R Greywoode et al. Inflamm Bowel Dis 2023; 29: 843-849. Open Access! Racial Difference in Efficacy of Golimumab in Ulcerative Colitis
The authors analyzed pooled individual-level data (n=1066) from induction and maintenance trials of golimumab in adults with moderate-to-severe UC. Key findings:
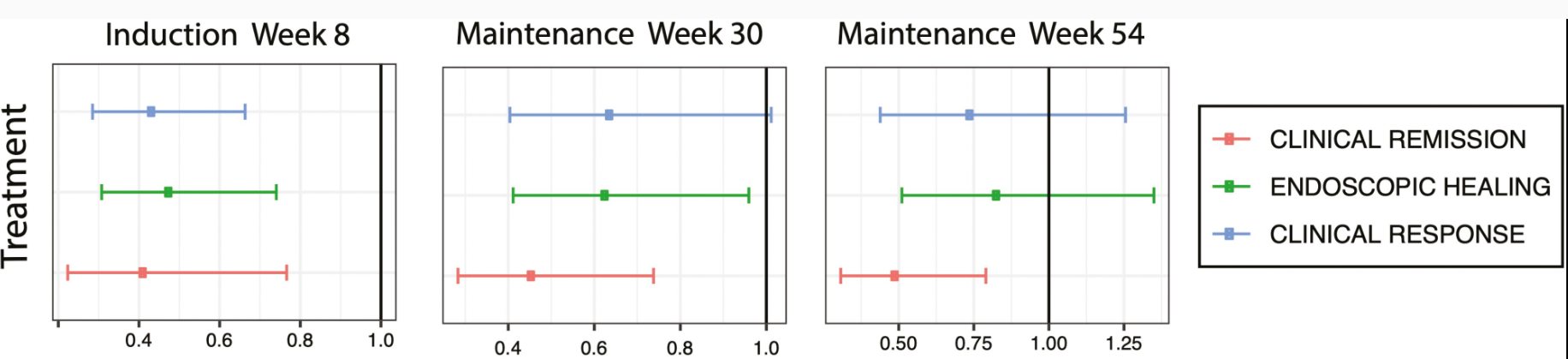
- Compared with White participants, participants from racial minority groups had significantly lower clinical response (adjusted odds ratio [aOR], 0.43), clinical remission (aOR, 0.41), and endoscopic healing (aOR, 0.48) at week 6.
- Participants from racial minority groups also had significantly lower clinical remission (aOR, 0.46) and endoscopic healing (aOR, 0.63) at week 30.
- There were no racial differences in placebo response rates.
Discussion:
This is a fascinating study. Most of the differences in response to IBD treatment have been attributed to social determinants of health including access to care (geography, insurance), and adherence to medical care. This study implicates biological factors rather than social factors for driving the difference in response. “There is also a growing body of research uncovering differences in the frequencies of genetic variants in diseases, which may contribute to differences in observed health outcomes among divergent ancestral populations.32,33“
“One of the challenges in further understanding how race may affect response to IBD biologic drugs is the relatively small number of participants from racial minority groups included in clinical trials. There is a longstanding disparity in clinical trial participation in the United States, whereby racial and ethnic minority groups have disproportionately low representation.34-37“
While the differences in the disease phenotype may account for the response to treatment, there may be other factors as well. With hepatitis C infection, those of us who remember the frequent use of Peg-interferon therapy will recollect that specific mutations in Interleukin-28B (IL28B) gene predicted lower response rates in African-American populations (related post: Understanding IL28B).
My take: Most of the changes in outcomes to treatment are likely driven by socioeconomic factors. This study is a good reminder that biological factors play a big role as well.