AM Jastreboff et al. NEJM 2023; DOI: 10.1056/NEJMoa2301972. Triple–Hormone-Receptor Agonist Retatrutide for Obesity — A Phase 2 Trial.
Background: Retatrutide (LY3437943) is an agonist of the glucose-dependent insulinotropic polypeptide, glucagon-like peptide 1, and glucagon receptors.
Methods: This study enrolled 338 with BMI of at least 27 in a a phase 2, double-blind, randomized, placebo-controlled trial with once-weekly injections of retatrutide.
Key Findings:
The number who achieved at least a 10% weight loss:
“The safety profile of retatrutide was consistent with reported phase 1 findings in persons with type 2 diabetes13 and similar to those of therapies based on GLP-1 or GIP–GLP-1 for the treatment of type 2 diabetes or obesity”
My take: There are a number of effective agents for obesity that have been developed very recently. Long term efficacy and safety are still not well-understood.
In previous posts, this blog (see below) has examined the potential bias of studies reporting better outcomes in breastfed infants along with issues of maternal guilt. A recent commentary explores the issue of feeling guilty when breastfeeding does not go well.
AJ Kennedy. NEJM 2023; 388:1447-1449. Breast or Bottle — The Illusion of Choice
Some excerpts:
Only about 25% of women in the United States exclusively breast-feed for the recommended period.2 After my struggles, these statistics seem realistic to me, but before I went through it myself, I had no concept of how hard it could be…
Around the time my son turned 6 months old…my primary care doctor… gave me the courage to start taking medication and to stop breast-feeding that very week. Though the guilt about stopping has never fully gone away, the joy and happiness in my life quickly returned…
Even after I’ve told them that I might not choose to breast-feed this time around [with 2nd child], multiple doctors have “reminded” me that breast milk has been shown to carry Covid-19 antibodies — yet another reason to feel ashamed if I choose not to breast-feed…I am hopeful that this time around I can embrace formula feeding more quickly if that is the path that works best for me and my baby,…
I encourage the AAP and other national health organizations to consider how their statements on exclusive breast-feeding are perceived by the public. If 75% of us are not meeting this goal [6 months of exclusive breastfeeding], a more patient-centered approach and recommendation is needed.
My take: Breastfeeding does not work for everyone. Parents often feel guilty about perceived short-comings and we need to find a balance in encouraging breastfeeding but acknowledging that formula feeding is a good alternative.
Related blog posts:
Feeling Guilty about Stopping Breastfeeding?Geoff Der, a statistician at the University of Glasgow who has worked with the same data in previous studies, said that the findings in the present study were robust and the authors’ method for eliminating selection bias was powerful…“In a society with a clean water supply and modern formulas,” he said, “a woman who isn’t able to breast-feed shouldn’t be feeling guilty, and the likelihood that there’s any harm to the baby is pretty slim.”
Key finding: In this cluster randomized controlled trial (n=181, ages 6-10 years), screen media reduction in the treatment group resulted in an increase of 45.8 minutes per day of physical activity compare to the usual routine group.
Using a database with 10,777 pediatric patients (2007-2018) with more than 28,000 patient years, there were 5 lymphomas reported. 4 had received thiopurines and none received anti-TNF monotherapy.
My take: This is a very reassuring study for the safety of anti-TNF agents.
In this retrospective study with 92 patients (182 colonoscopies), the authors found “minimal variability between degree of inflammation among biopsy fragments within and among different colorectal segments in UC, suggesting that even a single biopsy would adequately reflect the inflammation of the entire colorectum.”
My take: This study suggests that taking biopsies from every segment of the colon (when it looks uniform) is usually not needed, unless the purpose is to look for dysplasia. Also, it is worth recognizing that individuals with primary sclerosing cholangitis often have greater histologic activity in the right colon.
JPH Wilding et al. Diabetes, Obesity and Metabolism 2022. https://doi.org/10.1111/dom.14725 Open access! Weight regain and cardiometabolic effects after withdrawal of semaglutide: The STEP 1 trial extension “One year after withdrawal of once-weekly subcutaneous semaglutide 2.4 mg and lifestyle intervention, participants regained two-thirds of their prior weight loss, with similar changes in cardiometabolic variables. Findings confirm the chronicity of obesity and suggest ongoing treatment is required to maintain improvements in weight and health.”
This article discusses several conditions like Prader-Willi and pregnancy that can result in increase hunger and then elaborates on genetic tendency towards obesity in an age of abundant ultra-processed high calorie foods. Excerpts:
A famous 1990 study of identical twins born in Sweden showed that pairs who were separated at birth and adopted had weights more similar to each other than to their adoptive families…The ability to sense such fullness — and hunger — varies, the result of genetic differences in brain circuits that control appetite.
The new drugs are the first to manipulate the hormonal regulatory systems governing energy balance. The drugs simulate the action of our native GLP-1 but with longer-lasting effects, amplifying the fullness signal inside the body…At the very least, though, the way the drugs work can teach us that people who are larger did not necessarily choose to be, just as people who are smaller did not — and are not morally superior. This “isn’t a free pass, either to individuals who do have the capacity to choose better, nor does it take the heat off of food industries,” said a University of Sydney nutritional biologist, Stephen Simpson, but it’s “evidence that obesity isn’t a personal lifestyle choice.”
My take: For those who benefit from GLP-1 medications, it is important to recognize that weight gain is likely when the medications are discontinued; this indicates once treatment is started, the goal would be to use indefinitely –until something better comes along.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition
Anyone who follows this blog closely knows my inherent attraction for study acronyms; it is too bad I am not a leading researcher because it would be really fun to come up with some hilarious acronyms.
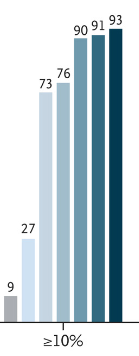
The Primary Obesity Surgery Endoluminal (POSE) Procedure for the treatment of obesity (GL Nava et al. Clin Gastroenterol Hepatol 2023; 21: 81-89) prospectively enrolled 44 adult patients who underwent “a novel pattern of full-thickness gastric body plications to shorten and narrow the stomach using durable suture anchor pairs.”
Key findings:
This procedure used an average of 19 suture anchor pairs, with a mean duration of 37 ± 11 minutes, and was technically successful in all subjects
Mean percentage total body weight loss (%TBWL) at 12 months was 15.7% ± 6.8%. >15% TBWL was achieved by 58%
Improvements in lipid profile, liver biochemistries, and hepatic steatosis were seen at 6 months
Repeat assessment at 24 months (n = 26) showed fully intact plications. No serious adverse events occurred
My take: This study shows that endoscopic therapies for obesity are quite promising. However, endoscopic therapies and bariatric surgery may become 2nd or 3rd line therapies if oral medications are available that can achieve similar success. Though, medications could require indefinite treatment.
Thank you to those who have helped me this past year with this blog –colleagues, friends and family. Wishing all of you a good 2023. Here are some of my favorite posts from this past year:
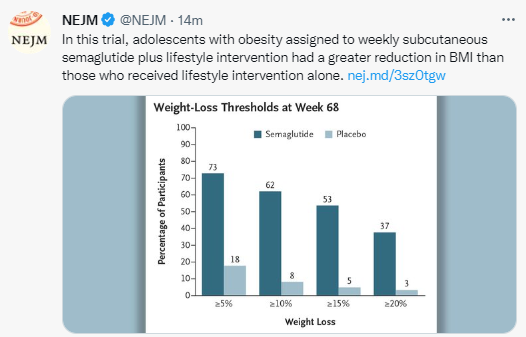
D Weghuber et al NEJM 2022; DOI: 10.1056/NEJMoa2208601. Once-Weekly Semaglutide in Adolescents with Obesity
Methods: In this double-blind, parallel-group, randomized, placebo-controlled trial, we enrolled 201 adolescents (12 to <18 years of age) with obesity (a body-mass index [BMI] in the 95th percentile or higher) or with overweight (a BMI in the 85th percentile or higher) and at least one weight-related coexisting condition. 180 (90%) completed treatment. Participants were randomly assigned in a 2:1 ratio to receive once-weekly subcutaneous semaglutide (at a dose of 2.4 mg) or placebo for 68 weeks, plus lifestyle intervention.
Key findings:
The mean change in BMI from baseline to week 68 was −16.1% with semaglutide and 0.6% with placebo
At week 68, a total of 95 of 131 participants (73%) in the semaglutide group had weight loss of 5% or more, as compared with 11 of 62 participants (18%) in the placebo group
Improvement with respect to cardiometabolic risk factors (waist circumference and levels of glycated hemoglobin, lipids [except high-density lipoprotein cholesterol], and alanine aminotransferase) were greater with semaglutide than with placebo
“The safety of semaglutide in this adolescent population appeared to be consistent with findings among adults with overweight or obesity… Gastrointestinal disorders (primarily nausea, vomiting, and diarrhea) were the most frequent adverse events with semaglutide (occurring in 62% of participants, as compared with 42% in the placebo group) and were generally mild or moderate in severity and of short duration (median duration, 2 to 3 days for nausea, vomiting, and diarrhea in the semaglutide group)”
“Permanent discontinuations because of gastrointestinal disorders were very low. Furthermore, semaglutide did not appear to affect growth or pubertal development during the trial period”
My take: As in adults, treatment with semaglutide results in weight loss.
The drug, called tirzepatide, works on two naturally occurring hormones that help control blood sugar and are involved in sending fullness signals from the gut to the brain...Those taking the highest of three studied doses lost as much as 21% of their body weight – 50-60 pounds in some cases…
Another obesity treatment approved last year called semaglutide, from Novo Nordisk, provides an average of up to about 15% weight loss. Previous generations of diet drugs cut only about 5% of weight and many carried prohibitive side effects…
About 15% of participants who received the active drug dropped out of the 72-week trial, about a third because of gastrointestinal side effects. Twenty-six percent of trial volunteers who received a placebo dropped out.
On May 13, the Food and Drug Administration approved tirzepatide, under the trade name Mounjaro, for the treatment of Type 2 diabetes…The new tirzepatide trial, called SURMOUNT-1, included more than 2,500 volunteers [without diabetes]…Nine out of 10 lost weight, and on the highest dose, 15 mg, they lost an average of 52 pounds each...
It’s too soon to know what price Lilly will set for tirzepatide. Mounjaro, the same drug used to treat diabetes at the same doses, retails for almost $1,000 a month…Semaglutide went on the market last year for weight loss and has been in short supply ever since, Rind said. It costs about $1,600 a month for the 2.4 mg weight loss dose, which is higher than the 1 or 2 mg doses used to treat diabetes. Like other weight loss drugs, semaglutide isn’t covered by many insurance plans.
My take: This therapy, already approved for Type 2 Diabetes, appears promising for obesity but costly. More time will be needed to understand the safety profile with extended use.
Retrospective study: 582 children had NGTs secured traditionally and 173 received nasal bridles
Key findings:
Children with bridled NGTs were compared to their non-bridled NGT counterparts (all results below with p values <0.02):
16.67 times less likely to experience ≥1 dislodgement (OR=0.06)
2.5 times less likely to have one more ED visit (OR=0.4)
4.76 times less likely to require one more radiographic exposure (OR=0.21)
My take: After learning about bridles at N2U in 2015 (thanks Praveen Goday), they quickly became popular in our institution. They improve NG/NJ outcomes.
Bridle Link –Youtube: AMT Bridle (~3 minutes with adult model). Bridle can be placed with NG or NJ in place.
AMT bridle website -includes full length video, family brochure, and at length description
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition