Full Text: JD Feuerstein et al. Gastroenterol 2020; 158: 1450-61. AGA Clinical Practice Guidelines on the Management of Moderate to Severe Ulcerative Colitis
Full Tex PDF: AGA Clinical Practice Guidelines on the Management of Moderate to Severe Ulcerative Colitis
Associated articles included the following:
- Clinical decision support tool (1462-63)
- PDF: Spotlight (summary -images above) (1464)
- Technical Review (1465-96)
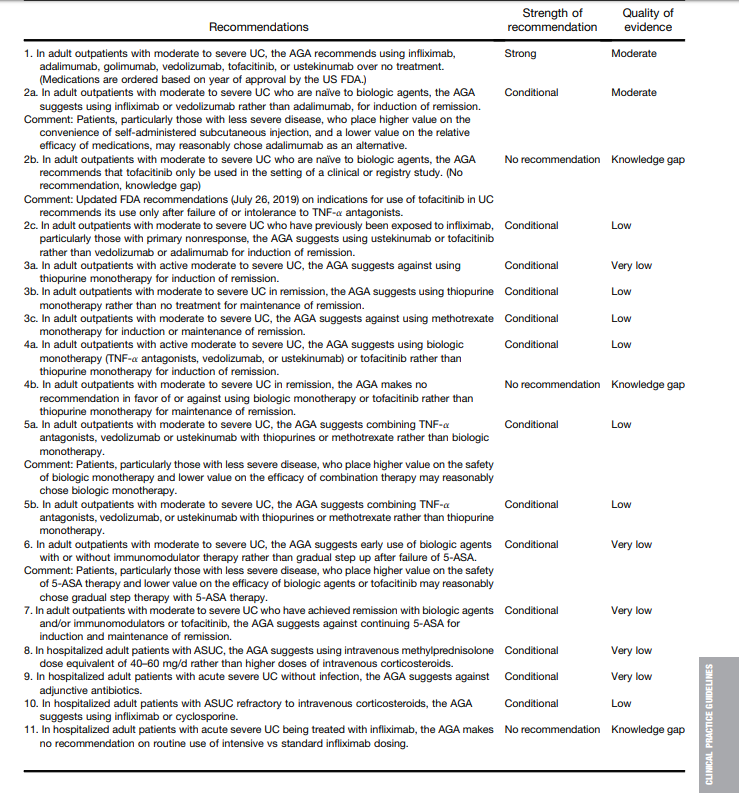
Key recommendations:
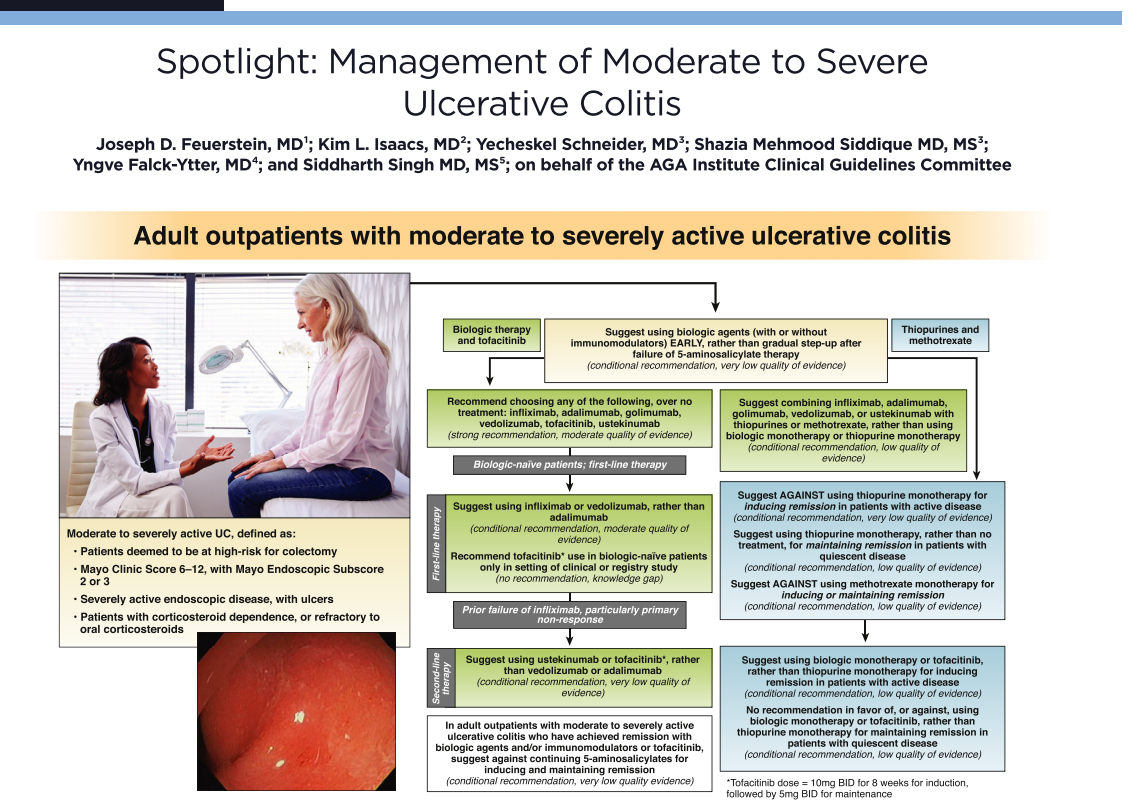
- 2a. In adult outpatients with moderate to severe UC who are naïve to biologic agents, the AGA suggests using infliximab or vedolizumab rather than adalimumab, for induction of remission. Comment: Patients, particularly those with less severe disease, who place higher value on the convenience of self-administered subcutaneous injection, and a lower value on the relative efficacy of medications, may reasonably chose adalimumab as an alternative
- 2c. In adult outpatients with moderate to severe UC who have previously been exposed to infliximab, particularly those with primary nonresponse, the AGA suggests using ustekinumab or tofacitinib rather than vedolizumab or adalimumab for induction of remission.
- 6. In adult outpatients with moderate to severe UC, the AGA suggests early use of biologic agents with or without immunomodulator therapy rather than gradual step up after failure of 5-ASA. Comment: Patients, particularly those with less severe disease, who place higher value on the safety of 5-ASA therapy and lower value on the efficacy of biologic agents or tofacitinib may reasonably chose gradual step therapy with 5-ASA therapy.
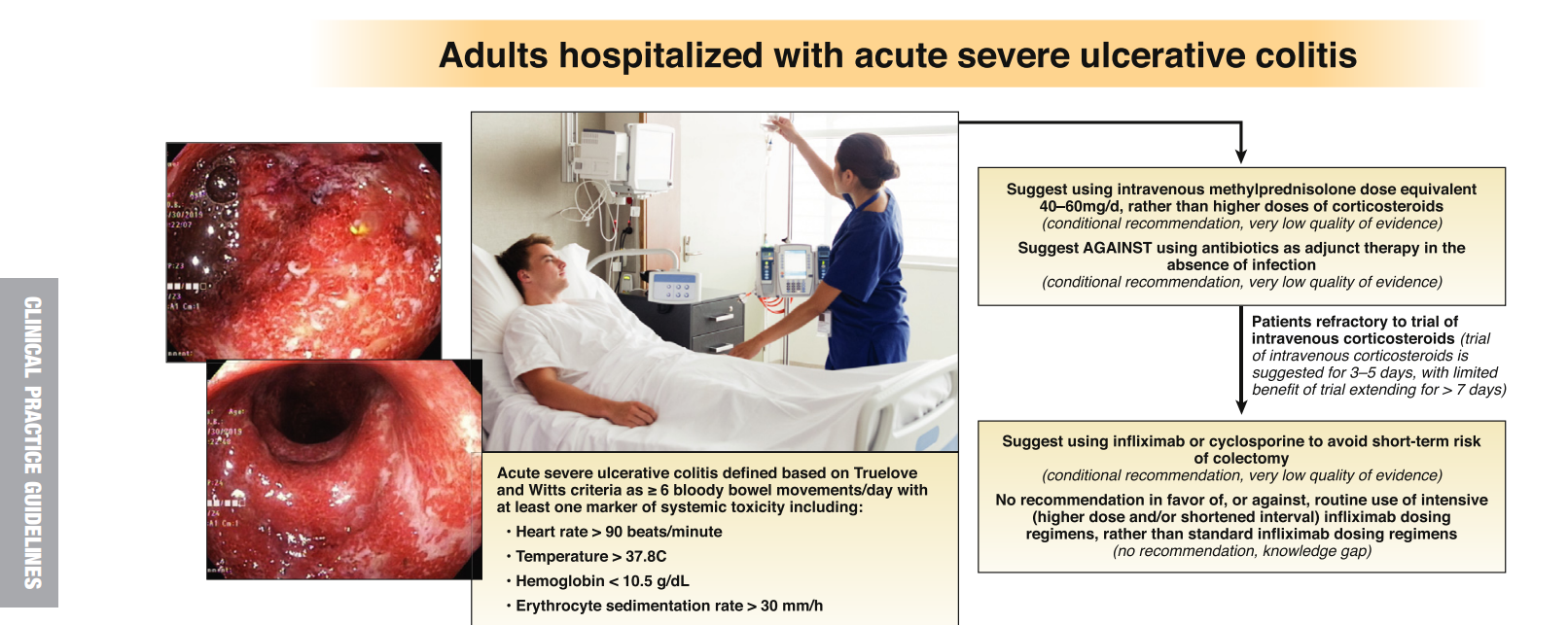
- 10. In hospitalized adult patients with ASUC refractory to intravenous corticosteroids, the AGA suggests using infliximab or cyclosporine
Summary of recommendations:
Related blog posts:
- AGA Guidelines for Mild to Moderate Ulcerative Colitis
- Toronto Consensus: Practice Guidelines for Nonhospitalized Ulcerative Colitis
- Is There Renal Toxicity with Mesalamine Therapy for IBD? | gutsandgrowth
- FDA Warning on Tofacitinib | gutsandgrowth
- “Tofacitinib: A Jak of All Trades” | gutsandgrowth
- Real-World Vedolizumab: Better Than Expected
- IBD Highlights from Recent Meetings with Commentary by Dr. Sandborn Explains Why Vedolizumab Should Be Considered a First Line Agent (2019)
- Vedolizumab vs Adalimumab for Infliximab Failure in Ulcerative Colitis –Which is Better?
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition