N Kristof, NY Times (1/24/23): A Smarter Way to Reduce Gun Deaths
Some excerpts:
In 2021 a record 48,000 Americans were killed by firearms, including suicides, homicides and accidents. So let’s try to bypass the culture wars and try a harm-reduction model familiar from public health efforts to reduce deaths from other dangerous products such as cars and cigarettes.
Harm reduction for guns would start by acknowledging the blunt reality that we’re not going to eliminate guns any more than we have eliminated vehicles or tobacco, not in a country that already has more guns than people.
Recommendations from article:
- We can try to keep firearms from people who are under 21 or who have a record of violent misdemeanors, alcohol abuse, domestic violence or some red flag that they may be a threat to themselves or others
- To keep ineligible people from buying firearms, we need universal background checks
- A pillar of harm reduction involving motor vehicles is the requirement of a license to drive a car. So why not a license to buy a gun?… In Massachusetts, which has one of the lowest gun mortality rates in the country, an applicant who wants to buy a gun must pay $100 for a license, be fingerprinted, undergo a background check and explain why he or she wants a gun. If the permit is granted, as it typically is after a few weeks, the bearer can then go to a gun store and buy the firearm. There is then an obligation to store it safely and report if it is stolen.
- Smoking and alcohol cause more deaths in U.S. –both are regulated, not banned. “Because we’ve worked to reduce vehicle deaths and haven’t seriously attempted to curb gun violence, firearms now kill more people than cars.”
- Background checks to purchase ammunition… this should be possible without creating burdens for gun owners who have already gone through background checks to buy weapons
- Waiting periods and limits on how many guns one can purchase at a time may also help. We also need to crack down on untraceable ghost guns and on firearms made by 3-D printers; ghost guns are already a growing source of weapons for criminals
- Warning labels: One proposed ammunition label has a photo of a bloody face and states that a gun increases the risk of someone in a home being killed
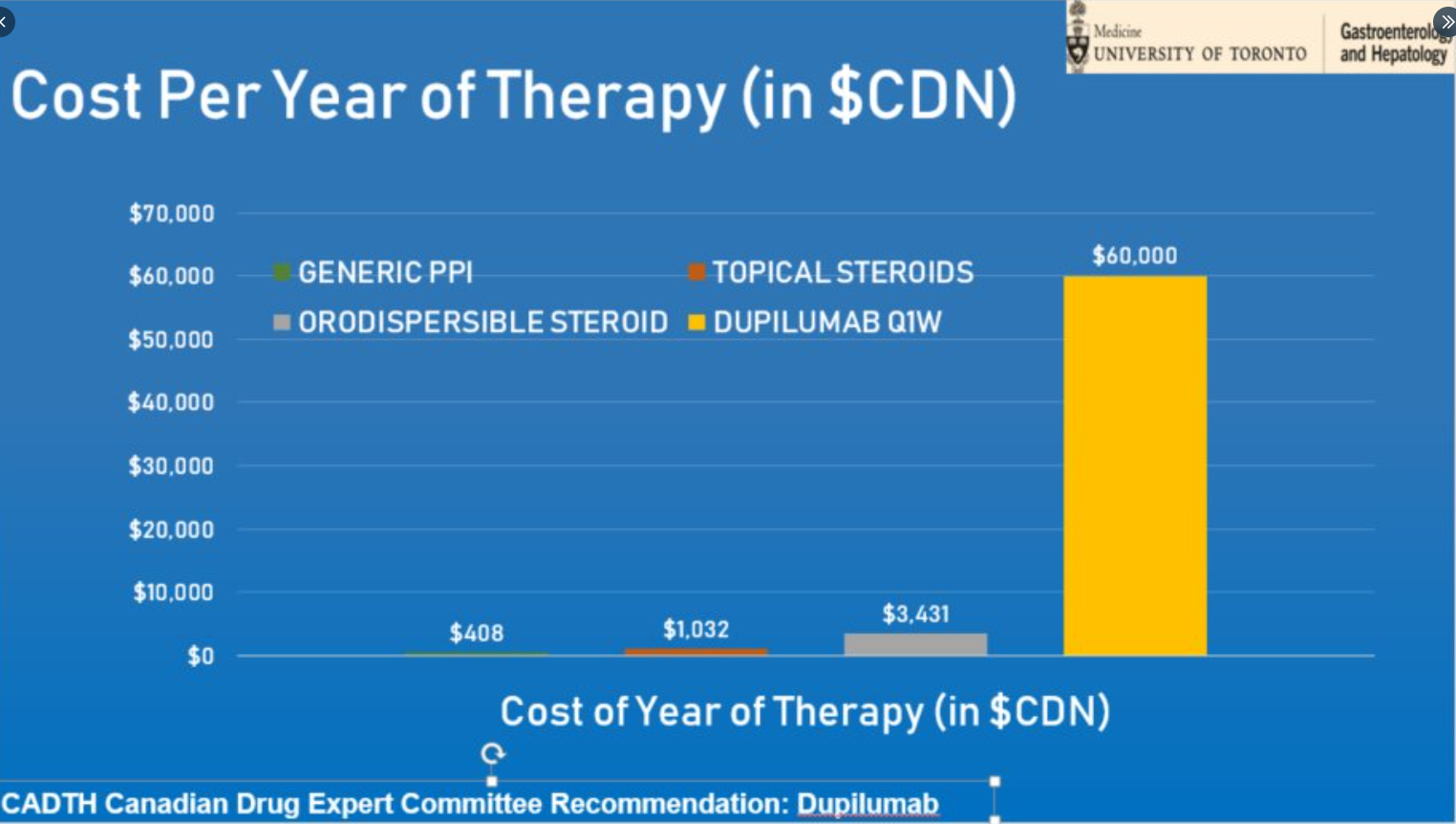
- Increase costs of ownership to cover the damage associated with weapons: raise cost of guns through taxes/fees
This article proposes a lot of practical interventions that if implemented would likely reduce gun violence.
Related article: NPR Jan 24, 2023: Gun violence deaths: How the U.S. compares with the rest of the world The chart below shows how the U.S compares to gun violence in countries with low levels of gun violence. The U.S. compares favorably with Mexico, El Salvador, Guatemala, Venezuela, The Phillipines and Iraq. However, many violent places have lower gun violence than U.S. including Syria, Somalia, Afganistan, Iran, Pakistan, Yemen, and Libya.
Related blog posts:
- The Harms from the Supreme Court’s Bruen Decision
- “Crossing Lines” and Why Firearm Deaths are The Leading Cause of Death in Children
- No Exaggeration: Too Many Children Are Dying in the U.S. “The sad fact is that a child or adolescent in the United States is 57% more likely to die by the age of 19 years than those in other wealthy nations.” This is due mainly to more deaths from MVAs and from gun violence.
- Firearms: #1 Cause of Pediatric Deaths & Households with Guns =More Deaths includes link to AAP toolkit/advocacy
- How the U.S. Compares in Rate of Gun Violence Deaths
- Gun Violence –What Will It Take To Change Anything?
- More Guns in Georgia, More Bad Outcomes
- Gun Carrying Adolescents –Why We Are Going to See More School Shootings

Atlanta Botanical Gardens
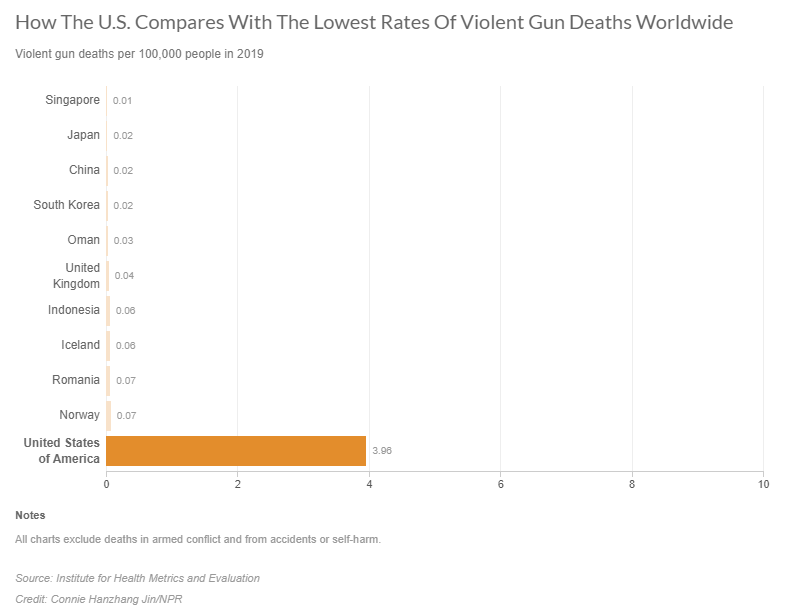
From NPR article.
Aslo, gun violence is widespread and is more common in ‘red’ states than ‘blue’ states despite the widely-held notion that gun violence occurs mainly in large urban centers.
Axios 1/27/23: Not an anomaly: 2020’s red states have higher murder rates Murder rates in red states have outpaced blue states by an average of 23% over the past two decades.