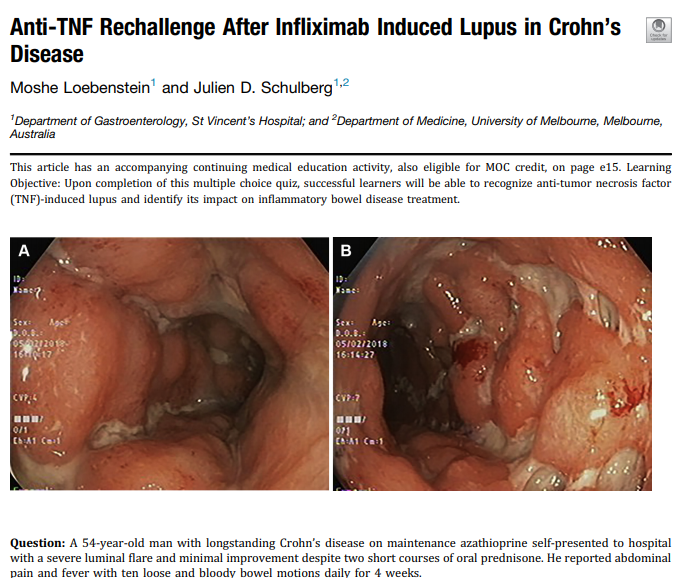
Emilio J. Laserna‐Mendieta et al. AP&T 2020; https://doi.org/10.1111/apt.15957. Full article link: Efficacy of proton pump inhibitor therapy for eosinophilic oesophagitis in 630 patients: results from the EoE connect registry
“This cross‐sectional study collected data on PPI efficacy from the multicentre EoE CONNECT database.” Overall, 630 patients (76 children) received PPI as initial therapy (n = 600) or after failure to respond to other therapies (n = 30)
Key findings:
- PPI therapy achieved eosinophil density below 15 eosinophils per high‐power field in 48.8% and a decreased symptom score ≥50% from baseline in 71.0% of patients.
- More EoE patients with an inflammatory rather than stricturing phenotype accomplished clinico‐histological remission after PPI therapy (OR 3.7; 95% CI, 1.4‐9.5)
- PPI treatment is more effective in achieving clinico‐histological remission of the disease when used in higher instead of standard or lower doses (50.8% vs 35.8%), and when the duration of therapy is prolonged from 8 to 12 weeks (50.4% vs. 65.2%)
My take: This study confirms previous studies which have generally found that PPIs are effective in 40-50% of patients with eosinophilic esophagitis. Higher doses of PPIs are needed to achieve the highest response rates.
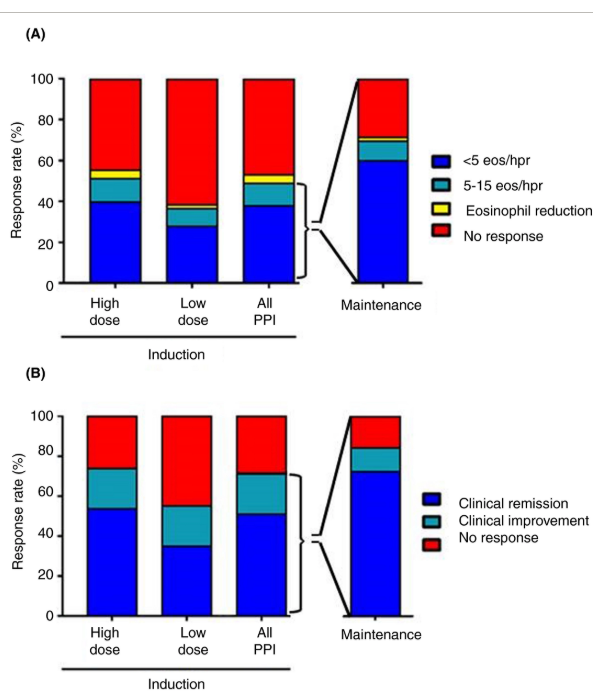
“Bar chart for histological (A) and symptomatic (B) responses for proton pump inhibitor (PPI) mono‐therapy to induce and maintain remission in patients with eosinophilic oesophagitis. For induction of remission, patients were classified according to the PPI dosage prescribed: high dose was double dosage or higher, and low dose was standard dosage or lower. For maintenance therapy, only patients with dosage reduction from that used for induction were included. eos/hpf: eosinophils per high power field”
Related blog posts:
- How Genetics Influence Response to PPIs in Eosinophilic Esophagitis
- New Therapy for Eosinophilic Esophagitis | gutsandgrowth
- Could Immunotherapy (EPIT) Work For Eosinophilic Esophagitis? & Coronavirus Up-to-Date Tally | gutsandgrowth
- Negligible Effect of Eosinophilic Esophagitis Treatment on Longitudinal Growth
- Increased Risk of EoE with TEF/EA
- What is EoE?
- EoE Update 2018 (Dr. Seth Marcus)
- Updated Consensus Guidelines for Eosinophilic Esophagitis