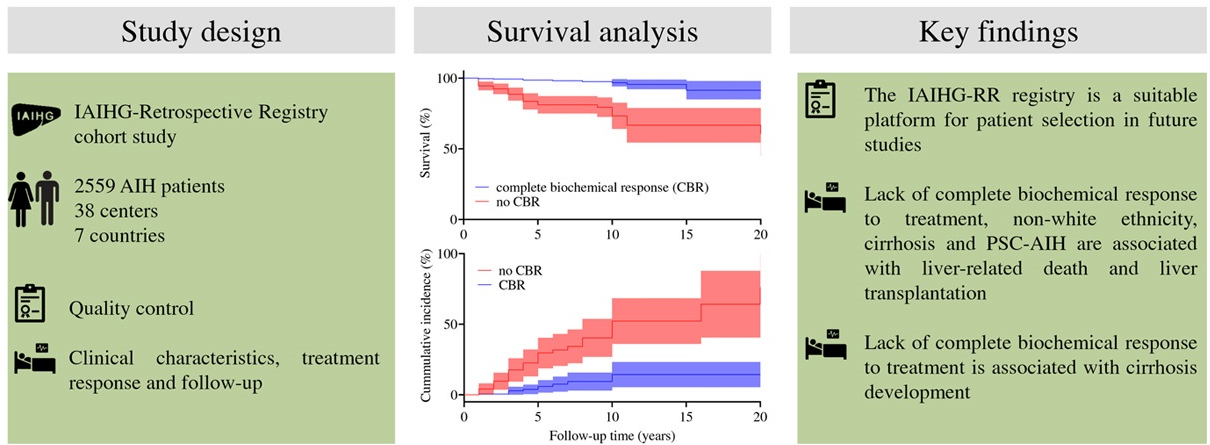
- CD Slooter et al. Hepatology 2024; 79: 538-550. Lack of complete biochemical response in autoimmune hepatitis leads to adverse outcome: First report of the IAIHG retrospective registry
- G Cholankeril, JM Vierling. Hepatology 2024; 79: 529-531. (Editorial) Open Access! The clinical imperative of a complete biochemical response to immunosuppression in autoimmune hepatitis: Close is not good enough!
“Close don’t count in baseball. Close only counts in horseshoes and hand grenades.” –Frank Robinson 1973.
This study used the the International Autoimmune Hepatitis Group retrospective registry (IAIHG-RR), a web-based platform. This retrospective, observational, multicenter study analyzed 2559 patients; however, only 1700 had adequate follow-up. A complete biologic response (CBR) was defined as normalization of aminotransferases and serum IgG within 6 months; only 706 had serial results of these parameters to assess for a CBR.
Key findings:
- Among the 706 with adequate data, 68.5% achieved a CBR.
- Non-White ethnicity (HR 4), cirrhosis (HR 3.5), variant syndrome with primary sclerosing cholangitis (PSC) (HR 3.1), and lack of complete biochemical response within 6 months (HR 5.7) were independent prognostic factors.
- Patients with a CBR had a greater actuarial survival over a 20-year period (91%) compared to those without a CBR (61%). Lack of a CBR at 6 months conferred a 3.6-fold higher risk of progression to cirrhosis.
- Even in patients with cirrhosis, a CBR increased long-term survival: 82% versus 34%.
My take: A CBR is associated with the best long-term outcomes. My suspicion is that a biochemical response is actually similar to horseshoes. Improvement with treatment is likely beneficial but not as good as hitting the stake (the target).
Related blog posts:
- Autoimmune Hepatitis -Early Response Associated with Remission
- Autoimmune Hepatitis: Safety of Low Dose Steroids and Utility of Aminotransferases
- Predicting Outcomes in Childhood Autoimmune Hepatitis
- Why It Is Hard to Stop Immunosuppression with Autoimmune Hepatitis and Lower Bone Density with Fatty Livers
- Is It a Mistake to Use Budesonide for Autoimmune Hepatitis?
- What to Do with Refractory Autoimmune Hepatitis: Case Report
- Slim Pickings: Data for 2nd-Line Autoimmune Hepatitis Pediatric Therapy
- Online Aspen Webinar -COVID-19, Autoimmune Hepatitis (Part 8)