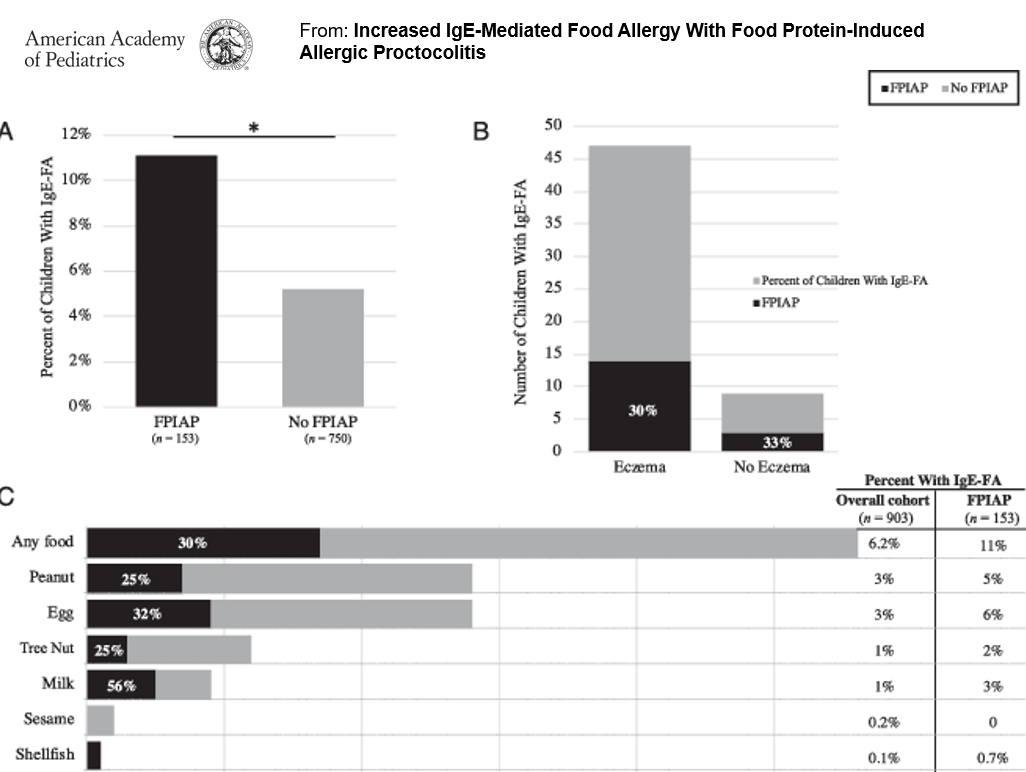
In this study of 153 infants with food protein-induced allergic proctocolitis (FPIAP) with documented blood in the stool, more children with FPIAP developed IgE-Food Allergy (IgE-FA) (11%) compared with healthy children.
Key points (from commentary by MT Kraft and D Stukus):
“Although conventional teaching is to wait until 12 months of age to reintroduce dairy to infants with FPIAP, it can likely be introduced much earlier.”
The diagnosis of FPIAP was associated with with an increased risk of IgE-FA, “although diagnosis was not confirmed through oral food challenges”
My take: Children with FPIAP are more likely to receive a diagnosis of IgE-FA. Prolonged restriction of milk, when no longer required, could contribute to this; in addition, some children are mislabeled as food allergic without appropriate confirmation (based on faulty testing).
“Major changes to the Georgia WIC Program effective today, announced by the @GaDPH & @GAChapterAAP, most importantly, a new WIC Request for Medical Formulas & Supplemental Foods (RMF) form replacing the MDF.”
Advances in Cystic Fibrosis (CF) have led to improvement in longevity, now ~46 years in 2019
Newer CFTR modulator therapies need to be aligned to the specific mutations. With new therapies, a high calorie diet may not be required and instead follow a standard healthy balanced diet.
These agents appear to be driving a big drop in hospitalizations
Now some patients need counseling for obesity and NAFLD
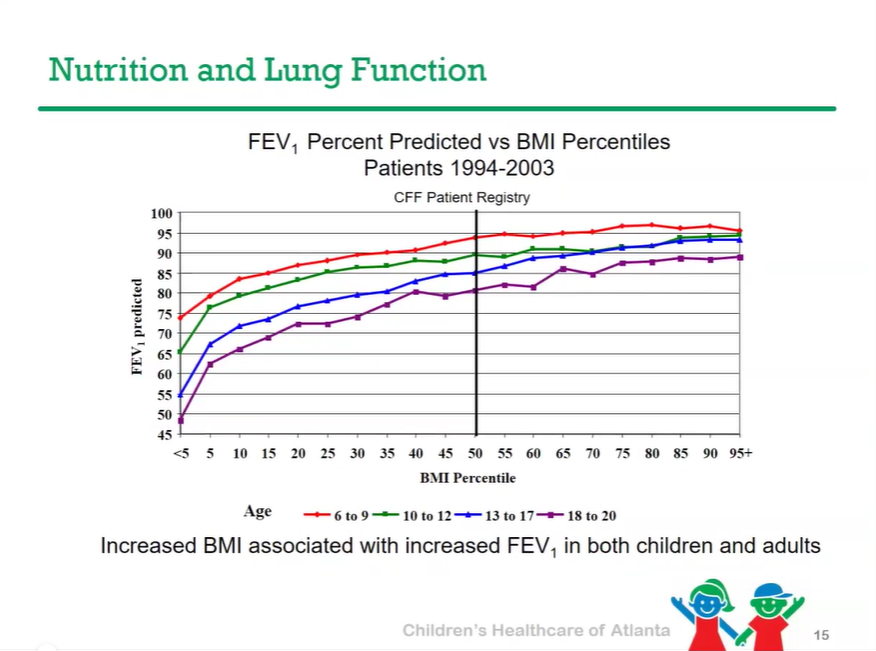
Better nutrition has been linked to better lung outcomes.
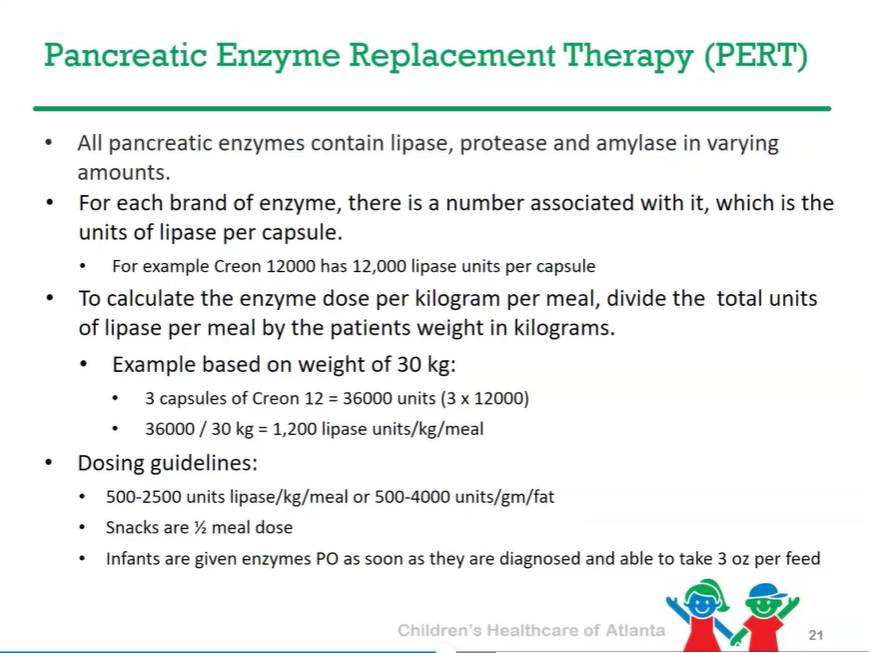
Pancreatic enzyme replacement therapy needed for 85-90% of patients with CF
CFTR modulator therapies may allow lower dosing PERT dosing
Fat soluble vitamin supplementation (A, D, E, K) is needed
Vitamin D (25-OH) goal (by CF Foundation) is >30 ng/mL
High salt diet is recommended due to excessive losses
Targeted nutritional support needs to be based on nutritional status; some patients may need G-Tube placement. CHOA algorithm developed.
High sugar diet may increase the development of CF related diabetes (CFRD)
Fibrosing colonopathy is a very rare effect of high dose pancreatic enzymes and may have been in part due to impurities in older preparations of panrcreatic enzymes.
As noted in previous blog posts (see below), allergy testing can lead to unnecessary food restrictions which can in turn lead to numerous subsequent problems. Case in point: YV Virkud et al (NEJM 2020; 383: 2462-2470) report on A 29-Month-Old Boy with Seizure and Hypocalcemia
This boy presented with severe hypocalcemia, rickets, and seizures one year after allergy testing led to additional dietary restrictions. Also, his mother was a vegetarian. At time of allergy testing, IgE testing suggested allergies to milk, cashews, pistachios, egg whites, almonds, soybeans, chickpeas, green peas, lentils, peanuts, and sesame seeds. Many of these foods caused no symptoms with food challenges.
Besides working through the potential reasons for hypocalcemia, the authors make several key points:
Nutritional rickets is NOT a historical relic. Vitamin D deficiency appears to be increasing in high-income countries despite food-fortification strategies.
There are frequent misdiagnosis of food allergies. “Clinical and laboratory testing is severely limited by poor specificity…approximately 20 to 25% of children have positive IgE blood tests to specific food allergens, even though the true prevalence of IgE-mediated food allergy is likely closer to 6 to 8%.”
Avoid indiscriminate use of IgE blood testing. Allergen panels are “particularly problematic, because they often uncover false positives and lead to unnecessary food avoidance.” Individual IgE testing can be used to help confirm a diagnosis after an allergic reaction to a food trigger.
The most accurate diagnostic tool is an oral food challenge.
In children with food allergies, supplements are often needed to avoid micronutrient deficiencies and a low threshold is needed for involvement of dieticians.
Early introduction of foods can reduce incidence of allergies and periodic reassessment is needed to determine if a child has outgrown an allergy.
Xrays show generalized demineralization. The metaphyses show flaring (dashed arrow) and cupping (arrowbead). The physes are radiolucent and widened (asterisks).
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition
I want to thank all of you who take an interest in my blog, particularly those who give suggestions, references, and encouragement. The following posts were the most popular from the past year.
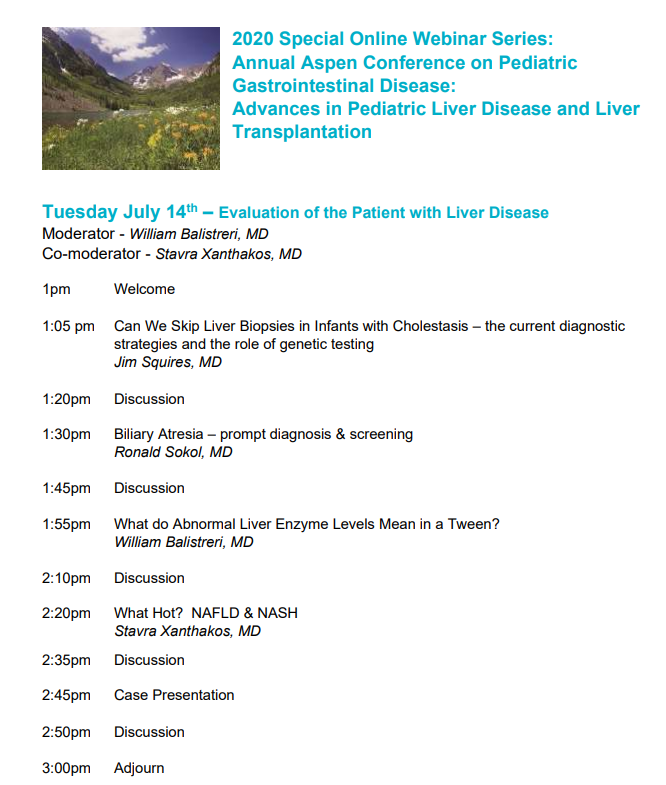
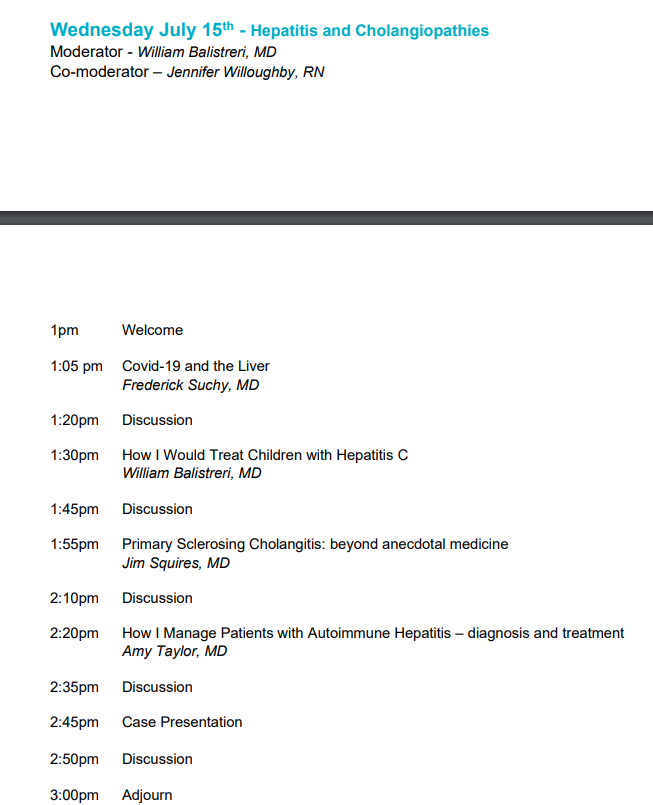
This year I had planned to go back to what many consider the best learning conference in our field, the Annual Aspen Conference. This conference alternates yearly between GI topics and liver topics. What has made this conference so great:
Intimate setting
Terrific faculty
Chance to enjoy the surroundings with friends and families after the lectures
Due to the pandemic, this year’s course will be curtailed and online. While this changes the setting, it is still a great opportunity and a heck of a lot easier to attend. It will take place 1:00-2:30 pm Tues, Weds, and Thurs next week (July 14-16). You can register for a day or for all 3 days. Course description and faculty are listed below.
Also, there is a pre-conference SCAVENGER HUNT. (This appears to be mainly to help with promotion of the conference sponsors.) By participating, attendees will be eligible for raffle prizes awarded during the webinar:
• Snowmass Camelback
• Snowmass Winter Gloves
• Snowmass Hat
• Snowmass Socks
The GRAND PRIZE is FREE 2021 CONFERENCE REGISTRATION!