:
As compared to unexposed fathers (3.4% prevalence of major congenital malformations), exposure to immunosuppressives/biologics were not associated with increased risk of major congenital malformations: thiopurines (relative risk [RR], 1.12; 95% confidence interval [CI], 0.66–1.76), methotrexate (RR, 0.67; 95% CI, 0.21–1.55), TNF-α antagonists (RR, 1.14; 95% CI, 0.81-1.57), and non–TNF-targeting biologic agents (RR, 1.75; 95% CI, 0.80–3.24).
No association was observed between paternal medication exposure and risk of preterm birth or low birth weight.
“Regarding major congenital malformations, we believe that the results should be interpreted with caution. The numbers of these outcomes are relatively low and the statistical precision of the risk estimates should be taken into consideration.”
My take: Overall, this study is reassuring. Though it is difficult to prove these medications do not have impacts on newborns, if these effects were frequent, it would likely be evident in this type of study.
Using a selected sample from a database with >62 million patients, this retrospective cohort study determined the rates of colorectal cancer among patients with IBD. Key finding:
Among the IBD cohort, patients treated with anti-TNF agents were less likely to develop CRC; patients with Crohn’s disease: odds ratio, 0.69; 95% confidence interval, 0.66-0.73; P < 0.0001 vs patients with ulcerative colitis: odds ratio, 0.78; 95% confidence interval, 0.73-0.83; P < 0.0001.
My take: This study found an association between anti-TNF therapy and a reduced risk of CRC in patients with IBD.
Using the National Health Interview survey (2015), the authors identified individuals with self-reported IBD and assessed national estimates of financial toxicity. Key findings:
23% reported financial hardships due to medical bills, 16% of patients reported cost-related medication nonadherence, and 31% reported cost-reducing behaviors
Approximately 62% of patients reported personal and/or health-related financial distress, and 10% of patients deemed health care unaffordable
Inflammatory bowel disease was associated with 1.6 to 2.6 times higher odds of financial toxicity across domains compared with patients without IBD
My take: In addition to the physical and emotional toll of having IBD, there is also significant financial hardships for many.
This reported case series with 5 patients with severe ulcerative colitis (UC) who received a combination of tofacitinib and infliximab for at least 90 days were retrospectively reviewed. Tofacitinib dosing was de-escalated to 5 mg twice daily after 8 weeks. Thiopurine therapy was stopped with tofacitinib initiation.
Key findings:
Median duration of combination therapy was 9 months (range, 4–12 months). At 90 days, all patients had a reduction in Mayo score of ≥3. Four patients improved clinically and biochemically (Table 1), with 3 patients achieving steroid-free remission.
The only adverse event reported was one patient developing varicella zoster.
The authors letter title regarding tofacitinib being “safe and effective” is clearly overstated. The reply notes that in limited experience the group from the University of Michigan had a 50-year-old man develop severe pulmonary and CNS disease due to acquisition of legionnaires disease while on combination tofacitinib and infliximab.
My take: (borrowed from reply) “Efficacy and safety data obtained through rigorous randomized trials are needed…it is possible that long-term use of combination tofacitinib and infliximab will lead to an unacceptable risk of infection.”
Another study of tofacitinib: GR Lichtenstein et al. Inflamm Bowel Dis 2021; 27: 816-825. Tofacitinib, an Oral Janus Kinase Inhibitor: Analysis of Malignancy (Excluding Nonmelanoma Skin Cancer) Events Across the Ulcerative Colitis Clinical Program Key finding: With an exposure of 2576.4 patient years & 124 overall cohort tofacitinib-treated patients, 20 developed a malignancy
Methods: The UC San Diego IBD Biobank was used to prospectively collect 332 stool samples (every 6 months) from 129 subjects (50 ulcerative colitis; 79 Crohn’s disease). Of these, 21 with Crohn’s disease had ileocolonic resections, and 17 had colectomies.
Key finding: Intestinal surgeries in IBD patients seem to reduce the diversity of the gut microbiome and metabolome in IBD patients. Colectomy has a larger effect than ileocolonic resection.
Limitations: Confounding variables (eg. antibiotics) and selection bias (patients with more severe disease
34,644 newly diagnosed patients with IBD (CD = 59.5%)
The probability of first and second hospitalizations remained unchanged in Québec and the probability of major surgery was low overall but did increase despite the higher and earlier use of anti-TNFs. However, the authors note that “in the present study, biologics use under the public reimbursement plan was 13% in patients with UC and 16% in patients with CD.”
My take: This study is provocative but probably misleading; it is quite likely that use of anti-TNF agents do lower the risk of hospitalization and surgery.
Methods: The authors used the Mount Sinai BioMe Biobank, which contains genetic data on 32,595 patients. After rigorous phenotype validation, 19,541 individuals were retained, of whom 339 were IBD patients (273 CD, 28 UC, and 37 individuals who were classified as both) and 19,202 were controls
Key findings: In this study, the authors identified several rare VEO-IBD variants with high genetic penetrance using the biobank samples and then replicated results in large case control African American and European data sets.
One of the variants with the highest genetic penetrance located in the gene LRBA was predicted to result in a deleterious change to the amino acid structure. Reduced expression of CTLA-4 secondary to the variants we identified in LRBA may result in autoinflammation that contributes to IBD. “Targeting reduced CTLA-4 expression is an exciting treatment venue, because expression of CTLA-4 has been shown to be increased by chloroquine treatment in vitro.”
Enteropathy is present in 63% of all known individuals with LRBA deficiency, with 27% having chronic diarrhea as the presenting symptom
Mangroves in John Pennekamp State Park (Key Largo)
As noted in previous blog posts (see below), adult guidelines for ulcerative colitis favor ustekinumab over vedolizumab for ulcerative colitis patients who have had anti-TNF therapy; recent pediatric guidelines appeared to do the opposite, possibly due to limited data with ustekinumab.
All patients had failed prior infliximab therapy, and 12 (48%) also had failed vedolizumab. Five patients discontinued ustekinumab after IV induction (four undergoing colectomy).
On intent to treat basis, 44% (n=11) achieved the primary endpoint of steroid‐free remission at week 52, including nine (69%) of 13 who previously treated with anti‐TNF only vs two (17%) of 12 who previously failed also by vedolizumab. Seven of 11 remitters met the criteria for endoscopic improvement.
Higher trough levels were not associated with a superior rate of clinical remission; the median (IQR) trough levels (μg/mL) were greater with q4 vs q8 weekly dosing (8.7 [4.6‐9.9] vs 3.8 [12.7‐4.8]) P = 0.02.
No adverse events were associated with therapy.
My take: Ustekinumab is a good option for pediatric patients with ulcerative colitis who are refractory to anti-TNF agents. More data are needed to help in positioning therapies.
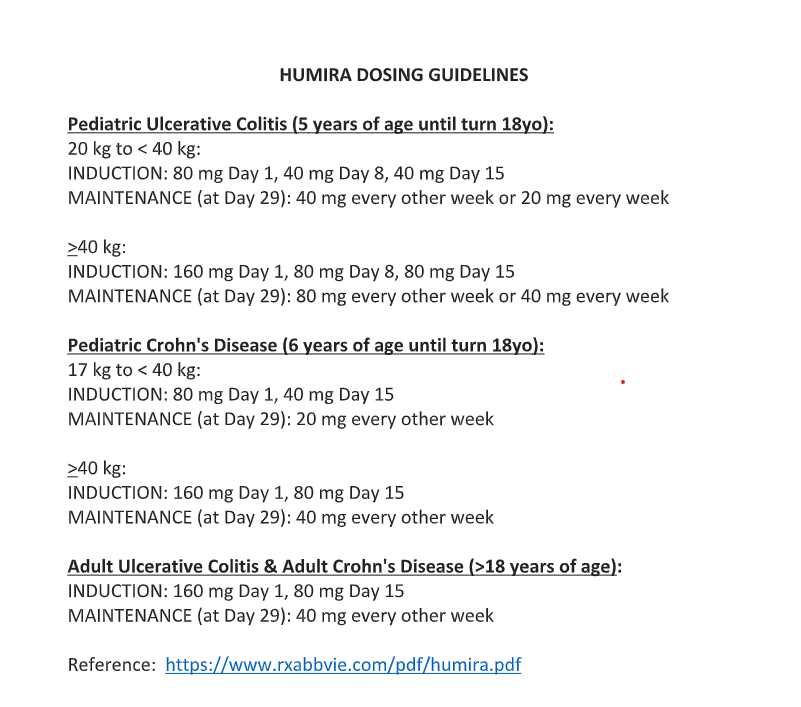
Also, Humira (adalimumab) is now FDA-approved for children as young as 5 years with ulcerative colitis: FDA Approves Adalimumab as Treatment for Children With Ulcerative Colitis (2/25/21). “This approval is based on results from the phase 3, randomized, double-blind, multicenter ENVISION I (NCT02065557) study.” Abbvie has now updated their Humira dosing recommendations (Reference: https://www.rxabbvie.com/pdf/humira.pdf). Thanks to Clair Talmadge for this update.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.