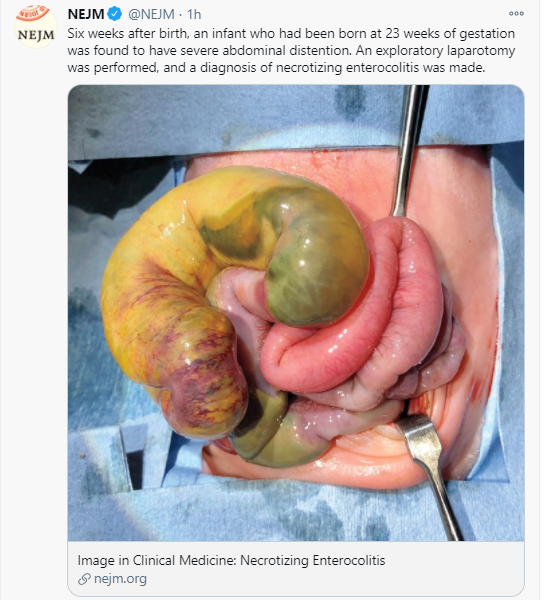
Y Li et al. J Pediatr 2020; 227: 128-134. Early Use of Antibiotics Is Associated with a Lower Incidence of Necrotizing Enterocolitis in Preterm, Very Low Birth Weight Infants: The NEOMUNE-NeoNutriNet Cohort Study
Methods: This study used the NEOMUNE-NeoNutriNet cohort of VLBW infants from 13 neonatal intensive care units (NICUs) in 5 continents (n = 2831). NEC incidence was compared between infants who received early antibiotics and those who did not.
Key finding:
- The incidence of NEC was 9.0% in the group of infants who did not receive early antibiotics (first 72 hrs) (n = 269), compared with 3.9% in those who did receive early antibiotics (n = 2562)
This type of study is inherently difficult due to measured and unmeasured confounders. In a related commentary, Joseph Cantey (Early Antibiotic Therapy and Adverse Outcomes in Preterm Infants: Time for a Trial!, https://doi.org/10.1016/j.jpeds.2020.07.046) notes that some previous studies have shown an association of antibiotics with increased risk of NEC, presumably due to a selection bias (eg. sicker patients getting antibiotics). Fortunately a randomized prospective trial is underway, the NICU Antibiotics and Outcomes (NANO, NCT03997266). This should help determine more carefully the risks and benefits of antibiotics in this vulnerable population.
My take: We have a lot to learn about modulating the premature infant’s microbiome to prevent necrotizing enterocolitis.
Related blog posts:
- Probiotics -Another Positive Study for Prevention of NEC
- Probiotics For NEC -More Work is Needed (part 1 …
- Probiotics for NEC -More Work is Needed (part 2 …
- Therapeutic Inertia in US Neonatal Units (vis-a-vis Probiotics)
- Potential and pitfalls of probiotics with necrotizing enterocolitis
- Lactobacillus rhamnosus GG Associated with Increased Necrotizing Enterocolitis in Observational Study