A recent study (JM Boster, M Iwanowski, RE Kramer. JPGN 2021; 72: 250-254. Management of Pediatric Postendoscopy Fever: Reducing Unnecessary Health Care Utilization With a Clinical Care Guideline) provides clear guidance for how to handle post-procedure fevers.
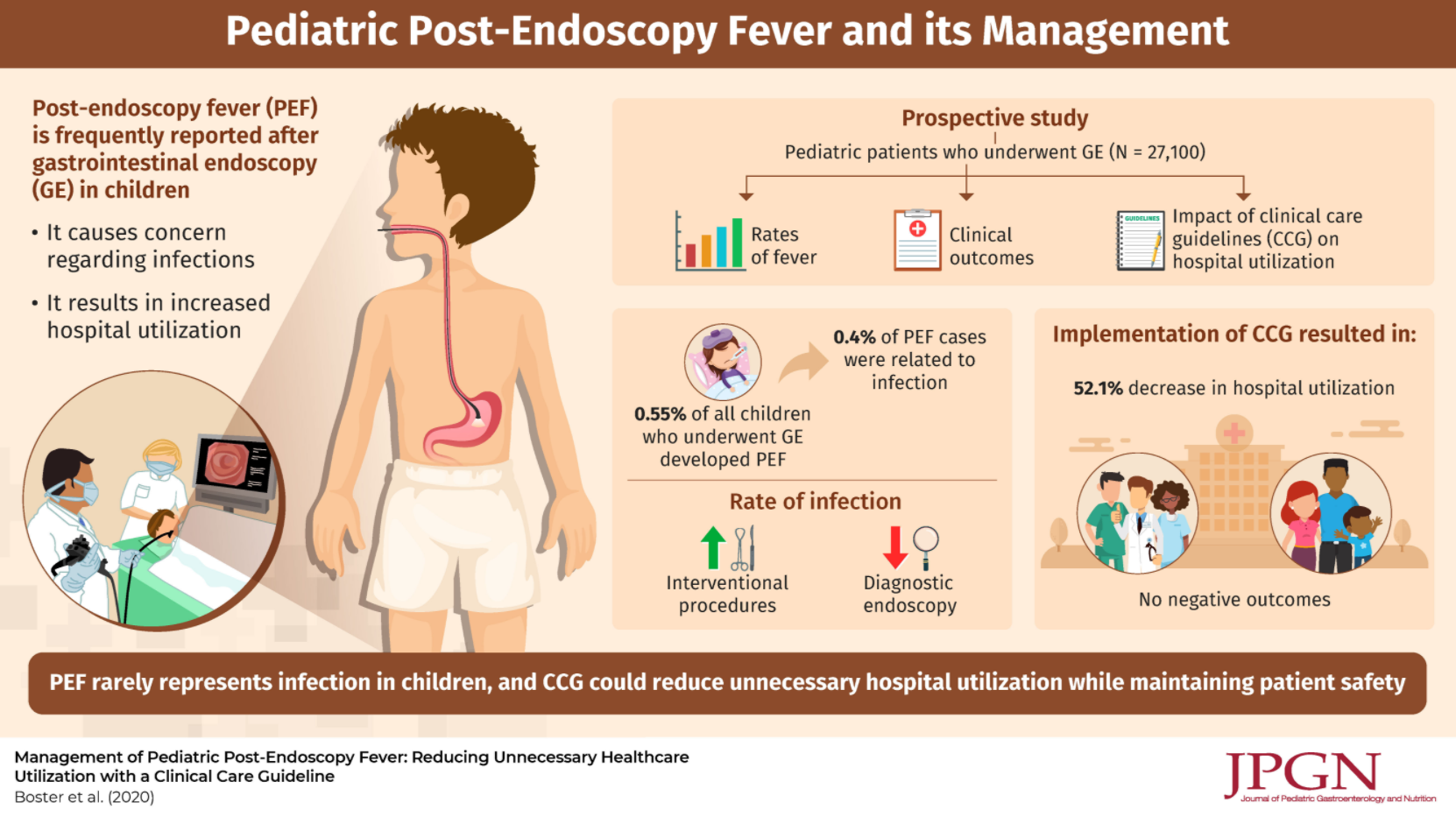
Using a prospective database with 27,100 endoscopies, the authors evaluated a clinical care guideline to reduce unnecessary medical care following endoscopy.
Key findings:
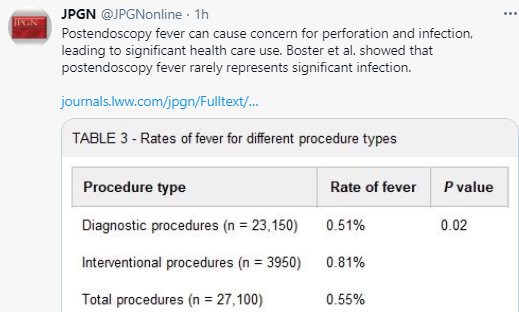
- Post-endoscopy fever (PEF) occurred in 0.55% (n=150)
- ONLY 6 of these 150 PEFs (0.4%) were attributed to a procedure complication: 3 had perforations (all with abdominal pain), 2 had aspiration (both had emesis at time of endoscopy) and 1 had a positive blood culture (though had undergone a liver biopsy as well as endoscopy)
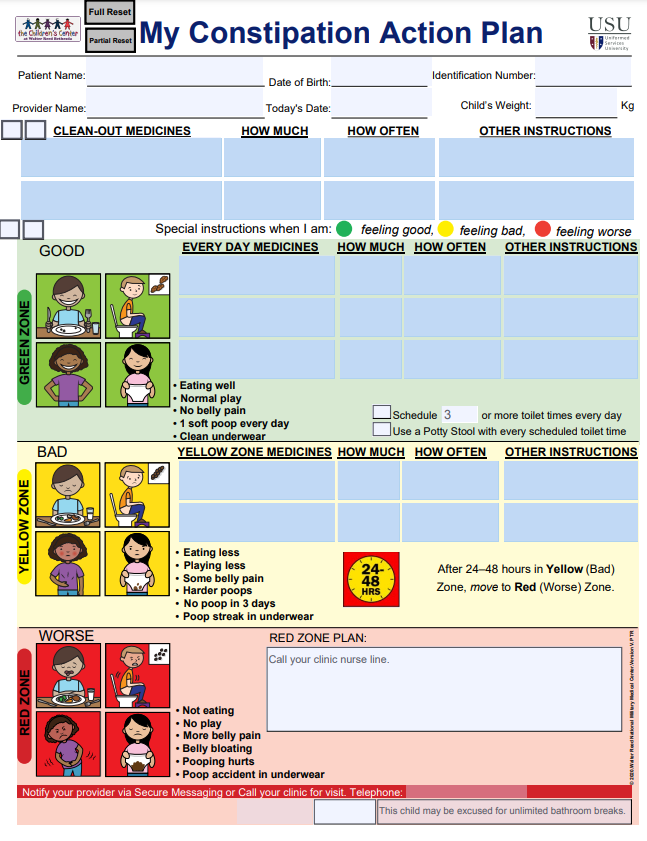
- The authors published their care guideline (Figure 1) which stratifies risk based on whether the procedure was an interventional (high risk) vs diagnostic (low risk), ASA class, duration of fever, concomitant immunosuppression (eg. steroids), and associated symptoms including vomiting, diarrhea, bleeding, new abdominal pain, impact on activities of daily living, and hydration
- Interestingly, the authors note that their cohort had a total of 23 perforations, but only 3 presented with fever
- Using the care guideline resulted in a “significant shift in the prevalence of Grade 2 and above (requiring hospital use) to Grade 1 (clinical observation and reassurance) adverse events, dropping ED visits and admissions by 43.6% and 76.4% respectively for the post-endoscopy fever patients.” This shift was not associated with any observed negative patient outcomes or missed diagnoses.
My take: The authors note that fever is often related to release of inflammatory cytokines which can occur with endoscopy in the absence of complications. The authors methodical guideline to post-procedure fever provides a logical approach to this common problem.
Related blog posts:
- Adverse Events Following Pediatric Endoscopy –Underestimated Previously
- Our Study: Provider Level Variability in Colonoscopy Yield
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.